Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
DISKUSI KASUS TRAUMA MULTIPEL
Kiki Lukman Divisi Bedah Digestif Dept. Ilmu Bedah FK UNPAD/RS Dr Hasan Sadikin

2
1. Ny. A. R. / ♀ / 18 thn. Diterima di IGD RS tanggal 06-04-2014, Jam:
1. Ny. A.R. / ♀ / 18 thn Diterima di IGD RS tanggal , Jam: WIB KU : Nyeri perut AK : Kurang lebih 3 jam SMRS saat pasien sedang belajar mengendarai sepeda motor di daerah Jatinangor dengan kecepatan tinggi, tanpa helm, tiba-tiba pasien menabrak tembok sehingga pasien terpental ke arah depan dengan kepala dan badan membentur tembok. Pingsan -, Muntah -, Perdarahan telinga/hidung/mulut -. Setelah itu pasien mengeluh nyeri perut disertai luka di kepala. Pasien dibawa ke Klinik Jatinangor kemudian dirujuk ke RSHS.

3
Pertanyaan 1: Apa saja masalah yang paling mungkin timbul?
Cidera kepala berat dan ekstremitas Syok perdarahan + cidera kepala + cidera abdomen Obstruksi jalan nafas + cidera kepala berat + cidera panggul Cidera kepala berat dan trauma dada Trauma abdomen dan cidera kepala berat

4
Pertanyaan 2: Berapa personel yang dibutuhkan untuk mengelola pasien ini di IGD?
Tujuh orang Enam orang Lima orang Empat orang Tiga orang

5
The Trauma Team: How to implement?

6
PEMERIKSAAN FISIK Survei Primer : A : Clear + c-spine controlled B : RR : 32x/m, Bentuk/Gerak simetris, Hemi thoraks kiri: hipersonor, vbs ki < ka, rh -/-, wh -/- , Trakhea di tengah, JVP tidak meningkat. Diberikan Oksigen 10 l/m, Dipasang CTT: keluar air bubble, RR = 24 x/m

7
Pertanyaan 3: Apakah diagnosis penyebab masalah breathing?
Kontusio paru Pneumothoraks Hematothoraks masif Tension Pneumothoraks Ruptura trachea

8
Pemeriksaan Fisik C : N : 120x/m lemah, TD : 90/60 , Bunyi jantung tidak menjauh

9
Pertanyaan 4: Apakah penyebab hipotensi pada pasien ini ?
Pneumothoraks Hematothoraks masif Syok perdarahan Syok spinal Syok kardiogenik

10
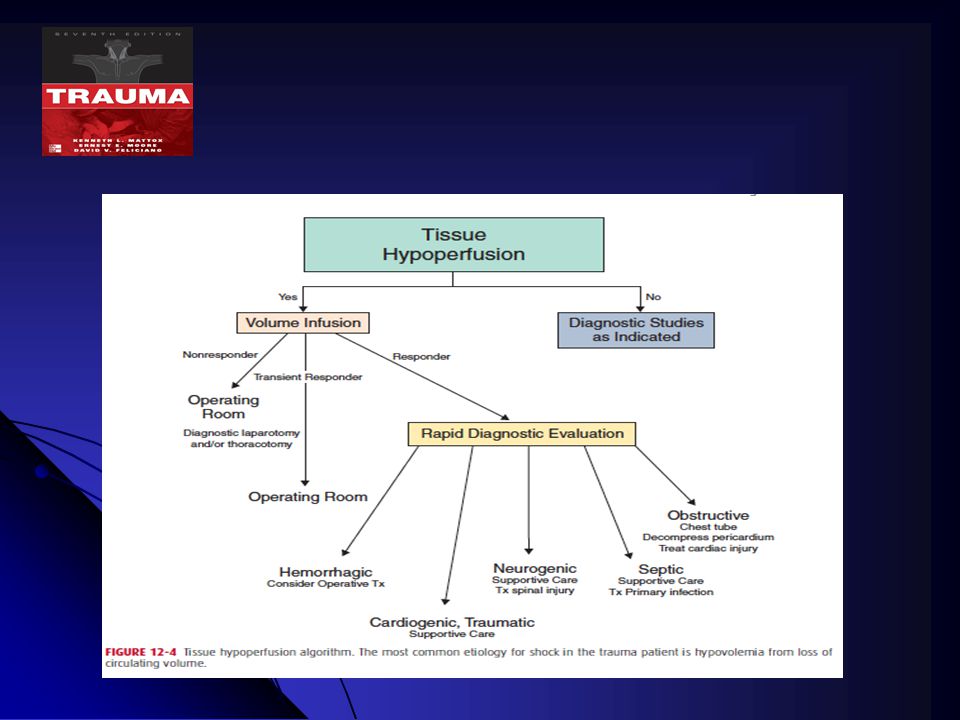
Algoritma Hipoperfusi

11
Pertanyaan 5: Setelah 3 jam dari kejadian, apakah masalah sirkulasi yang paling mungkin pada pasien ini ? Telah terjadi hipotermi, koagulopati dan asidosis Telah terjadi koagulopati, hipotermi, asidosis dan SIRS. Telah terjadi koagulopati, hipotermi, asidosis dan MODS Telah terjadi anemia dan koagulopati Telah terjadi gangguan mikrosirkulasi ireversibel

12
Concept of pathogenesis of physiologic changes in Multiple Trauma
Inflammation Haemorrhage Fibrinolysis Activation of haemostasis & endothelium Shock Tissue Hypoxia and Acidosis Coagulopathy

13
Traumatic Coagulopathy
Mc Leod, JBA, Arch Surg 143, Aug.2008

14
Pertanyaan 6: Bagaimana strategi resusitasi cairan pada pasien ini?
Pemberian cairan kristaloid hipotonik dengan target MAP 80 mmHg Pemberian cairan koloid dengan dengan target MAP 65 mmHg Pemberian Fresh Whole Blood Pemberian cairan plasma Pemberian cairan kristaloid isotonik tidak lebih dari 1500 ml.

15
Recommendation Of Fluid Therapy

16
Recommendation of Fluid Therapy in Trauma Patients
Fluid therapy be initiated in the hypotensive bleeding trauma patient – Garde 1A Crystalloids first choice – Grade 1B Avoid hypotonic solution RL sol Coloids used within the prescribed limit for each solution Hypertonic solution for unstable penetrating torso trauma – Grade 2C

17
Recommendation of Fluid Therapy in Trauma Patients
Administration of vasopressors to maintain to target MAP if no response to fluid therapy – Grade 2C Or inotropic myocardial dysfunction Maintain temperature > 35 degree C – Grade 1C Target Hb 7 – 9 gr%

18
Survai Sekunder a.r Frontalis : Luka terbuka 5x1x1 cm, tepi tidak rata, dasar fraktur depress < 1 tabula a.r Thorax : Jejas (-), B/G simetris, VBS ka>ki, rh -/-, wh -/-, Trakhea di- tengah, JVP tidak meningkat a.r Abdomen : Jejas (-), datar, lembut, BU menurun, NT(+), NL(-), DM (-) Pelvis : Kateter : Gross hematuria
, B/G simetris, VBS ka>ki, rh -/-, wh -/-, Trakhea di- tengah, JVP tidak meningkat. a.r Abdomen : Jejas (-), datar, lembut, BU menurun, NT(+), NL(-), DM (-) Pelvis : Kateter : Gross hematuria.")
19
a/r Femoralis sinistra L : Luka -, Oedem (+), deformitas (+) F : NT (+), sensisbilitas distal (+), CRT <2” M : ROM terbatas karena nyeri a/r Cruris sinistra a/r interdigiti I pedis dextra L : Luka terbuka uk 5x1x1 cm -, tepi irreguler, dasar tulang, Oedem (+), deformitas (+) F : NT (+), sensibilitas distal (+), CRT <2”
, deformitas (+) F : NT (+), sensisbilitas distal (+), CRT <2 M : ROM terbatas karena nyeri a/r Cruris sinistra a/r interdigiti I pedis dextra L : Luka terbuka uk 5x1x1 cm -, tepi irreguler, dasar tulang, Oedem (+), deformitas (+) F : NT (+), sensibilitas distal (+), CRT <2")
20
FAST Hepatorenal + Splenorenal - Retrovesica +

21
Foto Klinis

22
Resusitasi cairan dalam 15 menit:
Resusitasi kristaloid 1500 ml TD : 60/palpasi, N : 140 x/mnt D : GCS 14 (E3M6V5), pupil bulat isokor, 3/3 mm. RC (+/+). Paresis (-)
, pupil bulat isokor, 3/3 mm. RC (+/+). Paresis (-)")
23
Diagnosis klinik DK/ Perdarahan Class IV non responder + Pneumothorax sinistra ec trauma tumpul torax + Fraktur depress terbuka < 1 tabula a.r frontal dextra + fraktur terbuka distal end radius sinistra + fraktur tertutup femur sinistra + susp. Fraktur terbuka a.r pedis dextra + Vulnus laseratum interdigiti pedis I dextra

24
Pertanyaan 7: Apakah penyebab perdarahan pada pasien ini?
Syok hemorrhagik non responder e.c. trauma tumpul thoraks Syok hemorrhagik non responder e.c. trauma ekstremitas. Syok hemorrhagik non responder e.c. trauma tumpul abdomen Syok hemorrhagik non responder e.c. Fraktur pelvik Syok hemorrhagik non responder e.c. trauma kepala

25
Algoritma FAST pada trauma tumpul abdomen

26
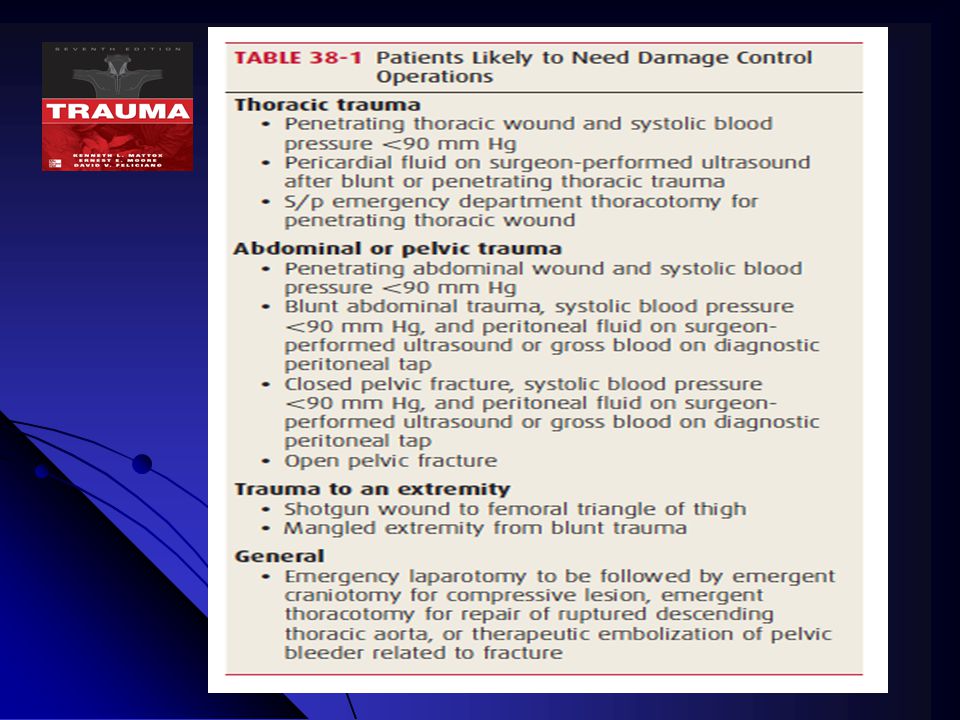
Pertanyaan 8: Apakah langkah manajemen selanjutnya?
Dilakukan laparotomi eksplorativa + damage control surgery Dilakukan laparotomi eksplorativa + damage control resuscitation + damage control surgery Dilakukan laparotomi eksplorativa + definitive surgery Dilakukan Damage Control Resuscitation dulu baru Laparatomi Dilakukan Laparotomi eksplorativa

28
Damage control resuscitation is now the predominant focus upon arrival in hospital
Crystalloid delivery should be minimized, as it can be associated with harm

29
Pre hospital Care Pre Hospital Care Less than 20 minutes Scoop and Run
Minimize Fluid Resuscitation Prevent Hypothermia GOAL: Get the patient to the trauma center Injury Pre Hospital Care Less than 20 minutes

30
Resuscitation GOAL: Mobilize promptly to OR/IR Suite Emergency Room
Allow permissive hypotension Administer blood and blood products early Minimize fluid resuscitation Start Tranexamic Acid Start massive transfusion protocol GOAL: Mobilize promptly to OR/IR Suite Emergency Room Less than 30 minutes

31
Dalam persiapan ke Kamar operasi hasil laboratorium :
Hb : 5.6 GDS : 155 Ht : 17 Na : 137 L : K : 3.3 Tr : INR : 2.13 Fibrinogen : 62.2 APTT : 142.8 D-dimer : 8.0 PT : 26.6 SGOT : 461 SGPT : 428 Urinalisis : eritrosit banyak Ur : 306 Kr : 2.3

32
Pertanyaan 8: Apakah data laboratorium lain yang diperlukan?
Hemoglobin serial Hematokrit serial Base deficit dan laktat serial Gula darah serial INR serial

33
What is the Recommendation ? ( Sphan et al critical Care 2013,17:R76)
It is not recommended the use of single Hct measurement as an isolated laboratory marker of bleeding – Grade 1B Serum lactate or base deficit measurement as sensitive test to estimate and monitor the extent of bleeding and shock – Grade 1B Routine practice to detect post traumatic coagulopathy include the early, repeated and combined measurement of PT, APTT, fibrinogen and platelets – Grade 1C

34
Temua intra-operatif Ditemukan : Perdarahan intraabdomen ± 2000 cc
Laserasi hepar di segmen 5,6,7 anterior dan segmen 5,6 posterior sesuai AAST grade IV Zona II kanan hematoma, ekspanding, pulsating eksplorasi Trauma ginjal sesuai AAST grade V Zona I, Zona II kiri, Zona III intak Organ solid dan organ berongga lainnya intak INA-CBG B-1-10-III PROSEDUR HATI DAN PANKREAS BERAT ISS : RTS : TRISS : 35.2% Rp

35
Pertanyaan 9: Bagaimanakah strategi operatif yang terpilih ?
Dilakukan reseksi non anatomikal hepar + nephrectomy + debridement fraktur depressed + Fiksasi eksterna fraktur ekstremitas. Dilakukan hepatorrhapy hepar + nephrectomy + debridement fraktur depressed + debridement + posterior slab fraktur ekstremitas. Dilakukan reseksi non anatomikal hepar + nephrectomy Mc Anich + debridement fraktur depressed + Fiksasi eksterna fraktur ekstremitas. Dilakukan peri hepatic packing + nephrectomy + debridement fraktur depressed + debridement + posterior slab fraktur ekstremitas. Dilakukan peri hepatic packing + nephrectomy + debridement fraktur depressed + debridement + posterior slab fraktur + TACD + VAC

37
Pertanyaan 10: Bagaimana jika terdapat fraktur pelvis yang tidak stabil ?
Dilakukan pemasangan extra peritoneal packing Dilakukan pelvic wrapping Dilakukan fiksasi eksterna definitif Dilakukan fiksasi interna definitif Dilakukan angiografi dan embolisasi pembuluh darah

38
TRAUMA PELVIK “ Perdarahan masif akibat fraktur pelvik tak stabil harus segera dengan difiksasi eksterna atau extra peritoneal pelvic packing atau therapeutic angiography”

39
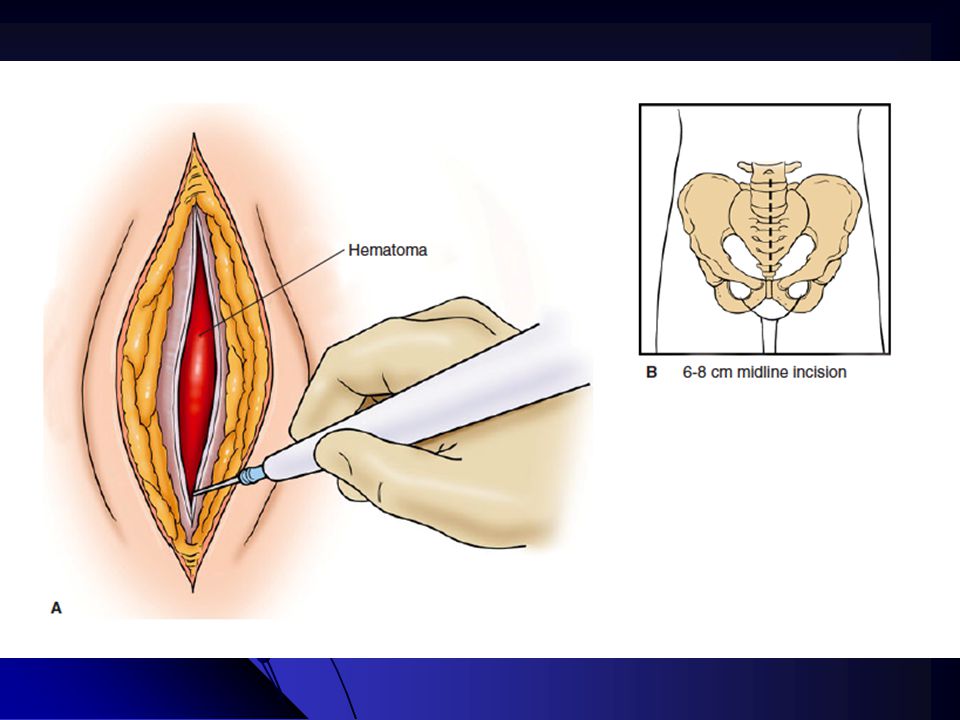
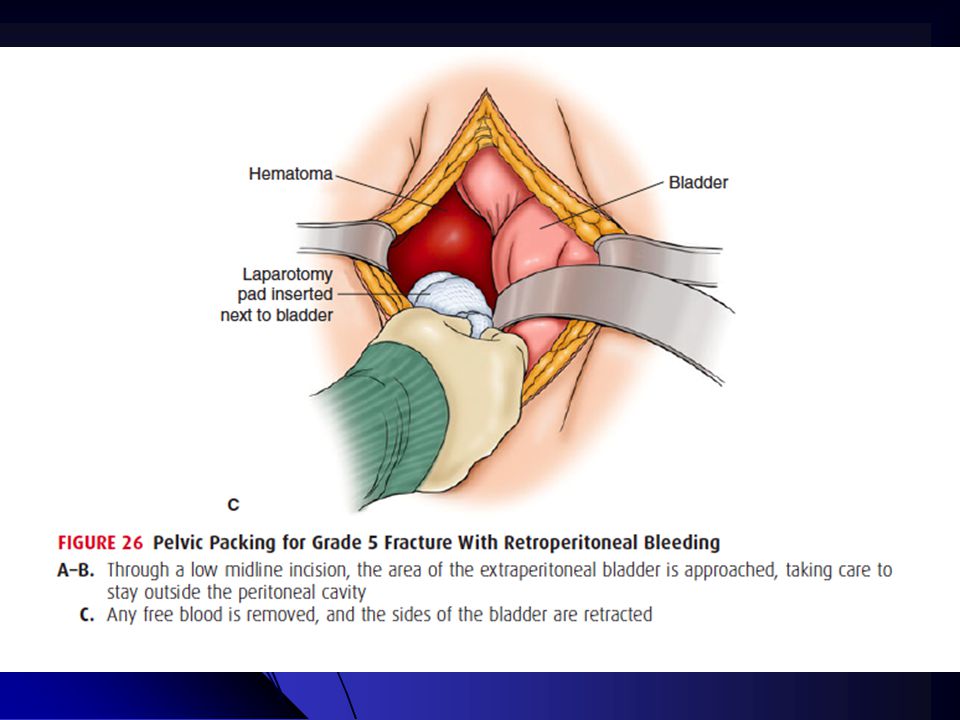
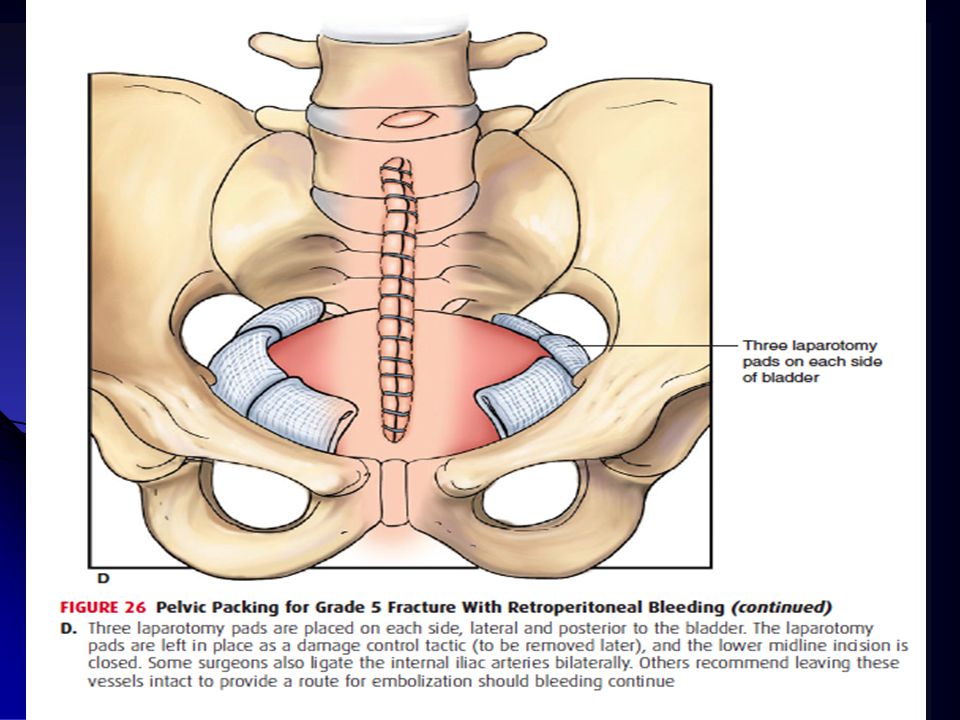
F. HEMODYNAMIC INSTABILITY AND REFRACTORY SHOCK
Preperitoneal packing Opening the retroperitoneal hematoma anteriorly, evacuating the blood and clot The bladder is retracted laterally with a malleable retractor and the pelvic brim is palpated and manually dissected Care should be taken to avoid avulsing any vascular connections between the iliac and obturator vessels After the pelvic brim is palpated as posteriorly as the surgeon can reach (it is not visualized), three laparotomy packs are placed squentially deep to the pelvic brim
, three laparotomy packs are placed squentially deep to the pelvic brim.")
43
16.45 (IGD) A : Clear + C-Spine Controlled B : RR : 28x/m, B/G simetris, VBS ka>ki, rh -/-, wh -/- , Trakhea di tengah, JVP tidak meningkat Oksigenasi NRM 10 l/m, R/ insersi CTT sinistra C : N : 120x/m lemah, TD : 90/60 Resusitasi kristaloid 1500 cc TD : 60/palpasi, N : 140 x/mnt Diputuskan naik OK D : GCS 14 (E3M6V5), pupil bulat isokor, 3/3 mm. RC (+/+). Parese (-) 17:00 (OK) - Dilakukan insersi CTT Sin DO : Air buble (+), produksi (-), undulasi (+) Dilakukan LE: - Packing eksplorasi zona I,II,III Zona II kanan hematom, ekspanding, pulsating Trauma ginjal AAST gr V nefrektomi - Aff packing Laserasi hepar di segmen 5,6,7 anterior 8 cm, dan segmen 5,6 post 5 cm Hepatorraphy + packing sementara 18:00 (Intraoperatif) DO : - Re-evaluasi post hepatorraphy rembesan darah (+) encer, merah muda kesan suspek DIC Diputuskan Packing intraabdomen Konfirmasi Lab INR 2.13/PT 26.6/APTT 142,6; Sysmex 5.6/17/13900/127000; Fib/D-dimer : 62.2/8.0 21.00 Pindah ICU (T 120/70, N 110, RR 20 dg support NA 1 mcg, dobut 10 mcg
, pupil bulat isokor, 3/3 mm. RC (+/+). Parese (-) 17:00 (OK) - Dilakukan insersi CTT Sin DO : Air buble (+), produksi (-), undulasi (+) Dilakukan LE: - Packing eksplorasi zona I,II,III Zona II kanan hematom, ekspanding, pulsating Trauma ginjal AAST gr V nefrektomi. - Aff packing Laserasi hepar di segmen 5,6,7 anterior 8 cm, dan segmen 5,6 post 5 cm Hepatorraphy + packing sementara. 18:00 (Intraoperatif) DO : - Re-evaluasi post hepatorraphy rembesan darah (+) encer, merah muda kesan suspek DIC Diputuskan Packing intraabdomen. Konfirmasi Lab INR 2.13/PT 26.6/APTT 142,6; Sysmex 5.6/17/13900/127000; Fib/D-dimer : 62.2/ Pindah ICU (T 120/70, N 110, RR 20 dg support NA 1 mcg, dobut 10 mcg.")
44
Damage Control Resuscitation and Surgery Algorithm
H.M. A. Kaafarani, G. C. Velmahos Scandinavian Journal of Surgery 0: 1–8, 2014

45
Pre hospital Care Pre Hospital Care Less than 20 minutes Scoop and Run
Minimize Fluid Resuscitation Prevent Hypothermia GOAL: Get the patient to the trauma center Injury Pre Hospital Care Less than 20 minutes

46
Resuscitation GOAL: Mobilize promptly to OR/IR Suite Emergency Room
Allow permissive hypotension Administer blood and blood products early Minimize fluid resuscitation Start Tranexamic Acid Start massive transfusion protocol GOAL: Mobilize promptly to OR/IR Suite Emergency Room Less than 30 minutes

47
Abbreviated surgical Procedure
Operating Theater Allow permissive hypotension Aim for 1:1:1 PRBC/FFP/Platelets ratio Administer cryoprecipitate Abdominal packing Temporary abdominal closure GOAL: Control surgical bleeding Control contamination Abbreviated surgical Procedure Less than 90 minutes

48
Intensive Care (1) GOAL: Resuscitate Reverse Triads of death
Reverse hypothermia Reverse coagulopathy Reverse acidosis Support hemodynamics GOAL: Resuscitate Reverse Triads of death Intensive Care Unit 12 – 36 hours

49
Definitive surgical procedure
Operating Theater Remove packing Definitive Surgical Repair Serial primary abdominal closure GOAL: Definitive surgical procedure (2 – 8 days)
")
50
Intensive Care Unit Stay
Diuresis GOAL: Decrease fluid overload to allow: Definitive abdominal closure Postoperative liberation from ventilator Intensive Care Unit Stay (2 – 8 days)
")
51
Reversing Hypothermia
Body Rewarming: (1) passive external rewarming (e.g. removal of wet clothing, warm blankets, raising the ambient temperature of room), (2) active external rewarming (e.g. forced air-warming devices), (3) active internal core rewarming
 passive external rewarming (e.g. removal of wet clothing, warm blankets, raising the ambient temperature of room), (2) active external rewarming (e.g. forced air-warming devices), (3) active internal core rewarming.")
52
Reversing Acidosis It is better achieved through:
aggressive blood and blood product resuscitation vasopressor support until surgical control of hemorrhage is achieved, shock is reversed, and end-organ perfusion is restored. End-points of resuscitation: Vital signs alone are poor indicators of end-organ perfusion. Base deficit and lactate levels are reliable perfusion indices (markers of the adequacy of resuscitation);
;")
53
Permissive Hypotension
Definition: A strategic decision to delay the initiation of fluid resuscitation and limit the volume of resuscitation fluids/blood products administered to the bleeding trauma patient by targeting a lower than normal blood pressure, usually a SBP of 80–90 mmHg or MAP of 50 mmHg.

54
The Advantages Rationales:
decreasing the incidence and severity of dilutional coagulopathy avoiding the hypothetical “pop the clot” effect, to the amelioration of the inflammatory cascade, which is exacerbated in response to exogenous fluids administration.

55
Hemostatic Resuscitation
One of the main pillars of DCR is early and aggressive transfusion of blood products aiming for a ratio of PRBCs, FFP, and platelets that approximates 1:1:1 Massive transfusion is typically defined as a transfusion of 10 or more units of PRBCs within the first 24 h of injury

56
Role of Hemostatic Adjuncts
These agents may: decrease mortality, transfusion requirements, rates of transfusion-related organ failure among certain trauma patients. BUT, increase thromboembolic events

57
Hemostatic Adjuncts Tranexamic acid: Prevent fibrinolysis
Useful within 3 hours of injury Recombinant human factor VIIa: Does not decrease mortality thrombo-embolic complications Prothrombin complex, which contains factors II, VII, IX, X, C,and S: mortality, transfusion requirements, complications, & lengths of stay

58
Hemostatic Adjuncts Anti-fibrinolytic agents
Early administration of tranexamic acid (TXA), an anti-fibrinolytic agent, (slightly decrease the risk of death from bleeding) Factor-concentrates recombinant factor VIIa or prothrombin complex concentrates (PCCs) (lack of evidence)
, an anti-fibrinolytic agent, (slightly decrease the risk of death from bleeding) Factor-concentrates. recombinant factor VIIa or prothrombin complex concentrates (PCCs) (lack of evidence)")
59
Resuscitation Goals and Monitoring
Coagulation test is inappropiate opiate PRBCs should be given to target a hemoglobin >7 g/dL, FFPs to target an international normalized ratio (INR) <2, Platelets to target a count >50,000, Cryoprecipitate to target a fibrinogen level >100 mg/dL. The use of thrombo-elastography-based protocols (promising results)
 <2, Platelets to target a count >50,000, Cryoprecipitate to target a fibrinogen level >100 mg/dL. The use of thrombo-elastography-based protocols (promising results)")
60
DAMAGE CONTROL SURGERY FOR ABDOMINAL TRAUMA
Laura Godat, Leslie Kobayashi, Todd Costantini and Raul Coimbra World Journal of Emergency Surgery 2013, 8:53

61
The Indications: Pre operative
The decision should be made early (pre operative): Systolic blood pressure (SBP) <90 mmHg with penetrating torso, Blunt abdominal, or severe pelvic trauma, The need for resuscitative thoracotomy Other Emergency Department (ED) variables : include SBP <60 mmHg, hypothermia, inappropriate bradycardia, pH of <7.2
: Systolic blood pressure (SBP) <90 mmHg with penetrating torso, Blunt abdominal, or severe pelvic trauma, The need for resuscitative thoracotomy. Other Emergency Department (ED) variables : include SBP <60 mmHg, hypothermia, inappropriate bradycardia, pH of <7.2.")
62
The Indications: Intra-operative
“ non-surgical” bleeding, pH≤ 7.18, temperature ≤ 33°C, transfusion of ≥ 10 units of blood, total fluid replacement >12 L, estimated blood losses of ≥ 5 L Platelet count, PT, aPTT, fibrinogen levels and thrombo-elastography findings

63
The Indications: Intra-operative
Patients at high riskfor ACS should be left open prophylactically at the time of laparotomy: Patients requiring large volume resuscitation (>15 L or 10 Units of PRBCs), Those with evidence of visceral edema, peak inspiratory pressures >40, intra-abdominal pressure (IAP) >21 during attempted closure [12-16].
, Those with evidence of visceral edema, peak inspiratory pressures >40, intra-abdominal pressure (IAP) >21 during attempted closure [12-16].")
64
The perioperative Critical Care
sedation, paralysis, nutrition, started early fluid management strategies may improve closure rates and recovery. Prophylactic antibiotics no more than 24 hours. Reconstructive strategies that may be used in the acute and chronic phases of abdominal closure (6 -12 months).
.")
65
Temporary Abdominal Closure Devices
Negative pressure dressing such as the “ vacuum pack” method or its commercially available alternative. After 5-7 days if the abdomen cannot be closed convert to the use of a bridging device which progressively brings the fascia together such as the Wittman patch or modified V.A.C.©.

66
VACUUM OPEN ABDOMEN MANAGEMENT
Vacuum Associated Fascial Closure buatan pabrik

Presentasi serupa













 Spine>")





 Keluhan : demam RPS : Anamnesa.>")
