Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
CURRICULUM VITAE PELATIHAN PENDIDIKAN UMUM PENDIDIKAN MILITER 1 1
DATA PRIBADI Nama : dr.ADIB ABDULLAH YAHYA,MARS Pangkat : Brigjen TNI (Purn) Tempat/tanggal lahir : Magelang,16 Februari 1949 Jabatan : DIREKTUR UTAMA RUMAH SAKIT MMC Agama : Islam ALAMAT : Jl. Punai H-24,Kel.Tengah,Jakarta Timur – 13540 Telp : (021) Fax : (021) HP : PENDIDIKAN UMUM SMA Negeri Magelang 1966 S1 : Fakultas Kedokteran Universitas Gajah Mada (UGM), Yogyakarta, 1973 S2 : Fakultas Kesehatan Masyarakat, Universitas Indonesia (UI), Jakarta, Program Kajian Administrasi Rumah Sakit ( KARS ) PENDIDIKAN MILITER Sekolah Staf dan Komando TNI Angkatan Darat (SESKOAD), 1987/1988 PELATIHAN Combined Humanitarian Assistance Response Training, oleh Singapore Armed Forces (SAF), Singapura, 2000 Health as a Bridge for Peace Workshop, oleh World Health Organization (WHO), Yogyakarta, 2000 1 1
 Tempat/tanggal lahir : Magelang,16 Februari Jabatan : DIREKTUR UTAMA RUMAH SAKIT MMC. Agama : Islam. ALAMAT : Jl. Punai H-24,Kel.Tengah,Jakarta Timur – Telp : (021) Fax : (021) HP : PENDIDIKAN UMUM. SMA Negeri Magelang S1 : Fakultas Kedokteran Universitas Gajah Mada (UGM), Yogyakarta, S2 : Fakultas Kesehatan Masyarakat, Universitas Indonesia (UI), Jakarta, Program Kajian Administrasi Rumah Sakit ( KARS ) PENDIDIKAN MILITER. Sekolah Staf dan Komando TNI Angkatan Darat (SESKOAD), 1987/1988. PELATIHAN. Combined Humanitarian Assistance Response Training, oleh Singapore Armed Forces (SAF), Singapura, Health as a Bridge for Peace Workshop, oleh World Health Organization (WHO), Yogyakarta,")
2
PENGALAMAN JABATAN Komandan Detasemen Kesehatan Pasukan Pengamanan Presiden (DanDenkes Paspampres), Kepala Rumah Sakit “Muhammad Ridwan Meuraksa”, Jakarta, 1992 Kepala Kesehatan Daerah Militer (Kakesdam) Jaya, Jakarta, 1993 Komandan Pusat Pendidikan Kesehatan TNI – AD,1995 – 1999 Wakil Kepala Pusat Kesehatan TNI, 1999 – 2000 Kepala RSPAD Gatot Soebroto, 2000 – 2002 Dekan Fakultas Kedokteran UPN, Jakarta, 2000 – 2002 Wakil Ketua Tim Dokter Kepresidenan RI, 2000 – 2002 Direktur Kesehatan TNI Angkatan Darat (Dirkesad), Wakil Ketua Tim Pemeriksaan kesehatan untuk calon Presiden dan calon Wakil Presiden RI Th.2004 DOSEN Pasca Sarjana FKM UI, Kajian Administrasi Rumah Sakit (KARS) DOSEN Pasca Sarjana URINDO DIREKTUR UTAMA RUMAH SAKIT MMC ORGANISASI Ketua Ikatan Rumah Sakit Jakarta Metropolitan (IRSJAM), Ketua Umum Perhimpunan Rumah Sakit Seluruh Indonesia ( PERSI), Anggota Komnas FBPI. Ketua Komtap Bidang Kebijakan Kesehatan KADIN Indonesia Angggota TNP2K. Dewan Pakar Perhimpunan Rumah Sakit Seluruh Indonesia ( PERSI) Dewan Pakar IDI Anggota Majelis Kehormatan Etik Kedokteran (MKEK) IDI Pusat Tim Konsultan Institut Manajemen Risiko Klinis ( IMRK ) Anggota KNKPRS Koordinator Bidang 1 : KAJIAN KESELAMATAN PASIEN, IKPRS- PERSI Instruktur HOPE ( Hospital Preparedness for Emergencies and Disasters} PRESIDENT OF ASIAN HOSPITAL FEDERATION ( AHF ) 2009 – 2011 2 2
 Jaya, Jakarta, Komandan Pusat Pendidikan Kesehatan TNI – AD,1995 – Wakil Kepala Pusat Kesehatan TNI, 1999 – Kepala RSPAD Gatot Soebroto, 2000 – Dekan Fakultas Kedokteran UPN, Jakarta, 2000 – Wakil Ketua Tim Dokter Kepresidenan RI, 2000 – Direktur Kesehatan TNI Angkatan Darat (Dirkesad), Wakil Ketua Tim Pemeriksaan kesehatan untuk calon Presiden dan calon Wakil Presiden RI Th DOSEN Pasca Sarjana FKM UI, Kajian Administrasi Rumah Sakit (KARS) DOSEN Pasca Sarjana URINDO. DIREKTUR UTAMA RUMAH SAKIT MMC. ORGANISASI. Ketua Ikatan Rumah Sakit Jakarta Metropolitan (IRSJAM), Ketua Umum Perhimpunan Rumah Sakit Seluruh Indonesia ( PERSI), Anggota Komnas FBPI. Ketua Komtap Bidang Kebijakan Kesehatan KADIN Indonesia. Angggota TNP2K. Dewan Pakar Perhimpunan Rumah Sakit Seluruh Indonesia ( PERSI) Dewan Pakar IDI. Anggota Majelis Kehormatan Etik Kedokteran (MKEK) IDI Pusat. Tim Konsultan Institut Manajemen Risiko Klinis ( IMRK ) Anggota KNKPRS. Koordinator Bidang 1 : KAJIAN KESELAMATAN PASIEN, IKPRS- PERSI. Instruktur HOPE ( Hospital Preparedness for Emergencies and Disasters} PRESIDENT OF ASIAN HOSPITAL FEDERATION ( AHF ) 2009 –")
3
PERAN TENAGA TEKNIK PERUMAHSAKITAN DIBIDANG MFK DALAM PROGRAM KESELAMATAN DAN KEAMANAN RS
Dr. Adib Abdullah Yahya, MARS DIREKTUR UTAMA RS MMC SEMILOKA DIT JEN DIKTI : “ PERAN TEKNIK PERUMAH SAKITAN DALAM MEMENUHI STANDAR AKREDITASI RUMAH SAKIT DIBIDANG MANAJEMEN FASILITAS DAN KESELAMATAN “ JAKARTA, 20 MARET 2014

4
The roles of hospital engineering

5
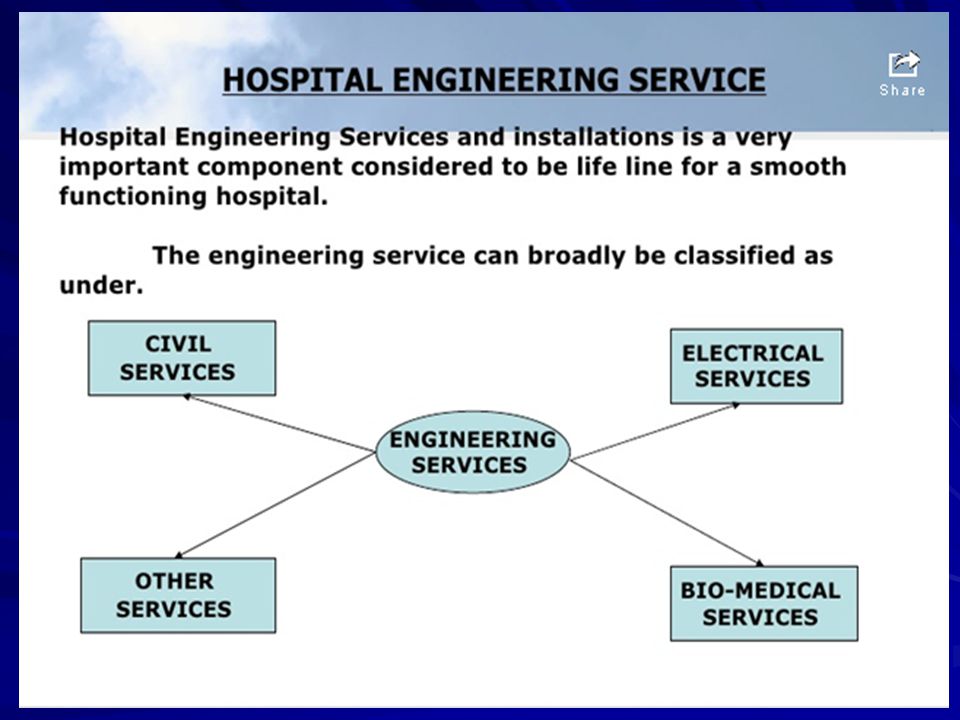
What is hospital engineering?
: "Hospital engineering is defined as both an art and a science of efficiency planning, managing and maintaining the physical environment, equipment and systems for health care and includes plant operations, clinical engineering, biomedical engineering, safety technology and telecommunications“ (Justisiano Nurak) For a hospital to run efficiently, all the mechanical, electrical, fire, safety and building maintenance systems must be operating at optimum levels. A hospital engineer is in charge of observing these operations and keeping them functional.
 For a hospital to run efficiently, all the mechanical, electrical, fire, safety and building maintenance systems must be operating at optimum levels. A hospital engineer is in charge of observing these operations and keeping them functional.")
6
Engineering Services are perhaps the most vital of the utility services in the hospital.
The efficiency of entire patient care delivery system of the hospital depends on their efficiency. Even the slightest breakdown of power supply system, information system communication system or malfunctioning of vital equipment can have catastrophic effects.

10
IMPORTANT ROLES Smooth functioning of the hospital.
To ensure optimum operational efficiency. Risk reduction and Safety to patients, staff and the public.

11
Safety and risk management In hospitals

12
The hospital develops and maintains
Standard FMS.2 The hospital develops and maintains a written program(s) describing the processes to manage risks to patients, families, visitors, and staff.
 describing the processes to manage risks to. patients, families, visitors, and staff.")
13
To manage the risks within the environment in which patients are treated and staff work requires planning. The hospital develops one master program or individual programs that include the following: a) Safety and Security Safety—The degree to which the hospital’s buildings, grounds, and equipment do not pose a hazard or risk to patients, staff, and visitors Security—Protection from loss, destruction, tampering, or unauthorized access or use b) Hazardous materials—Handling, storage, and use of radioactive and other materials are controlled, and hazardous waste is safely disposed. c) Emergencies—Response to epidemics, disasters, and emergencies is planned and effective. d) Fire safety—Property and occupants are protected from fire and smoke. e) Medical technology—Technology is selected, maintained, and used in a manner to reduce risks. f) Utility systems—Electrical, water, and other utility systems are maintained to minimize the risks of operating failures.
 Safety and Security. Safety—The degree to which the hospital’s buildings, grounds, and equipment do not pose a hazard or risk to patients, staff, and visitors. Security—Protection from loss, destruction, tampering, or unauthorized access or use. b) Hazardous materials—Handling, storage, and use of radioactive and other materials are controlled, and hazardous waste is safely disposed. c) Emergencies—Response to epidemics, disasters, and emergencies is planned and effective. d) Fire safety—Property and occupants are protected from fire and smoke. e) Medical technology—Technology is selected, maintained, and used in a manner to reduce risks. f) Utility systems—Electrical, water, and other utility systems are maintained to minimize the risks of operating failures.")
14
to reduce and control risks in the care environment.
Standard FMS.3 One or more qualified individuals oversee the planning and implementation of the facility management program to reduce and control risks in the care environment.

15
Hospitals need to develop a facility/environment risk management program that addresses managing environmental risk through the development of facility management plans and the provision of space, technology, and resources. One or more individuals provide oversight to the program. In a small hospital, one individual may be assigned part-time. In a larger hospital, several engineers or other specially trained individuals may be assigned.

16
Safety and Security Safety refers to ensuring that the building, property, medical and information technology, equipment, and systems do not pose a physical risk to patients, families, staff, and visitors. Security, refers to protecting the organization’s property and the patients, families, visitors, and staff from harm.

17
Prevention and planning are essential to creating a safe and supportive patient care facility.
Effective planning requires the hospital to be aware of all the risks present in the facility. The goal is to prevent accidents and injuries; to maintain safe and secure conditions for patients, families, staff, and visitors; and to reduce and to control hazards and risks. This is also important during periods of construction or renovation.

18
As part of the safety program, the hospital develops and implements a comprehensive, proactive risk assessment to identify areas in which the potential for injury exist. Examples of safety risks that pose a potential for injury or harm include sharp and broken furniture, linen chutes that do not close properly, broken windows, water leaks in the ceiling, and locations where there is no escape from fire. This periodic inspection is documented and helps the hospital design and carry out improvements and budget for longer-term facility upgrading or replacement. Construction and renovation pose additional risks to the safety of patients, families, visitors, and staff, and include risk related to infection control, ventilation, traffic flow, garbage/refuse, and other risks. A preconstruction risk assessment is helpful in identifying these potential risks, as well as the impact of the construction project on services provided. The risk assessment should be performed during all phases of construction.

19
In addition to the safety program, the hospital must have a security program to ensure that everyone in the hospital is protected from personal harm and from loss or damage to property. Restricted areas such as the newborn nursery and the operating theatre must be secure and monitored. Children, elderly adults, and other vulnerable patients unable to protect themselves or signal for help must be protected from harm. In addition, remote or isolated areas of the facility and grounds may require the use of security cameras.

20
PROSES MANAJEMEN RISIKO
TEGAKKAN KONTEKS IDENTIFIKASI RISIKO KOMUNIKASI DAN KONSULTASI ANALISA RISIKO MONITOR DAN REVIEW ASESMEN RISIKO EVALUASI RISIKO KELOLA RISIKO RISK REGISTER

21
Contoh Risiko yang biasanya harus diketahui terkait Safety
1. Luka Tusuk Jarum 2. Cedera Punggung 3. Terpapar radiasi atau hazmat lain 4. Pasien agresif 5. Terpeleset, Tersandung dan Jatuh 6. Kekerasan di Tempat Kerja 7. Tersengat Listrik 8. Luka Bakar 9. Properti Rusak 10. Pasien dengan TBC 11. Penyakit yang ditularkan melalui darah 12. Kebakaran 13. Banjir dan disaster alam lain 14. Kebisingan 15. Risiko yang menyebabkan gangguan muskuloskeletal

22
Insiden Security * Pasien Bunuh Diri * Penculikan bayi / anak
* Pasien kabur * Ancaman bom * VIP * Perampokan bersenjata * Informasi yang bersifat rahasia / Information security

23
Area Rawan Security Menambahkan Perangkat Keamanan khusus untuk Area yang rawan : Contoh area: * Unit Perawatan bayi * Unit psikiatri * Farmasi * Unit Gawat Darurat : * Ruang tunggu * Ruang Triage * Ruang Tindakan * Ruang Seklusi * Ruang Polisi * Safe room

24
Security / Safety Plan Purpose * Goals * Responsible Individual
* Safety Risk Assessment * Facility Inspections * Preventive safety program strategies * Active safety program * Roles of Safety / security Committee * Monitoring data (measures) for improvements in the safety and security program * Training / Education Program * Annual program Evaluation
 for improvements in the safety and security program. * Training / Education Program. * Annual program Evaluation.")
25
The Impact of Facility Design on Patient Safety

26
The Impact of Facility Design on Patient Safety
Recent attention in health care has been on the actual architectural design of a hospital facility, including its technology and equipment, and its effect on patient safety. To address the problems of errors in health care and serious safety issues, fundamental changes of health care processes, culture, and the physical environment are necessary and need to be aligned, so that the caregivers and the resources that support them are set up for enabling safe care.

27
Contributary Factors Influencing
Clinical Practice Organisational & Corporate Culture Defence Barriers Task Management Decisions/ Organisational Processes Error Producing Conditions Error Violation Producing Conditions Violation Latent Failures Active Failures ( “sharp end “ ) -Procedure Professionalism Team Individual Environment Equipment PATIENT TASK AND TECHNOLOGY INDIVIDUAL TEAM WORK ENVIRONMENT Planning, Designing , Policy-making, Communicating Emergency Diagnose Pemeriksaan Pengobatan Perawatan Adapted from Reason (revised)
 -Procedure. Professionalism. Team. Individual. Environment. Equipment. PATIENT. TASK AND TECHNOLOGY. INDIVIDUAL. TEAM. WORK ENVIRONMENT. Planning, Designing , Policy-making, Communicating. Emergency. Diagnose. Pemeriksaan. Pengobatan. Perawatan. Adapted from Reason (revised)")
28
With human factors in mind, there are several aspects of the built environment that should be considered. The following design elements were identified as critical in ensuring patient safety and quality care, based on the six quality aims of the Institute of Medicine’s report, Crossing the Quality Chasm: A New Health System for the 21st Century: 1. Patient-centeredness, including using variable-acuity rooms and single-bed rooms ensuring sufficient space to accommodate family members enabling access to health care information having clearly marked signs to navigate the hospital 2. Safety, including applying the design and improving the availability of assistive devices to avert patient falls using ventilation and filtration systems to control and prevent the spread of infections using surfaces that can be easily decontaminated facilitating hand washing with the availability of sinks and alcohol hand rubs preventing patient and provider injury addressing the sensitivities associated with the interdependencies of care, including work spaces and work processes

29
3. Effectiveness, including
use of lighting to enable visual performance use of natural lighting controlling the effects of noise 4. Efficiency, including standardizing room layout, location of supplies and medical equipment minimizing potential safety threats and improving patient satisfaction by minimizing patient transfers with variable-acuity rooms 5. Timeliness, by ensuring rapid response to patient needs eliminating inefficiencies in the processes of care delivery facilitating the clinical work of nurses 6. Equity, by ensuring the size, layout, and functions of the structure meet the diverse care needs of patients

30
THANK YOU

Presentasi serupa

>")




>")













