Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
GANGGUAN PANKREATOBILIER
Dr Willy B Uwan, MARS, SpPD, K-GEH, FINASIM SMF Penyakit Dalam Klinik Penyakit Hati dan Saluran Cerna Unit Endoskopi Diagnostik dan Terapeutik RSU St Antonius Pontianak

2
Pankreatitis Akut Definisi
Peradangan akut, non-bakterial pada organ pankreas. Patofisiologis Terjadinya pankreatitis akut diawali karena adanya jejas di sel asini pankreas akibat: Obstruksi duktus pankreatikus (terutama oleh migrasi batu empedu) Stimulasi hormon cholecystokinin (CCK) sehingga akan mengaktifasi enzim pankreas (misalnya karena pengaruh hipertrigliseridemia dan alkohol) Iskemia (misalnya pada pankreatitis akut paska prosedur endoscopic retrograde cholangiopancreatography / ERCP atau atherosklerosis)
 Stimulasi hormon cholecystokinin (CCK) sehingga akan mengaktifasi enzim pankreas (misalnya karena pengaruh hipertrigliseridemia dan alkohol) Iskemia (misalnya pada pankreatitis akut paska prosedur endoscopic retrograde cholangiopancreatography / ERCP atau atherosklerosis)")
3
Etiologi Beberapa penyebab pankreatitis akut adalah:
Obstruksi batu di duktus koledokus (38%) Alkohol (36%) Pankreas divisium (7%) Komplikasi paska tindakan ERCP (5,4%) Hipertrigliseridemia (1-4 %) Obat-obatan (1-4 %) Hiperkalsemia Pankreatitis akut idiopatik (10-15 %)
 Alkohol (36%) Pankreas divisium (7%) Komplikasi paska tindakan ERCP (5,4%) Hipertrigliseridemia (1-4 %) Obat-obatan (1-4 %) Hiperkalsemia. Pankreatitis akut idiopatik (10-15 %)")
4
ETIOLOGY Gallstones, microlithiasis, biliary sludge
Ethanol (5 years, > 50g/day), ERCP Toxins, tumors, trauma Steroids and ulcers Mumps and other infections Autoimmune Stenosis (sphincter of Oddi dysfunction, papillary stenosis) Hypertriglyceridemia, hypercalcemia, hypothermia Genetic (<30 years old, family history) Drugs (Azathioprine, estrogen, HIV drugs, tetracycline, sulfa
, ERCP. Toxins, tumors, trauma. Steroids and ulcers. Mumps and other infections. Autoimmune. Stenosis (sphincter of Oddi dysfunction, papillary stenosis) Hypertriglyceridemia, hypercalcemia, hypothermia. Genetic (<30 years old, family history) Drugs (Azathioprine, estrogen, HIV drugs, tetracycline, sulfa.")
5
Fase Pankreatitis Akut
Pada umumnya perjalanan klinis pankreatitis akut dapat dibagi: Fase awal Fase awal terjadi pada minggu pertama, ditandai dengan adanya systemic inflammatory response syndrome / SIRS Fase lambat Fase lambat berlangsung beberapa minggu sampai bulan dan ditandai dengan adanya SIRS yang persisten atau oleh karena komplikasi lokal dari pankreatitis akut.

6
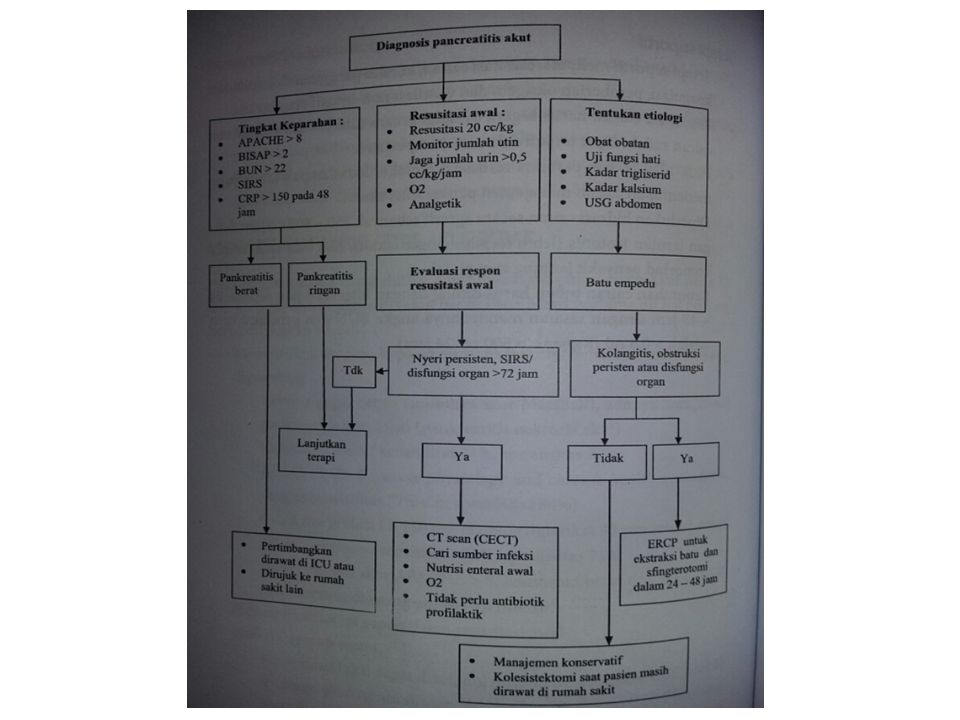
Diagnosis Diagnosis pankreatitis akut ditegakkan berdasarkan:
Anamnesis Pemeriksaan fisik Laboratorium Pemeriksaan imaging Menurut klasifikasi Atlanta (2012), diagnosa pankreatitis akut tegak bila memenuhi 2 dari 3 kriteria berikut: Nyeri perut bagian atas Peningkatan amilase atau lipase > 3x nilai batas atas normal Pemeriksaan imaging (USG / CT scan atau MRI)
, diagnosa pankreatitis akut tegak bila memenuhi 2 dari 3 kriteria berikut: Nyeri perut bagian atas. Peningkatan amilase atau lipase > 3x nilai batas atas normal. Pemeriksaan imaging (USG / CT scan atau MRI)")
7
Sistem skor Marshall untuk menilai gagal disfungsi organ
Sistem organ Skor 1 2 3 4 Respirasi (Pa02/Fi02) >400 301 – 400 201 – 300 101 – 200 ≤101 Ginjal (serum kreatinin; mg/dl) <1,4 1,4 – 1,8 1,9 – 3,6 3,6 – 4,9 >4,9 Kardiovaskular (mm Hg) >90 <90, respon(+) dengan cairan <90, respon(-) dengan cairan <90, pH<7,3 <90, pH<7,2
 > – – – 200. ≤101. Ginjal. (serum kreatinin; mg/dl) <1,4. 1,4 – 1,8. 1,9 – 3,6. 3,6 – 4,9. >4,9. Kardiovaskular. (mm Hg) >90. <90, respon(+) dengan cairan. <90, respon(-) dengan cairan. <90, pH<7,3. <90, pH<7,2.")
8
Definisi pankreatitis akut berat: perbandingan kriteria Atlanta 1992 dan 2012
Pankreatitis akut ringan Tidak adanya gagal organ Tidak adanya komplikasi lokal Pankreatitis akut berat Komplikasi lokal dan atau Gagal organ Perdarahan gastrointestinal >500 cc /24 jam Syok – tekanan darah sistolik ≤90 mmHg Pa02 ≤ 60% Kreatinin ≥ 2 mg/dl Pankreatitis akut sedang – berat Komplikasi lokal atau sistemik tanpa gagal organ persisten Gagal organ sementara (<48 jam) Gagal organ persisten (>48 jam) (memakai kriteria skor Marshall) Gagal organ tunggal Gagal organ multiple
 Gagal organ persisten (>48 jam) (memakai kriteria skor Marshall) Gagal organ tunggal. Gagal organ multiple.")
9
Klasifikasi Pankreatitis Akut
Berdasarkan Klasifikasi Atlanta 2012, tingkat keparahan pankreatitis akut dibagi: Pankreatitis akut ringan Pankreatitis akut sedang Pankreatitis akut berat

12
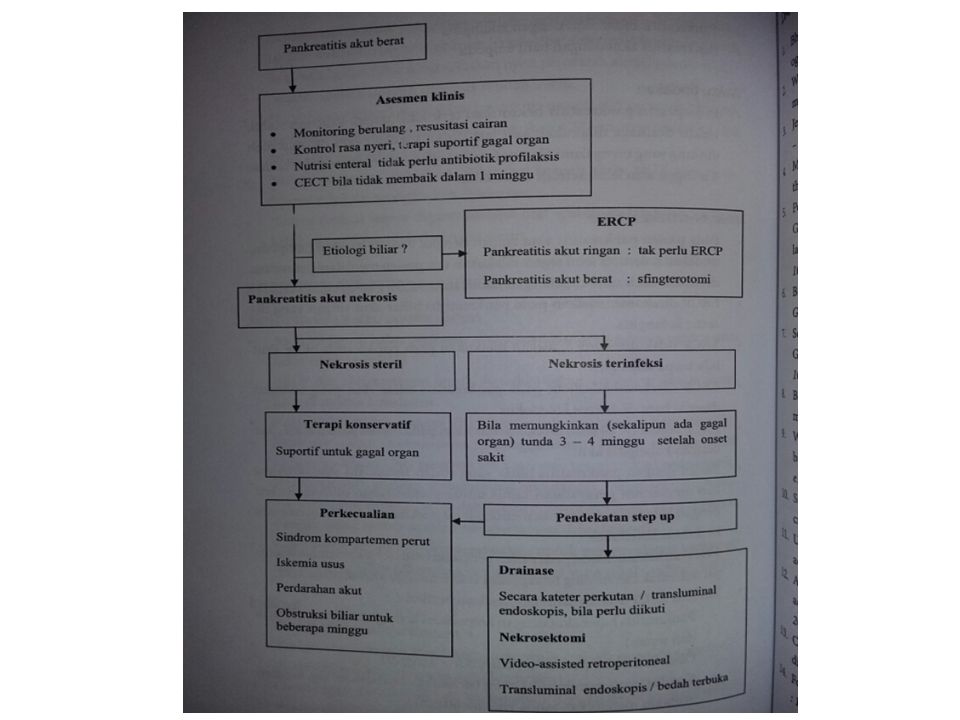
Tatalaksana Terapi supportif: resusitasi cairan, koreksi gangguan elektrolit dan koagulasi, pemberian oksigen Antibiotik: diberikan pada infeksi ekstra pankreas seperti kolangitis Analgetik: pilihan narkotik injeksi Terapi nutrisi Terapi pembedahan

13
Acute PANCREATITIS

14
EPIDEMIOLOGY AP was responsible for approximately 300,000 hospital admissions in the United States in 2012. Recent studies show the incidence of AP varies between 4.9 and 73.4 cases per 100,000 worldwide. Although the case fatality rate for AP has decreased over time, the overall population mortality rate for AP has remained unchanged.

15
PATHOPHYSIOLOGY DUCT OBSTRUCTION ACINAR CELL INJURY

16
DIAGNOSIS (REVISED ATLANTA CONSENSUS 2012)
2 of the 3 criteria: Abdominal pain consistent with the disease Serum amylase and or lipase greater than three times the upper limit of normal, and or Characteristic findings from abdominal imaging Contrast-enhanced computed tomography (CECT) and or magnetic resonance imaging (MRI) should be reserved for patients in whom: the diagnosis is unclear or who fail to improve clinically within the first 48 – 72h after hospital admission or to evaluate complications
 and or magnetic resonance imaging (MRI) should be reserved for patients in whom: the diagnosis is unclear or. who fail to improve clinically within the first 48 – 72h after hospital admission or to evaluate complications.")
17
CLINICAL PRESENTATION
Sudden-onset abdominal pain and persists for hours to days Nausea and vomiting Delirium, hemodynamic instability, extreme respiratory distress

18
PHYSICAL EXAMINATION Abdominal tenderness with guarding especially in the epigastric region Bowel sounds are diminished

19
LABORATORY STUDIES Elevated serum amylase and or lipase ≥ 3xULN
> 5xULN and lipase is more specific

20
IMAGING STUDIES Ultrasound: CT scanning:
Most sensitive noninvasive for detecting gallstone and biliary tract dilation CT scanning: Superior to ultrasound for detecting the changes associated with pancreatitis and its complications

21
IMAGING STUDIES ERCP: EUS:
Primarily a therapeutic tool in acute biliary pancreatitis (no role in diagnosing) EUS: A sensitive test for detecting persistent biliary stones for further ERCP procedure
 EUS: A sensitive test for detecting persistent biliary stones for further ERCP procedure.")
22
SYSTEMIC COMPLICATIONS
Pulmonary processes (hypoxemia, pleural effusions, ARDS) Renal failure Coagulopathy Delirium Shock
 Renal failure. Coagulopathy. Delirium. Shock.")
23
LOCAL COMPLICATION RESOLVING INTERSTITIAL PANCREATITIS WITH PSEUDOCYST
INTERSTITIAL PANCREATITIS WITH ACUTE PERIPANCREATIC FLUID COLLECTION RESOLVING INTERSTITIAL PANCREATITIS WITH PSEUDOCYST

24
LOCAL COMPLICATION PANCREATIC AND PERIPANCREATIC NECROSIS
WALLED-OFF PANCREATIC NECROSIS (ENCAPSULATED IN 4-6 WEEKS)
")
25
INITIAL ASSESSMENT AND RISK STRATIFICATION
Hemodynamic status and resuscitative measures Stratify patients into higher and lower risk categories (admission setting) Evaluate organs failure Tenner et al, American College of Gastroenterology Guideline: Management of Acute Pancreatitis, Am J Gastroenterol
 Evaluate organs failure. Tenner et al, American College of Gastroenterology Guideline: Management of Acute Pancreatitis, Am J Gastroenterol.")
26
DEFINITIONS OF SEVERITY
The onset of acute pancreatitis is defined as the time of onset of abdominal pain Early discharge No need imaging Very rare mortality SIRS Mortality 36-50% Infected necrosis

27
DEFINITIONS OF SEVERITY
A score of ≥ 2 in any system define the presence of organ failure

28
PROGNOSTIC SCORING SYSTEM (SEVERITY OF AP)
Ranson’s criteria; Glasgow prognostic criteria; APACHE II; Balthazar CT severity index; BISAP: is applicable within the first 24h presentation ≥ 3 had a mortality rate of approx. 15% CRITERIA POINTS BUN > 25mg/dL 1 Impaired mental status Presence of SIRS (≥ 2 criteria) Age > 60yo Presence of pleural effusion
 Age > 60yo. Presence of pleural effusion.")
29
TREATMENT Supportive (first 24h is golden hours):
Massive volume repletion Parenteral/enteral feeding NGT? No rule for the use prophylactic antibiotics No evidence to support routine use of somatostatin ERCP

30
INITIAL MANAGEMENT Obtain vital signs at frequent intervals (such as every 4-6 h) Supplemental oxygen be administered during the first 24–48 h, especially if narcotic agents are used to control pain. BGA should be performed when oxygen saturation is ≤95%, hypoxemia or hypotension refractory to a bolus of IV fluids.

31
INITIAL MANAGEMENT Aggressive hydration using isotonic crystalloid solution should be provided to all patients, unless cardiovascular, renal or other related comorbid factors exist (most beneficial during the first – 24 h). Lactate Ringer solution may be the preferred. Large volume normo-saline may lead to a non- anion gap, hyperchloremic metabolic acidosis.
. Lactate Ringer solution may be the preferred. Large volume normo-saline may lead to a non- anion gap, hyperchloremic metabolic acidosis.")
32
AGGRESSIVE HYDRATION Bolus 1 to 2 L of crystalloids (approx. 20 mL/kg)
Continuous infusion of 150 to 300 cc/hour (approx. 3 mL/kg/h), first 24 hours Fluid requirements assessment (intervals 6 h of admission and for h) Decrease hematocrit and BUN Maintain a normal creatinine
, first 24 hours. Fluid requirements assessment (intervals 6 h of admission and for h) Decrease hematocrit and BUN. Maintain a normal creatinine.")
33
ICU? Need aggressive fluid resuscitation
(elderly and cardiovascular disease) Deteriorating respiration (no hypoxemia) Severe
 Deteriorating respiration. (no hypoxemia) Severe.")
34
NUTRITION IN AP Mild acute pancreatitis: Severe acute pancreatitis:
Oral feedings can be started immediately if there is no nausea and vomiting and the abdominal pain has resolved. Initiation of feeding with a low-fat solid diet appears as safe as a clear liquid diet. Severe acute pancreatitis: Enteral nutrition is recommended (nasogastric and nasojejunal). Parenteral nutrition should be avoided, unless the enteral route is not available/not tolerated/not meeting caloric requirements.
. Parenteral nutrition should be avoided, unless the enteral route is not available/not tolerated/not meeting caloric requirements.")
35
NUTRITION IN AP Oral intake of limited amounts of calories is usually initiated when: Abdominal pain has subsided Parenteral narcotics are no longer required Nausea and vomiting have ceased Abdominal tenderness has markedly decreased Bowel sounds are present Overall assessment of the patient has improved

36
ANTIBIOTICS IN AP Should be given for:
Infection included extra-pancreatic Necrosis who deteriorate or fail to improve after days of hospitalization → infected Is not recommended: Prophylactic antibiotics No source of infection is identified

37
ERCP IN AP Concurrent acute cholangitis should undergo ERCP within 24 h Progressive bilirubin increasing (CBD obstruction/biliary pancreatitis) In the absence of cholangitis and or jaundice, MRCP or EUS rather than diagnostic ERCP should be used to screen for choledocholithiasis if highly suspected.

38
Autoimmune Pancreatitis (Ig G4– Associated Cholangitis)
Stricturing of the pancreatic duct, focal or generalized pancreatic enlargement, IgG4 > 140 mg/dL Lymphoplasmacytic infiltrate on biopsy Response to corticosteroid therapy

39
Primary Sclerosing Cholangitis

40
Epidemiology Prevalence: 6-16 cases/100.000 Incidence: 1 case/100.000
Geographical variation Men > Women Median age: 40 years Concomitant (60-80%) with UC North America and Europe > Asia and South Europe. 62%–70% of patients are male.
 with UC. North America and Europe > Asia and South Europe. 62%–70% of patients are male.")
41
Pathophysiology Immune-mediated process
Genes: HLA-DRB1*1501-DQB1*602, HLA- DRB1*1301-DQB1*0603, HLA-A1-B8-DRB1*0301- DQB1*0201 ‘Second Hit’ – environmental trigger, toxin or infectious exposure Innate and adaptive immune system Lymphocyte migration, cholangiocyte damage, fibrosis

42
Clinical Presentations
Asymptomatic Non-specific: fatigue, pruritus, jaundice, weight loss Less common: fever, chill, night sweat, abdominal pain Jaundice, Hepato-splenomegaly, Excoriations Cirrhosis

43
Clinical Presentations
Elevated alkaline phosphatase and bilirubin Aminotransferase normal or mildly elevated Synthetic function altered in advanced disease

44
Clinical Presentations
US: ductal wall thickening and focal bile duct dilations, gallbladder wall thickening, distention, gallstones and mass CT: thickened and inflamed bile ducts, saccular dilation intra-hepatic ducts and mass in gallbladder MRCP: “beaded” appearance – multifocal short annular strictures alternate between normal and dilated

45
Diagnosis Gold standard: MRCP with sensitivity and specificity of 86% and 94%, and ERCP Multifocal annular strictures alternating with segments of normal or dilated bile ducts of intrahepatic and/or extrahepaticbile ducts – ‘bead on a string apperance’ Rule out IgG-4 Liver biopsy rarely helpful – “onion skin” (25%), small duct PSC, PSC-AIH overlap syndrome
, small duct PSC, PSC-AIH overlap syndrome.")
46
MRCP reveals the caliber fluctuations and irregular walls of the CBD and the intrahepatic bile ducts. There is narrowing of a long segment of the distal portion of the CBD. Similar findings are seen in this image of the bile ducts obtained by ERCP.

47
Onion Skin Apperance NEJM 1995
A necrotic bile duct is at the center of an enlarged, scarred portal triad. Note the onionskin appearance of the concentric rings of connective tissue. The inflammation and scar tissue extend into the periportal parenchyma. NEJM 1995

48
Diagnosis Classic PSC: biliary strictures with normal intervening segments or diffusely involved long segments. Radio-occult: strictures not present, shallow ulcerations bile duct Small duct PSC more difficult to diagnosis Antibodies are non-specific 87%: Intra and Extra-hepatic bile ducts. 11%: Intra-hepatic bile ducts. 2%: Extra-hepatic bile ducts. Small duct PSC : 10%

49
Serum Autoantibodies in PSC

50
Differential Diagnosis
The clinical history, distribution of cholangiographic findings, and the presence or absence of IBD, have to be taken into consideration when determining if an abnormal cholangiogram is due to PSC or secondary processes. Clinical Liver Disease, Vol 3, No 3, March 2014

51
Treatments No proven medical therapy
Ursodeoxycholic acid (UDCA): 15 mg/kg/day – improve biochemical markers and inflammation Endoscopic treatment - dominant bile-duct stenosis Liver transplantation (LTx) – end stage liver disease, portal hypertension refractory therapy, intractable pruritus, reccurent cholangitis LTx: 5 and 10 year survival rates of 87.4% and 83.2 % Dominant bile duct strictures: stenoses <1.5 mm in diameter in the common bile duct and <1 mm in the right and left hepatic duct
: 15 mg/kg/day – improve biochemical markers and inflammation. Endoscopic treatment - dominant bile-duct stenosis. Liver transplantation (LTx) – end stage liver disease, portal hypertension refractory therapy, intractable pruritus, reccurent cholangitis. LTx: 5 and 10 year survival rates of 87.4% and 83.2 % Dominant bile duct strictures: stenoses <1.5 mm in diameter in the common bile duct and <1 mm in the right and left hepatic duct.")
52
Major RCT of UDCA in the Treatment of PSC
PSC Management and Surveillance Clinical Liver Disease, Vol 3, No 3, March 2014

53
Complications Obstructive
Colorectal Cancer, Cholangiocarcinoma, HCC, Gallbladder Cancer Cirrhosis Cholelithiasis, Fat-soluble vitamin deficiencies, Osteoporosis

54
The risk of developing PSC-associated cancers
CRC (colorectal carcinoma) – 9% at 10 years and 31% at 20 years in patients with both PSC and chronic inflammatory bowel disease (CIBD). CCC (cholangiocellular carcinoma) – ca. 11% cumulative incidence in population studies; up to 26% in patients with dominant stenoses with 9 years of follow-up. HCC (hepato-cellular carcinoma). GB (gall-bladder carcinoma). PC (pancreatic carcinoma) – only a single study indicates elevated risk (significance unclear). Dtsch Arztebl Int 2013
 – 9% at 10 years and 31% at 20 years in patients with both PSC and chronic inflammatory bowel disease (CIBD). CCC (cholangiocellular carcinoma) – ca. 11% cumulative incidence in population studies; up to 26% in patients with dominant stenoses with 9 years of follow-up. HCC (hepato-cellular carcinoma). GB (gall-bladder carcinoma). PC (pancreatic carcinoma) – only a single study indicates elevated risk (significance unclear). Dtsch Arztebl Int")
55
Clinical surveillance of PSC
Dtsch Arztebl Int 2013

56
Cholangiocarcinoma surveillance in PSC
Clinical Liver Disease, Vol 3, No 3, March 2014

57
Prognosis Median time to death or transplantation:
12-18 years for asymptomatic and no IBD 9 years for symptomatic Mayo Risk Score: R = 0.03 (age [years]) loge (bilirubin [mg/ dL]) loge (AST [UIL]) (variceal bleeding [0/1]) − 0.84 (albumin [g/dL])
 loge (bilirubin [mg/ dL]) loge (AST [UIL]) (variceal bleeding [0/1]) − 0.84 (albumin [g/dL])")
58
Gallbladder cancer surveillance in PSC
Clinical Liver Disease, Vol 3, No 3, March 2014

59
Subclassification of PSC

60
Relationships between subphenotypes of PSC

62
Diagnostic Algorithm for the Overlap Syndromes

63
Diagnostic Features of the Overlap Syndromes

64
Treatment Options for the Overlap Syndromes

65
Simplified Criteria for the Diagnosis of AIH
*A score 6 indicates probable AIH; a score 7 indicates definite AIH. †Additional points for all autoantibodies cannot exceed a maximum of 2.

66
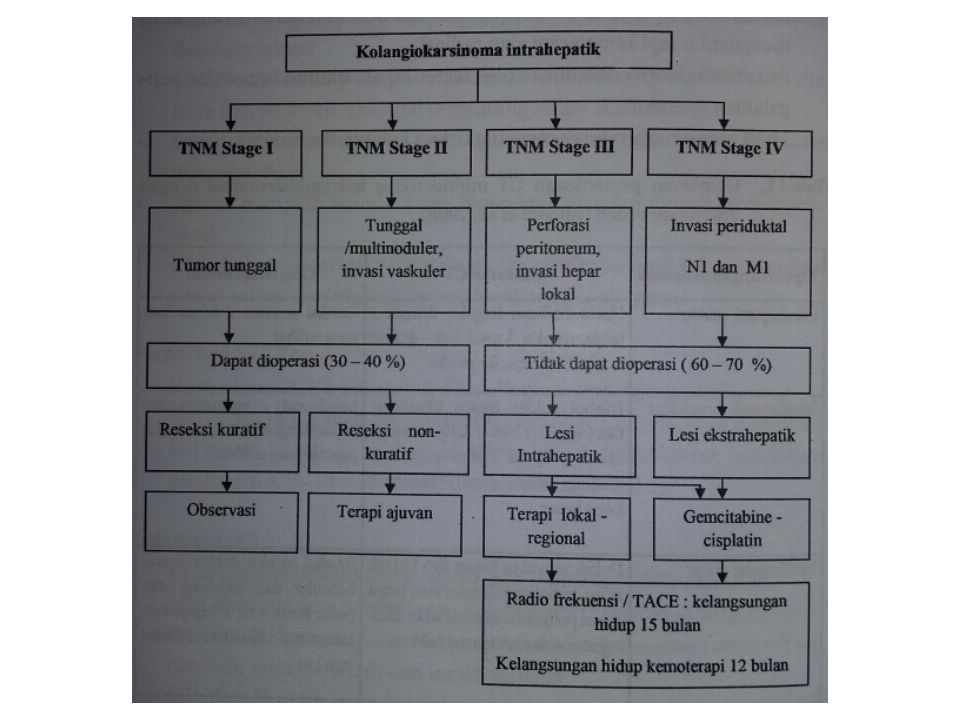
Kolangiokarsinoma Tumor primer dari epitel duktus biliaris
Kanker hepatobilier terbanyak kedua setelah karsinoma hepatoseluler 95% adalah adenokasinoma Lokasi 20% intra hepatik /perifer, 80% ekstra hepatik (70-80% perihilar dan 20-30% distal duktus biliaris) Faktor risiko: kolangitis sklerosing primer, kista duktus biliaris, sirosis hepatis, hepatitis B dan C, infeksi clonorchis sinensis
 Faktor risiko: kolangitis sklerosing primer, kista duktus biliaris, sirosis hepatis, hepatitis B dan C, infeksi clonorchis sinensis.")
Presentasi serupa


>")


















