Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
PENGANTAR TOKSIKOLOGI
Dr. H.Achmad Basori, MS Profesor Farmakologi Departemen Farmakologi Dan Terapi Fakultas Kedokteran UA

6
Pharmacology : Dogma and Reason
Ancient Beginnings - Religious /magical Hippocrates ( ~ 460 BC) - Observation / experience Paracelcus ( 1439 – 1541) - Applyng chemistry to medicine 1600 – 1900 Materia Medica - Experimental Physiology, Cause of Disease - Isolation of Active Principles, Synthetic Chemistry 1900 ~ Modern Era - Efficacy and Safety - Clinical Trial
 - Observation / experience. Paracelcus ( 1439 – 1541) - Applyng chemistry to medicine – 1900 Materia Medica. - Experimental Physiology, Cause of Disease. - Isolation of Active Principles, Synthetic Chemistry ~ Modern Era. - Efficacy and Safety. - Clinical Trial.")
7
Ancient Beginnings - Religious /magical
The Ebers papyrus, written in Egypt in the 16th century B.C., lists the extensive pharmacopia of that civilization. Included in this are: beer, turpentine, myrrh, , juniperberries., poppy, lead, salt and crushed precious stones. Also included were products derived from animals, including lizard's blood, swine teeth, goose grease, ass hooves and the excreta from various animals. The effects of many of these drugs on patients of antiquity can only be imagined.

8
Hippocrates ( ~ 460 BC) - Observation / experience (empiric- primitive)
 - Observation / experience (empiric- primitive)")
9
Paracelcus ( 1439 – 1541) Pharmacon or Toxicon ?
- Applyng chemistry to medicine(empiric analytic)
")
10
"The dose makes the poison.“
Swiss physician Paracelsus ( ) credited with being “the father of modern pharmacology/ toxicology.” “All substances are poisons: there is none which is not a poison. The right dose differentiates a poison from a remedy.” He determined that specific chemicals were actually responsible for the toxicity of a plant or animal poison. Paracelsus is often quoted for his statement: "All substances are poisons; there is none which is not a poison. The right dose differentiates a poison and a remedy." "The dose makes the poison.“
 credited with being. the father of modern pharmacology/ toxicology. All substances are poisons: there is none which is not a poison. The right dose differentiates a poison from a remedy. He determined that specific chemicals were actually responsible for the toxicity of a plant or animal poison. Paracelsus is often quoted for his statement: All substances are poisons; there is none which is not a poison. The right dose differentiates a poison and a remedy. The dose makes the poison.")
11
OBAT = PISAU BERMUKA DUA
MANFAAT : satu bahan bisa mendatangkan satu atau lebih efek yg menguntungkan yg digunakan utk medikasi MUDARAT : satu bahan mempunyai beberapa macam efek yg merugikan dg berbagai tingkatan dari yg ringan berat s/d fatal (side effect & adverse effect) Besar kecilnya manfaat/mudarat yg muncul dalam pengobatan tergantung dari dosis. Drug (Pharmacon) Batas kadar terapi Dalam darah Cyclosporine ng/ml Phenytoin 10 – 20 mg/ml Gentamicin 2 – 4 mg/ml Theophylline Digoxin 1 – 2 ng/ml Obat = racun Obat ”aman” bila digunakan dengan kaidah/hukum Farmakologi (Klinik)
 Besar kecilnya manfaat/mudarat yg muncul dalam pengobatan tergantung dari dosis. Drug. (Pharmacon) Batas kadar terapi. Dalam darah. Cyclosporine ng/ml. Phenytoin. 10 – 20 mg/ml. Gentamicin. 2 – 4 mg/ml. Theophylline. Digoxin. 1 – 2 ng/ml. Obat = racun. Obat aman bila digunakan dengan kaidah/hukum Farmakologi (Klinik)")
12
1600 – 1900 Materia Medica - Experimental Physiology, Cause of Disease - Isolation of Active Principles, Synthetic Chemistry

13
1900 ~ Modern Era - Efficacy and Safety - Modern Toxicology studies
- Clinical Trial

15
Isoproterenol (Isoprel) Inhaler
Bronchodilator Cardiac Arrest Isoproterenol Pure beta receptor agonist ( non- selective) Tidak mempunyai efek thd alpha-receptor
 Tidak mempunyai efek thd alpha-receptor.")
16
DRUG DISCOVERY & DEVELOPMENT PROCESSES
Overall cost per marketed compound = $ 1 – 1.2 billion time-scale = years Total patent lifetime = ~30 years DRUG DISCOVERY EARLY DEVELOPMENT CLINICAL DEVELOPMENT Phase I Phase II Phase III Phase IV Target selection Lead-finding Lead optimisation Pharmacological profiling Pharmacokinetics Short-term Toxicology Formulation Synthesis scale-up Pharmacokinetics,tolerability, side effects in healthy volunteers Small-scale trials in patients to assess efficacy & dosage Large-scale controlled trials To develop a drug is a costly process. Only 10-20% of all potential drugs reach the level of early development, 3-5% clinical development and 1-2% finally reach the market. Post-marketing surveillance 2-5 years (10-20%) 1 year (3-5%) 5-7 years (1-2%) Drug candidate Development compound Compound approved for marketing Chao Han dkk,2010 Rick et al,2010
 1 year. (3-5%) 5-7 years. (1-2%) Drug. candidate. Development. compound. Compound approved for marketing. Chao Han dkk,2010. Rick et al,2010.")
17
Pharmakon + Logos? Toxikon + Logos? What is Toxicology Pharmacology :
Old Greek = poison Modern Greek = Drug Pharmacology : Pharmakon + Logos? Toxikon Logos? Toxicology :

18
Perkembangan Ilmu Toksikologi
Pharmacology (Pharmacon+Logos): Ilmu tentang senyawa (obat) yang digunakan untuk mencegah, mendiagnosa, dan mengobati penyakit Toxicology (Toxicon + Logos) : Suatu cabang dari ilmu farmakologi yang mempelajari efek yang tidak dikehendaki dari senyawa kimia pada sistem biologi (Undesirable) (ASPET,2000) The Science of Poisons (ToxiCology) The study of toxic effects of chemicals on living systems. Study oh how natural or man made poisons cause undesirable effects in living organism PATHOLOGY: Study of structural and functional changes in cells, tissues and organs after toxic exposure
: Ilmu tentang senyawa (obat) yang digunakan untuk mencegah, mendiagnosa, dan mengobati penyakit. Toxicology (Toxicon + Logos) : Suatu cabang dari ilmu farmakologi yang mempelajari efek yang tidak dikehendaki dari senyawa kimia pada sistem biologi (Undesirable) (ASPET,2000) The Science of Poisons (ToxiCology) The study of toxic effects of chemicals on living. systems. Study oh how natural or man made poisons cause undesirable effects in living organism. PATHOLOGY: Study of structural and functional changes in cells, tissues and organs after toxic exposure.")
19
Efek Bahan / Obat Desirable Diharapkan (Therapeutic) Undesirable
Tidak Diharapkan Non-deleterious (Side effects) Deleterious (Toxic effects)
 Deleterious. (Toxic effects)")
21
DEFINISI - Toxicosis : disease state that results from exposure to a poison.

22
Toxicon Poisonous substances are produced by plants, animals, or bacteria. Phytotoxins Zootoxins Bacteriotoxins Toxicant - the specific poisonous chemical. Xenobiotic - man-made substance and/or produced by but not normally found in the body.

23
Xenobiotics ( Xenos, Foreign Chemical)
Xenobiotics may be naturally occurring chemicals produced by plants, microorganisms, or animals (including humans). Xenobiotics may also be synthetic chemicals produced by humans. Poisons are xenobiotics, but not all xenobiotics are poisonous. Xenobiotic are substances which normally is not needed by our body
. Xenobiotics may also be synthetic chemicals produced by humans. Poisons are xenobiotics, but not all xenobiotics are poisonous. Xenobiotic are substances which normally is not needed by our body.")
24
History Swiss physician Paracelsus (1493-1541) credited with being
“the father of modern toxicology.” “All substances are poisons: there is none which is not a poison. The right dose differentiates a poison from a remedy.” He determined that specific chemicals were actually responsible for the toxicity of a plant or animal poison. Paracelsus is often quoted for his statement: "All substances are poisons; there is none which is not a poison. The right dose differentiates a poison and a remedy." "The dose makes the poison.“

25
Paracetamol dosis terapi : analgesik antipiretik dosis tinggi kanker hati Viagra dosis terapi : erectogenic dosis tinggi : permanent blindness Morphine dosis terapi : analgesik kuat dosis tinggi : depresi pernafasan Air (H2O) : 1 gelas : tdk apa apa 1 galon : lambung pecah Gula : jumlah kecil : pemanis jumlah besar : hyperglycemia diabet Coma
 : 1 gelas : tdk apa apa. 1 galon : lambung pecah. Gula : jumlah kecil : pemanis. jumlah besar : hyperglycemia diabet Coma.")
27
Toxic Therapeutic Theophrastus von Hohenheim (Paracelcus,1493 – 1541)
All things are poison, nothing is without poison Toxic Minimum Toxic Concentration Therapeutic Minimum Effective Concentration Ineffective

28
Pharmacon atau Toxicon = Drug Toxicity
Batas kadar terapi Dalam darah Cyclosporine ng/ml Salicylic acid > 200 mg/ml Phenytoin 10 – 20 mg/ml Gentamicin 2 – 4 mg/ml Theophylline Digoxin 1 – 2 ng/ml

29
EFEK FARMAKOLOGI HIGH Coma Hypnosis LOW Dosis (mg/kg BB) DEATH GENERAL
ANESTHESIA Confusion, Delirium, Ataxia EFEK FARMAKOLOGI Hypnosis SEDATIVE EFFECTS Drowsiness/ decrease reaction time ANTI- CONVULSANT EFFECTS ANXIOLYTIC EFFECTS Dosis (mg/kg BB) LOW Phenobarbital (Luminal) 5x dosis hipnotik depresi nafas
 LOW. Phenobarbital (Luminal) 5x dosis hipnotik depresi nafas.")
30
Toxicity: Derajad kemampuan suatu senyawa bersifat racun dan menyebabkan kerusakan Toxicity tergantung : dosis, lama pemaparan, rute pemaparan,bentuk & struktur senyawa, faktor individu Toxic : Efek racun atau mematikan terhadap tubuh melalui inhalasi, oral, kontak langsung dgn bhn kimia Toxicant : tiap bahan kimia yang dpt melukai atau membunuh manusia, hewan, tanaman = Poison. Toxicant banyak dikaitkan dgn bahan yg dihasilkan dari produk hasil aktifitas manusia.Mis, Dioxin suatu bahan by produk pada proses khlrinasi bhn kimia.Arsenic merupakan kontaminan air atau hasil limbah industri Toxin : Senyawa toksik hasil alam. Merupakan senyawa racun dari hewan, tanaman (bacterio toxin, Zootoxin, Phytotoxin Toxicosis : Suatu penyakit yang terjadi akibat terpapar pada suatu toxicant

31
Itai Itai Disease Penyebab terpapar cadmium secara khronik (Di daerah pertambangan , Jepang). Akumulasi logam berat di air minum gagal ginjal, perlunaan tulang, lumbago, arthralgia, dan full-body muscle spasm. Diiringi rasa sakit hebat, patah tulang lengan/kaki, tubuh menjadi pendek 56 orang dila[porkan meninggal.

32
Klasifikasi Toxicant / Poison
Berdasarkan target organ : hepatotoxican,nephrotoxicant,cardiotoxicant, dll Berdasarkan penggunaannya: pesticide,solvent,food additive,dll) Berdasarkan asal bahan: animal toxins, plant toxins Berdasarkan efek: mutation,cancer,liver injury,dll Berdasarkan siFat fisik: gas, dust, liquid Berdasarkan reaktifitas kimia labeling:explosives,flammable,oxidizer,dll) Bedasarkan struktur kimia : aromatic amine,halogenated hydrocarbon,dll Berdasarkan potensi toxicant : extremely toxic,very toxic, super toxic, dll Berdasarkan mekanisme kerja : sulhydriyl inhibitor,methoglobin producer,dll)
 Berdasarkan asal bahan: animal toxins, plant toxins. Berdasarkan efek: mutation,cancer,liver injury,dll. Berdasarkan siFat fisik: gas, dust, liquid. Berdasarkan reaktifitas kimia labeling:explosives,flammable,oxidizer,dll) Bedasarkan struktur kimia : aromatic amine,halogenated hydrocarbon,dll. Berdasarkan potensi toxicant : extremely toxic,very toxic, super toxic, dll. Berdasarkan mekanisme kerja : sulhydriyl inhibitor,methoglobin producer,dll)")
33
Toxicant ( Poison = Xenobiotics)
Obat-Obatan (Psikotropik=Sedatives-hypnotics,Tranquillizer,Antidepressant,cardiovascular,Hormon,Alcohol,street drugs,Obat obat OTC,dll) Cleaning/polishing agent,hydrocarbon, paint,pestisides,corrosive,ll) Foods,Botulinum, TTX,Insect bites,dll) Animal toxin (TTX, insect bites,dll) Gas (CO,NO,Freon,dll) Industrial product (heavy metals): As, Pb, Hg,Cd,Chrom,Ba,Li,Fe,dll Cosmetics Venome Dan lain lainnya
 Cleaning/polishing agent,hydrocarbon, paint,pestisides,corrosive,ll) Foods,Botulinum, TTX,Insect bites,dll) Animal toxin (TTX, insect bites,dll) Gas (CO,NO,Freon,dll) Industrial product (heavy metals): As, Pb, Hg,Cd,Chrom,Ba,Li,Fe,dll. Cosmetics. Venome. Dan lain lainnya.")
34
TOXICOLOGY Basic Science Medical Toxicology : - Biochemical Toxicology
Biology, Biochemistry,Pathology, Physiology, Genetic, Pharmacology TOXICOLOGY Medical Toxicology : - Biochemical Toxicology - Analytical Toxicology - Cellular Toxicology Molecular Toxicology - Clinical Toxicology - Forensic Toxicology -Food Toxicology - Ecotoxicology - Industrial Toxicology -Enviromental Toxicology -Occupational Toxicology -Developmental and reproductive Toxicology -Regulatory Toxicology -Mechanistic Toxicology - Descriptive Toxicology

35
Area toksikologi khusus yang penting utk kedokteran :
Forensic toxicology kombinasi kimia analitik dan toksikologi dasar yang memperhatikan aspek medikolegal Clinical toxicology fokus pada penyakit yang disebabkan atau secara unik berhubungan dengan substansi toksik Occupational toxicology Toksikologi di tempat kerja - berhub dg bhn kimia disekitar tempat kerja - terutama identifikasi “agent” - kondisi tempat kerja aman, absorbsi bahan kimia berlebih dapat dicegah - guideline konsentrasi bahan kimia di udara yang pasti aman (establish) ada daftar bahan kimia yg direkomendasikan memenuhi threshold limit values (TLVs). Guideline selalu di evaluasi new information
 ada daftar bahan kimia yg direkomendasikan. memenuhi threshold limit values (TLVs). Guideline selalu di evaluasi new information.")
36
TOKSIKOLOGI LINGKUNGAN
- berhubungan dg dampak kimia sbg polutan di lingkungan organisme hidup udara, tanah, air, dll - target utama manusia, spesias lain target biologik potensial Polusi udara produk industri pengembangan teknologi peningkatan urbanisasi Polusi tanah dan air pestisida Pengolahan makanan residu bahan kimia pada produk makanan

38
Ukrainian president Viktor Yushchenko, after alleged poisoning with dioxin, and, possibly endotoxin, prior to the 2004 elections.

39
MOLECULES OF DEATH 1. 1.Aflatoxin 2. Botulinus Toxin
3. Carbon Monoxide – Ther Silent Killer 4. Domoic Acid 5. Ecstacy 6. Heroin 7.Hydrofluoric Acid 8.Hydrogen Sulphide 9.Lead : An old and Modern Poison 10.Mercury 11.Mushroom Toxin 12.Nerve Gases 13.Nicotine and Tobacco Alkaloid 14.Paracetamol (Acetominophen) 15.Paraquat and Diquat 16.Phosphorus 17.Radon 18.Ricin 19.Snake Toxin 20.Spider Toxin 21.Strychnine 22.Tetrodotoxin 23.Thallium 24.Arsen 25.Cyanide 1.
 15.Paraquat and Diquat. 16.Phosphorus. 17.Radon. 18.Ricin. 19.Snake Toxin. 20.Spider Toxin. 21.Strychnine. 22.Tetrodotoxin. 23.Thallium. 24.Arsen. 25.Cyanide. 1.")
40
Keracunan bahan kimia di IRD RSUD Dr
Keracunan bahan kimia di IRD RSUD Dr. Soetomo Surabaya dalam 5 tahun terakhir (Hernomo, 2001) Nama Bahan 1. Pestis. 128 (32.82%) 150 (29.30%) 84 (22.11%) 75 (22.52%) 78 (31.84%) 2. Ob. Farm. 120 (30.77%) 227 (44.34%) 159 (41.84%) 137 (41.14%) 81 (33.06%) 3. Minyak 60 (15.38%) 45 (8.79%) 29 (7.63%) 38 (11.41%) 32 (13.06%) 4. Makanan 13 (3.33%) 35 (6.84%) 39 (10.26%) 23 (6.91%) 8 (3.27%) 5. Alkohol 24 (6.15%) 14 (2.73%) 22 (5.79%) 30 (9.01%) 20 (8.16%) 6. Rmh tng 8 (2.05%) 11 (2.15%) 7 (1.84%) 5 (1.50%) 3 (1.22%) 7. Gas 2 (0.51%) 4 (0.78%) 2 (0.53%) 0 (0%) 0 (0%) 8. Ob. Trad. 11 (2.82%) 3 (0.59%) 6 (1.58%) 12 (3.60%) 2 (0.82%) 9. Korosif 18 (4.62%) 14 (2.73%) 10 (2.63%) 11 (3.30%) 5 (2.04%) 10. Lain-lain 2 (0.60%) 0 (0%) 0 (0%) 0 (0%) 3 (1.22%) 11. Tak diket. 6 (1.54%) 16 (4.21%) 0 (0%) 0 (0%) 13 (5.31%) Total 390 (100%) 512 (100%) 380 (100%) 333 (100%) 245 (100%)
 Nama Bahan Pestis. 128 (32.82%) 150 (29.30%) 84 (22.11%) 75 (22.52%) 78 (31.84%) 2. Ob. Farm. 120 (30.77%) 227 (44.34%) 159 (41.84%) 137 (41.14%) 81 (33.06%) 3. Minyak 60 (15.38%) 45 (8.79%) 29 (7.63%) 38 (11.41%) 32 (13.06%) 4. Makanan 13 (3.33%) 35 (6.84%) 39 (10.26%) 23 (6.91%) 8 (3.27%) 5. Alkohol 24 (6.15%) 14 (2.73%) 22 (5.79%) 30 (9.01%) 20 (8.16%) 6. Rmh tng 8 (2.05%) 11 (2.15%) 7 (1.84%) 5 (1.50%) 3 (1.22%) 7. Gas 2 (0.51%) 4 (0.78%) 2 (0.53%) 0 (0%) 0 (0%) 8. Ob. Trad. 11 (2.82%) 3 (0.59%) 6 (1.58%) 12 (3.60%) 2 (0.82%) 9. Korosif 18 (4.62%) 14 (2.73%) 10 (2.63%) 11 (3.30%) 5 (2.04%) 10. Lain-lain 2 (0.60%) 0 (0%) 0 (0%) 0 (0%) 3 (1.22%) 11. Tak diket. 6 (1.54%) 16 (4.21%) 0 (0%) 0 (0%) 13 (5.31%) Total 390 (100%) 512 (100%) 380 (100%) 333 (100%) 245 (100%)")
42
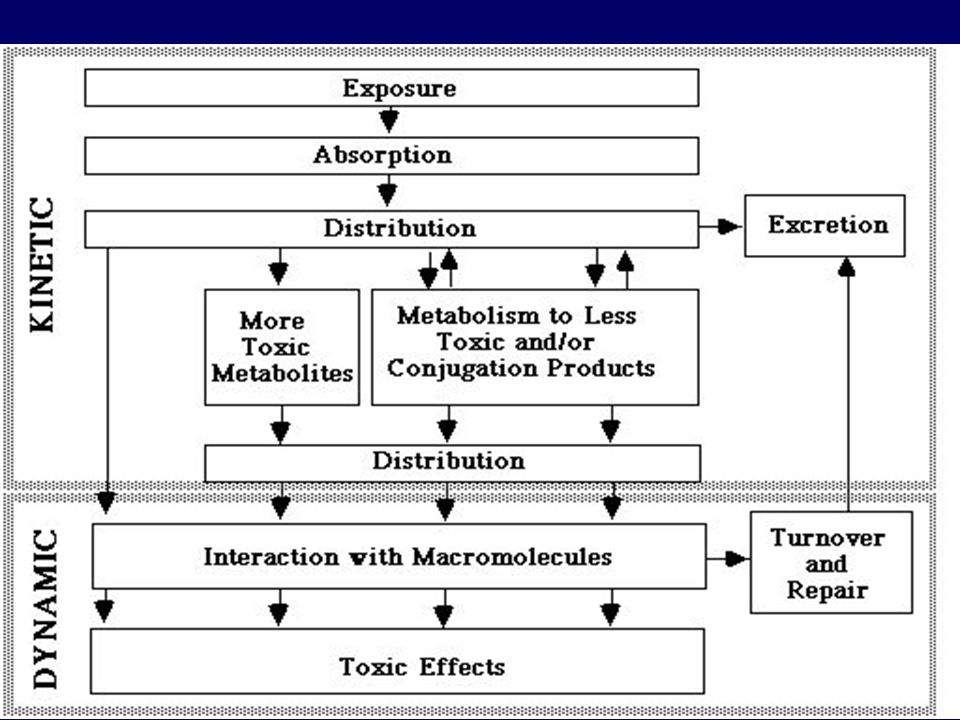
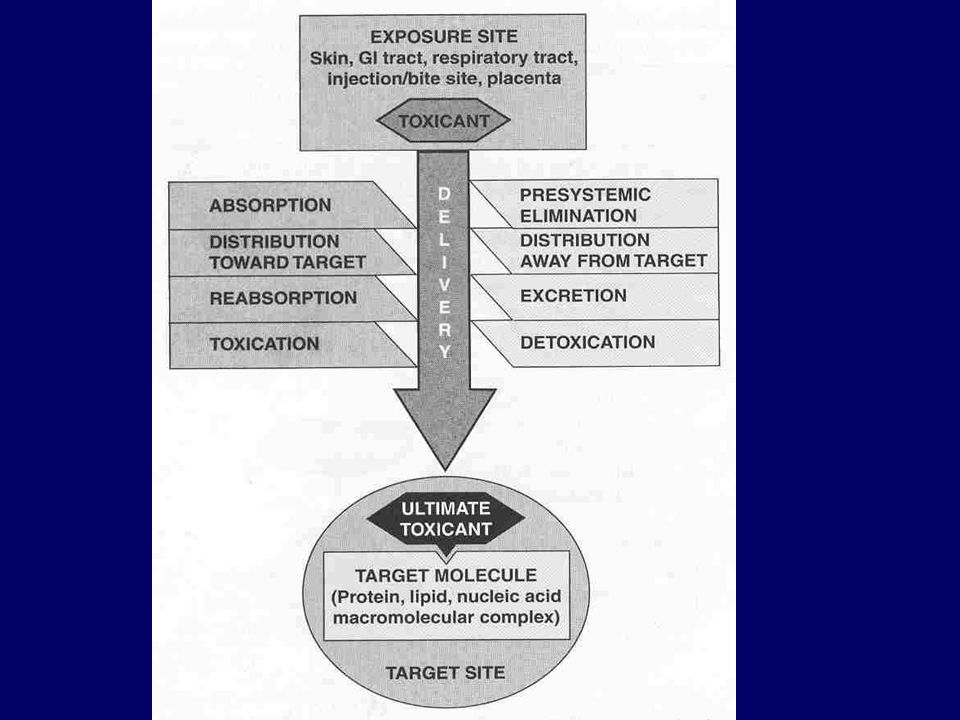
TOXICOKINETICS AND TOXICODYNAMIC
Bagaimana toksikan memasuki tubuh ? Bagaimana nasib toksikan didlm tubuh ? Bagaimana efek tubuh terhadap terhadap toxicant ? Bagaimana efek toksikan terhadap tubuh ? Bagaimana cara penanganan intoksikasi ? Dll

44
TOXICOKINETICS (TOKSIKOKINETIK)
Studi pengaruh tubuh terhadap toksikan dan pergerakan toksikan didalam tubuh MTC Therapeutic MEC Ineffective

46
Bioaccumulation = the accumulation of a contaminant or toxin in or on an organism from all sources (e.g., food, water, air). Biomagnification = the increase in concentration of toxin as it passes through successive levels of the food web

47
Assimilation Efficiency (= Lindeman’s Efficiency
Bioaccumulation Assimilation Efficiency (= Lindeman’s Efficiency Lindeman Ecology 23: ) AE increases with trophic level When a chemical is assimilated more efficiently than organic energy -> bioaccumulation AE
 AE increases with trophic level. When a chemical is assimilated more efficiently than. organic energy -> bioaccumulation. AE.")
48
Scenario 1: Alewife (2o predator) eats Cercopagis 1o predator
Biomagnification Scenario 1: Alewife (2o predator) eats Cercopagis 1o predator cals. 1 10 100 ppm toxin 1 100 10,000 Scenario 2 cals. 1 100 ppm toxin 1000 1
 eats Cercopagis 1o predator. cals ppm toxin ,000. Scenario 2. cals ppm toxin")
49
Food Web Bioaccumulation

50
The Mercury Cycle

51
TOXICOKINETICS: Study of the time-course of toxins (study of what the body does to the toxin).
.")
52
TOXICODYNAMICS (TOKSIKODINAMIK)
Studi efek pengaruh toksikan terhadap tubuh

53
TOXICODYNAMICS: Study of biochemical and physiological effects of drugs and toxins (study of what the toxin does to the body).
.")
54
Target Organ Toxicity -Central Nervous System – lead
-Immune System - isocyanates -Liver - ethanol, acetaminophen -Respiratory Tract - tobacco smoke, asbestos, ozone -Eye - UV light (sunlight) -Kidney - metals -Skin - UV light, gold, nickel -Reproductive System –dibromochloropropane
 -Kidney - metals. -Skin - UV light, gold, nickel. -Reproductive System –dibromochloropropane.")
55
Karakteristik Rute Pemaparan Toksikan (Exposure)
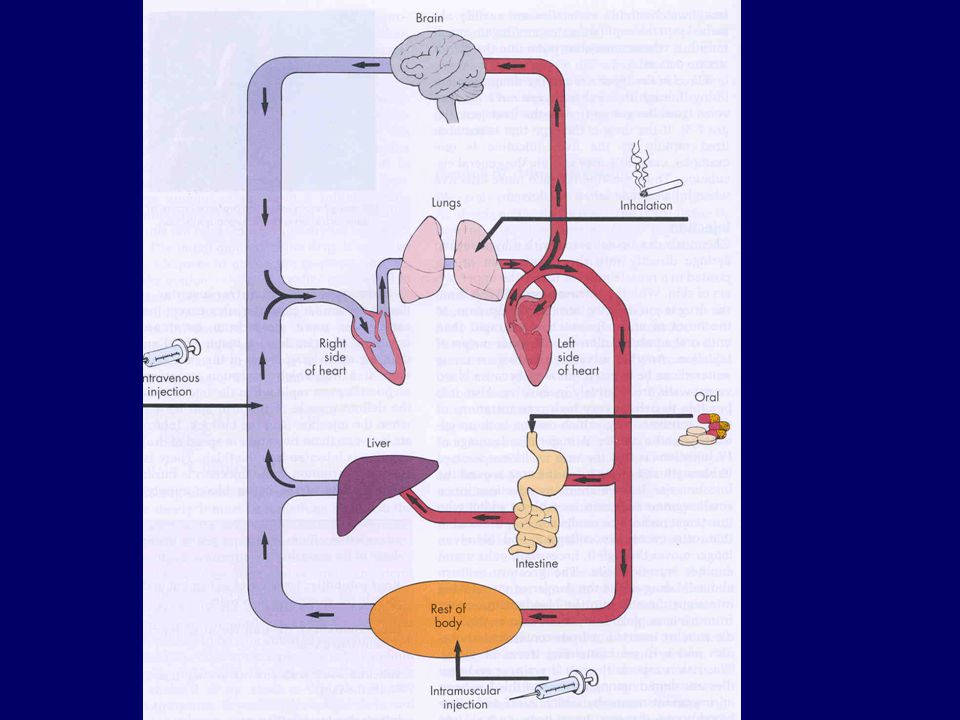
Rute dan Titik tangkap Pemaparan Ingestion (Gastrointestinal Tract) Inhalation (Lungs) Dermal/Topical (Skin) Injection intravenous, intramuscular, intraperitoneal Effectiveness pemaparan: iv > inhale > ip > im > ingest > topical
 Inhalation (Lungs) Dermal/Topical (Skin) Injection. intravenous, intramuscular, intraperitoneal. Effectiveness pemaparan: iv > inhale > ip > im > ingest > topical.")
56
Dosis Jumlah bahan kimia / Toxicant yang memasuki tubuh Umumnya dalam satuan mg /kg BW Dosis Toxicant tergantung pada bbp faktor : concentration di lingkungan sekitarnya Karakteristik exposure Lama exposure Frekwensi exposure Sifat toxicant

57
Toxicant Toxicant Toxicant

58
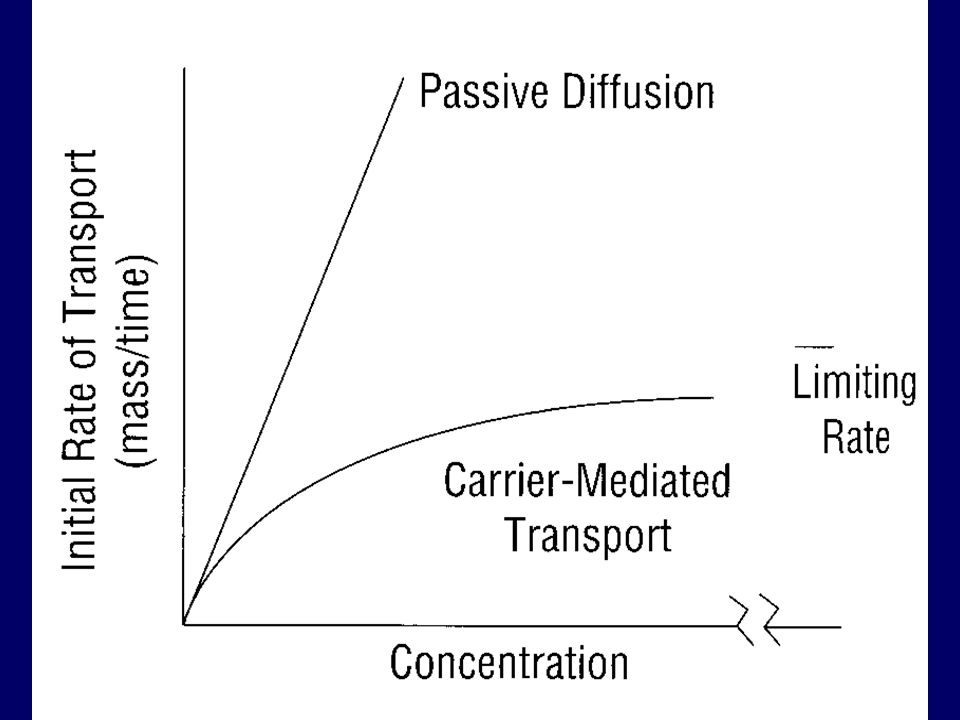
Passive diffusion MEKANISME TRANSPORT DARI TOXICANT Carrier-mediated
Active Facilitated ATP ADP-Pi Transporter Molecule

59
Memerlukan carrier Transport menjadi jenuh (saturated) pada konsentrasi tinggi Proses bersifat selective Dua obat yang ditranspor oleh mekanisme yg sama akan menghambat satu sama lain Melawan concentration gradient ( active transport) Tdk melawan cocentration gradient ( facilitated transport) Memerlukan energy Mekanisme transport dapat dihambat oleh obat obat yang mempengaruhi cellular metabolism Karakteristik facilitated diffusion dan active transport
 Tdk melawan cocentration gradient ( facilitated. transport) Memerlukan energy. Mekanisme transport dapat dihambat oleh obat obat yang mempengaruhi cellular metabolism. Karakteristik facilitated diffusion dan active transport.")
60
Karakteristik dari molekul Un-ionized
Dan Ionized Toxicant Un-ionized Ionized Pharmacologic effect Active Inactive Solubility Lipids Water Cross lipid barriers Yes No (gastrointestinal tract, blood-brain barrier, placenta) Hepatic metabolism Yes No Renal excretion No Yes
 Hepatic metabolism Yes No. Renal excretion No Yes.")
62
Absorption: Kemampuan bhn kimia memasuki darah (darah berkesimbangan dgn jaringan)
Inhalasi--gas menuju darah melalui alveoli. (luas permukaan alveolar, aliran darah banyak, lapisan antara darah menuju alveolar air) Ingestion--absorpsi melalui GI tract : stomach (asam), small intestine (contact time panjang, luas permukaan luas--villi; bases dan transporter bahan bahan tertentu) 1st Pass Effect (liver metabolism) Dermal—absorpsi melalui epidermis (stratum corneum), dermis; titik tangkap dan keadaan kulit
 Ingestion--absorpsi melalui GI tract : stomach (asam), small intestine (contact time panjang, luas permukaan luas--villi; bases dan transporter bahan bahan tertentu) 1st Pass Effect (liver metabolism) Dermal—absorpsi melalui epidermis (stratum corneum), dermis; titik tangkap dan keadaan kulit.")
64
Respiratory System Surface area approximately 50 to 100 m2 Nasopharynx
Oropharynx Epiglottis Thyroid cartilage Larynx Cricoid cartilage Trachea Bronchiole Left main bronchus Right main bronchus Bronchiole Diaphragm Lungs Alveolus Alveolar sac

65
Respiratory Physiology
CO 2 2 2 . CO 2 Blood from right side of heart Aveolus (low in O, 2 high in CO) O O 2 2 2 CO Blood to left CO 2 2 side of heart Reoxygenated blood (high in O, low in CO) Capillary 2 2 Red blood cells
 O. O CO. Blood to left. CO side of heart. Reoxygenated blood. (high in O, low in CO) Capillary Red blood cells.")
66
Absorpsi Pulmonary Systemic (e.g. insulin, anesthetics)
dan local delivery Area absorpsi sangat luas Suplai darah sangat baik Tidak mengalami first pass effect Bentuk sediaan mahal Ukuran partikel : 2-5 m

67
Absorption from the Lungs
REMOVAL OF PARTICLES Absorption of Aerosols and Particles: 1- Particle Size 2- Water solubility of the chemical present in the aerosol or particle Lymph Physical Phagocytosis

68
Pemberian per inhalasi
Patikel > 10 um : diendapkan, dihembuskan dan berbangkis Partikel < 0.01 um : terbuang pada saat inspirasi dan ekspirasi Partikel 0.01 – 10 um :diendapkan pada alveoli, nasopharyng sampai bronchioli 25% dikeluarkan bersama udara nafas 50% diendapkan disalurannafas bagian atas 25% diendapkan disaluran nafas bagian bawah

69
Absorpsi dari Paru Gas, vapors,volatile liquids, aerosols and particles Large surface area, thin barrier, high blood flow rapid absorption Blood:air partition coefficient – dipengaruhi respiratory rate dan blood flow Blood:tissue partition coefficient

70
NasopharyngealRegion
DEPOSISI PARTIKEL TOKSIKAN DI DLM SALURAN RESPIRASI NasopharyngealRegion 5-30 µm Trachea Bronchi Bronchioles 1-5 µm Alveolar Region 1 µm

72
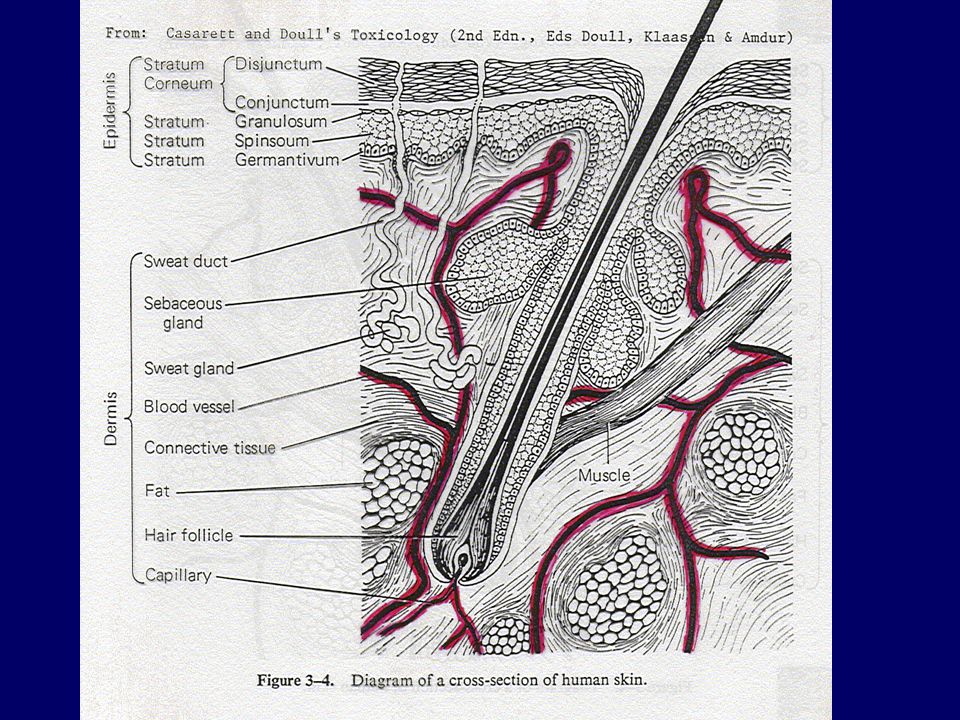
Absorpsi dari kulit Melewati bbg lapisan sel (stratum corneum, epidermis, dermis) menuju pembuluh darah . Faktor yang mempengaruhi : lipid solubility, hydrasi kulit (sole of feet vs. scrotum)
")
74
Absorption by the Skin

75
Absorpsi melalui kulit
Permeability depends on the diffusivity and thickness (depends on the area of the body) of the stratum corneum Polar outer surface of protein filaments of the hydrated stratum corneum Nonpolar lipid matrix between protein filaments Percutaneous absorption lower layers of the epidermis and dermis Below the s.corneum porous, nonselective aqueous medium Compromised stratum corneum integrity Increased stratum corneum hydration Increased temperature increased blood flow Low solubility of toxicant in the vehicle Small size Increased Absorption
 of the stratum corneum. Polar outer surface of protein filaments of the hydrated stratum corneum. Nonpolar lipid matrix between protein filaments. Percutaneous absorption lower layers of the epidermis and dermis. Below the s.corneum porous, nonselective aqueous medium. Compromised stratum corneum integrity. Increased stratum corneum hydration. Increased temperature increased blood flow. Low solubility of toxicant in the vehicle. Small size Increased Absorption.")
76
Kecepatan distribusi Toxicant tergantung : -- aliran darah
Distribution: proses translokasi dari Toxicant menuju seluruh bagian tubuh Darah membawa Toxicant menuju site of action, storage depots, organ transformasi, dan organ eliminasi Kecepatan distribusi Toxicant tergantung : -- aliran darah karakteristik toxicant (afinitas thd jaringan dan partition coefficient) Distribusi mungkin berubah setiap waktu
 Distribusi mungkin berubah setiap waktu.")
77
Distribusi: Storage / Binding
Storage di dlm Adipose tissue sangat lipophylic (DDT). Cepat dimobilisasi dari fat (starvation) , cepat meningkat dalam darah cepat meningkat dalam darah Storage dalam tulang (Bone) Chemicals analog dgn Calcium--Fluoride, Lead, Strontium Ikatan dgn Plasma proteins mendesak senyawa endogenous . Hanya fraksi bebas adverse effects dan excretion
. Cepat dimobilisasi dari fat (starvation) , cepat meningkat dalam darah cepat meningkat dalam darah. Storage dalam tulang (Bone) Chemicals analog dgn Calcium--Fluoride, Lead, Strontium. Ikatan dgn Plasma proteins mendesak senyawa endogenous . Hanya fraksi bebas adverse effects dan excretion.")
78
Metabolism: Toxicant lebih water soluble (Polar) ekskresi
Menurunkan lipid solubility menurunkan jumlah toxicant pada target Meningkatkan ionisasi meningkatkan excretion rate --> menurunkan toxicity Bioactivasi Biotransformasi pembentukan reactive metabolites

79
Biotransformation (Metabolism)
Meningkatkan kec clearance dari toxicant Dapat terjadi mulai absorpsi ekskreri

80
Biotransformation Key organs in biotransformation
LIVER (high) Lung, Kidney, Intestine (medium) Others (low) Biotransformation Pathways Phase I--make the toxicant more water soluble Phase II--Links with a soluble endogenous agent (conjugation)
 Lung, Kidney, Intestine (medium) Others (low) Biotransformation Pathways. Phase I--make the toxicant more water soluble. Phase II--Links with a soluble endogenous agent (conjugation)")
81
FPE Beberapa toxin tidak efektif bila digunakan peroral (snake venome)
Bila toxicant dimetabolisme menjadi bentuk aktif (ultimate toxicant) kumulatif dari metabolit toxic
 kumulatif dari metabolit toxic.")
84
Distribution: the process in which a chemical agent translocates throughout the body
Blood carries the agent to and from its site of action, storage depots, organs of transformation, and organs of elimination Rate of distribution (rapid) dependent upon blood flow characteristics of toxicant (affinity for the tissue, and the partition coefficient) Distribution may change over time
 dependent upon. blood flow. characteristics of toxicant (affinity for the tissue, and the partition coefficient) Distribution may change over time.")
85
Distribution: Storage and Binding
Storage in Adipose tissue--Very lipophylic compounds (DDT) will store in fat. Rapid mobilization of the fat (starvation) can rapidly increase blood concentration Storage in Bone--Chemicals analogous to Calcium--Fluoride, Lead, Strontium Binding to Plasma proteins--can displace endogenous compounds. Only free is available for adverse effects or excretion
 will store in fat. Rapid mobilization of the fat (starvation) can rapidly increase blood concentration. Storage in Bone--Chemicals analogous to Calcium--Fluoride, Lead, Strontium. Binding to Plasma proteins--can displace endogenous compounds. Only free is available for adverse effects or excretion.")
86
Target Organs: adverse effect is dependent upon the concentration of active compound at the target site for enough time Not all organs are affected equally greater susceptibility of the target organ higher concentration of active compound Liver--high blood flow, oxidative reactions Kidney--high blood flow, concentrates chemicals Lung--high blood flow, site of exposure Neurons--oxygen dependent, irreversible damage Myocardium--oxygen dependent Bone marrow, intestinal mucosa--rapid divide

87
Target organ Carbon tetrachloride – liver Mercury & lead – CNS, kidneys & hematopoietic system Benzene – hematopoietic system Storage sites Dichlorodiphenyltrichloroethane (DDT) – fat depots no toxic effect
 – fat depots no toxic effect.")
88
Lungs are capable of biotransformation & elimination
Nose is a “scrubber” for water-soluble and highly reactive gases Solubility ratio (blood-to-gas partition coefficient) – conc. in blood/conc. in gas phase before or at saturation Low solubility ratio – blood flow through the lungs (perfusion-limited) Highs solubility ratio – rate and depth of respiration (ventilation-limited) Lungs are capable of biotransformation & elimination Steady state concentration can be reached Aerosols dependent on aerosol size & water solubility 5um or more – lodged in nasopharyngeal region 2.5 um – tracheobronchial region 1 um or less – alveolar sacs of blood
 – conc. in blood/conc. in gas phase before or at saturation. Low solubility ratio – blood flow through the lungs (perfusion-limited) Highs solubility ratio – rate and depth of respiration (ventilation-limited) Lungs are capable of biotransformation & elimination. Steady state concentration can be reached. Aerosols dependent on aerosol size & water solubility. 5um or more – lodged in nasopharyngeal region. 2.5 um – tracheobronchial region. 1 um or less – alveolar sacs of blood.")
89
Efek Toxic Berdasarkan Mekanisme
Allergic (hypersensitivity,Antigen) Idiosyncratic (e.g. G6PD def., Drugs) Local vs. Systemic (Corrosive agent) Reversible vs. Irreversible Necrosis /organ damage (Ozone, Lead, Cd, Sr) Carcinogenecity (Benzene, Rokok, Asbestos, Coloring Agent) Mutagenicity (uv light, Coloring Agent) Teratogenicity (Drugs:Thalidomide, Valproic acid, Herbal) Death (Arsen, Cyanide) 89
 Idiosyncratic (e.g. G6PD def., Drugs) Local vs. Systemic (Corrosive agent) Reversible vs. Irreversible. Necrosis /organ damage (Ozone, Lead, Cd, Sr) Carcinogenecity (Benzene, Rokok, Asbestos, Coloring Agent) Mutagenicity (uv light, Coloring Agent) Teratogenicity (Drugs:Thalidomide, Valproic acid, Herbal) Death (Arsen, Cyanide) 89.")
90
Efek Toksik Berdasarkan Lama Pemaparan (Exposure)
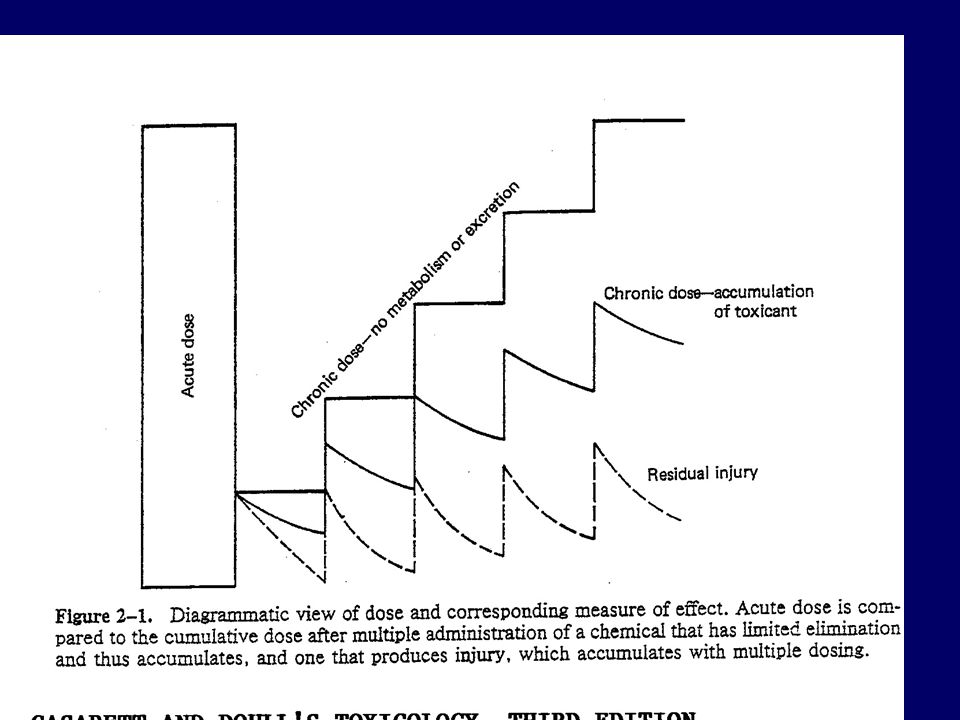
Acute toxicity < 24hr umumnya 1 x paparan Subacute toxicity bulan dosis berulang Subchronic toxicity 1-3 bulan dosis berulang Chronic toxicity > 3 bulan dosis berulang Pada pemakaian berulang akumulasi Toxicant didalam tubuh

91
Sifat Toxicant Acute Toxicity
Biasanya menyebabkan kematian Th 1989, 5,000 orang meninggal dan 30,000 cacat permanen akibat terpapar methyl isocyanate akibat kebocoran industri di India. Subchronic Toxicity - Minum coumadin tablets (blood thinners) beberapa minggu pada pengobatan venous thrombosis menyebabkan perdarahan internal . Chronic Toxicity - cirrhosis pada alcoholics (beberapa tahun) - chronic kidney disease pada pekerja terpapar Pb beberapa tahun - chronic bronchitis pada cigarette smokers - pulmonary fibrosis pada pekerja tambang (black lung disease) - Carcinogenicity, Mutagenicity - Developmental Toxicity, Teratogenicity Embryolethality,embryotoxic,teratogenic - Genetic Toxicity (somatic cells) Gene mutation,chromosome aberration,aneuploidy,polyploidy
 beberapa. minggu pada pengobatan venous thrombosis menyebabkan. perdarahan internal . Chronic Toxicity - cirrhosis pada alcoholics (beberapa tahun) - chronic kidney disease pada pekerja terpapar Pb beberapa tahun - chronic bronchitis pada cigarette smokers - pulmonary fibrosis pada pekerja tambang (black lung disease) - Carcinogenicity, Mutagenicity. - Developmental Toxicity, Teratogenicity Embryolethality,embryotoxic,teratogenic. - Genetic Toxicity (somatic cells) Gene mutation,chromosome aberration,aneuploidy,polyploidy.")
93
Target Organs: adverse effect tergantung pada kadar senyawa aktif dlm target site untuk waktu yang cukup Tidak semua organ dipengaruhi sama ,tetapi tergantung Kepekaan target organ Kadar toxicant yg tinggi dalam target organ Liver—aliran drh sangat tinggi,oxidative reactions Kidney—aliran drh sangat tinggi, bhn kimia terkonsentrat Lung--high blood flow, tempat pemaparan Neurons--oxygen dependent, kerusakan irreversible Myocardium--oxygen dependent Bone marrow, intestinal mucosa -- rapid divide cell

94
Target Sites: Mechanisms of Action
Adverse effects can occur at the level of the molecule, cell, organ, or organism Molecularly, chemical can interact with Proteins Lipids DNA Cellularly, chemical can interfere with receptor-ligand binding interfere with membrane function interfere with cellular energy production bind to biomolecules perturb homeostasis (Ca)
")
95
Excretion: Toxicants are eliminated from the body by several routes
Urinary excretion water soluble products are filtered out of the blood by the kidney and excreted into the urine Exhalation Volatile compounds are exhaled by breathing Biliary Excretion via Fecal Excretion Compounds can be extracted by the liver and excreted into the bile. The bile drains into the small intestine and is eliminated in the feces. Milk Sweat Saliva Excretion: Toxicants are eliminated from the body by several routes

96
Mekanisme kerusakan sel (cellular injury)
Perubahan permeabilitas cell membrane Perubahan enzymes activity. Modifikasi carriers. Reaksi yg menyebabkan deplesi GSH. Interaksi dgn co-enzyme. Interaksi dgn nucleic acid. Pembentukan reactive metabolite. Perubahan protein synthesis. Immunotoxicity. Perubahan Lysosomal Inhibisi cellular respiration.

97
Occupancy Theory T + R T-R Complex Response

98
Law of Mass Action R + T RT [R].[T].kf [RT].kb Kec. asosiasi = [R].[T].kf Kec. disosiasi = [RT].kb Pada keseimbangan [R].[T].kf = [RT].kb Keduanya dibagi dengan kf [R].[T]=[RT].kb/kf (1)
![Law of Mass Action R + T RT. [R].[T].kf. [RT].kb. Kec. asosiasi = [R].[T].kf. Kec. disosiasi = [RT].kb.](http://slideplayer.info/slide/3305930/11/images/98/Law+of+Mass+Action+R+%2B+T+RT.+%5BR%5D.%5BT%5D.kf.+%5BRT%5D.kb.+Kec.+asosiasi+%3D+%5BR%5D.%5BT%5D.kf.+Kec.+disosiasi+%3D+%5BRT%5D.kb..jpg "Pada keseimbangan [R].[T].kf = [RT].kb. Keduanya dibagi dengan kf [R].[T]=[RT].kb/kf (1)")
99
Let Kd = kb/kf [R].[T]=[RT].Kd (2)
[Rt] = total no. receptors [Rt] = [R] + [RT] Subst [R] = [Rt]-[RT] ke (2) [T]([Rt]-[RT]) = [RT].Kd Selanjutnya [RT](Kd+[T]) = [T].[Rt] Dibagi dengan [Rt] [RD](Kd+[T])/[Rt] = [T] Dibagi oleh (Kd + [T]) [RT] = [T] [Rt] [T] + Kd Besarnya efek toksik sebanding dengan komplek TR yaitu E ~ [TR] Respon maximum terjadi bila semua reseptor diduduki toksikan, yaitu Emax ~ [Rt] Fraksi reseptor yang diduduki toxicant = efek = respon = RT / Rt
![Let Kd = kb/kf [R].[T]=[RT].Kd (2)](http://slideplayer.info/slide/3305930/11/images/99/Let+Kd+%3D+kb%2Fkf+%5BR%5D.%5BT%5D%3D%5BRT%5D.Kd+%282%29.jpg "[Rt] = total no. receptors [Rt] = [R] + [RT] Subst [R] = [Rt]-[RT] ke (2) [T]([Rt]-[RT]) = [RT].Kd. Selanjutnya [RT](Kd+[T]) = [T].[Rt] Dibagi dengan [Rt] [RD](Kd+[T])/[Rt] = [T] Dibagi oleh (Kd + [T]) [RT] = [T] [Rt] [T] + Kd. Besarnya efek toksik sebanding dengan komplek TR yaitu E ~ [TR] Respon maximum terjadi bila semua reseptor diduduki toksikan, yaitu Emax ~ [Rt] Fraksi reseptor yang diduduki toxicant = efek = respon = RT / Rt.")
101
Model dari “Occupancy Theory”
Toxicant

102
Dose Response Relationship
All Effected 100 80 75 % Response 50 Half Effected 25 NO Adverse Effect level 20 10 20 30 40 50 60 70 80 90 100 Dose (mg/kg body weight) Increasing dose
 Increasing dose.")
103
Dose-response relationship: LEAD (Pb)
decreased erythrocyte delta-ALAD activity increased zinc protoporphyrin anemia CNS effects decreased peripheral nerve conductivity Nervous paralysis, lead colics Adapted from Elinder C-G et al., Biologisk monitoring av metaller hos människa. Arbetsmiljöfonden, Uppsala, 1991

106
Maximum Effect atau Efficacy
Kurva Dosis-Efek ( in vivo) Maximum Effect atau Efficacy Slope Effect Potency Log Dose
 Maximum Effect atau Efficacy. Slope. Effect. Potency. Log Dose.")
107
Kurva Dose - Respon in vivo ( Efficacy & Potency )
")
108
Perbedaan Potensi Dose Dioxine Rattle snake Strychnine Sulfate
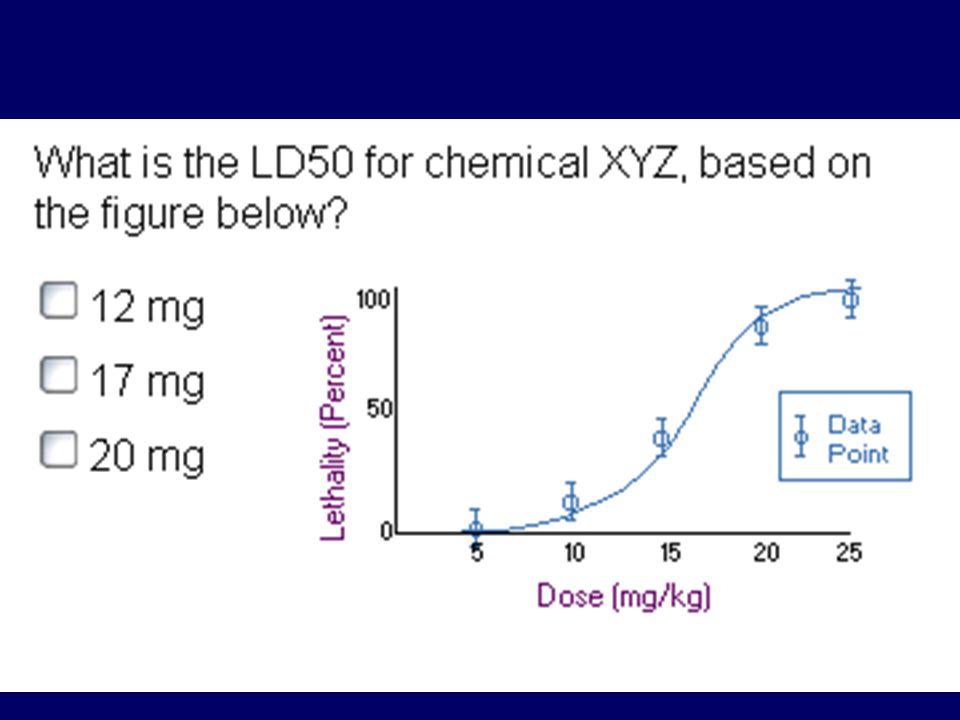
100 Strychnine Sulfate Ethyl Alcohol % of Lethality 50 LD50 Dose

109
Hubungan Dosis-Efek : Phenobarbital
Therapeutic Index: LD50 ED50 Hipnotik Mati % Respon ED50 LD50 Dosis Phenobarbital

110
Toxicity Studies Acute Toxicity
LD 50,Max Tolerated Dose,2 species,2 route, single dose Subacute Toxicity 3 doses,2 doses, 4 weeks-3 months, Chronic Toxicity Rodent,non-rodent, 6 months and more Effect on reproductive performance Effects on animal mating behavior,reproduction,parturition,progeny,birth defects,postnatal development Carcinogenic potential 2 years, 2 species Mutagenic potential Effects on genetic stability and mutations in bacteria (Ames test) or mammalian cells in culture, dominant lethal test and clastogenicity in mice Investigative Toxicology Determine sequence and mechanisms of toxic action, etc
 or mammalian cells in culture, dominant lethal test and clastogenicity in mice. Investigative Toxicology. Determine sequence and mechanisms of toxic action, etc.")
111
Qualitative Observation
Body Weight and Food Consumption Ophthalmology interval Hematology parameters Clinical Chemistry Parameters Urinalysis Parameters Organ Weight Microscopic Pathology Animal Responses Clinical Signs of Toxicity Autonomic Signs Etc CRC Handbook of Toxicology,2005

112
Quantitative Observation
Acute Toxicity ED-50, LD-50, TI Sub Chronic and Chronic Toxicity ADI, NOEL, NOAEL CRC Handbook of Toxicology,2005

113
Acute Toxicity - Acute toxicity dilakukan pertama kalinya (biasanya oral dan IV) - Menentuklan harga LD Binatang coba mati dlm waktu 7-14 hari period after a single dose is tabulated. - Tanda tanda intoksikasi, lethargy, perubahan perilaku, studi biokimia harus dilakukan

114
(short-term exposure)
Acute Toxicity: (short-term exposure) 114
 114.")
115
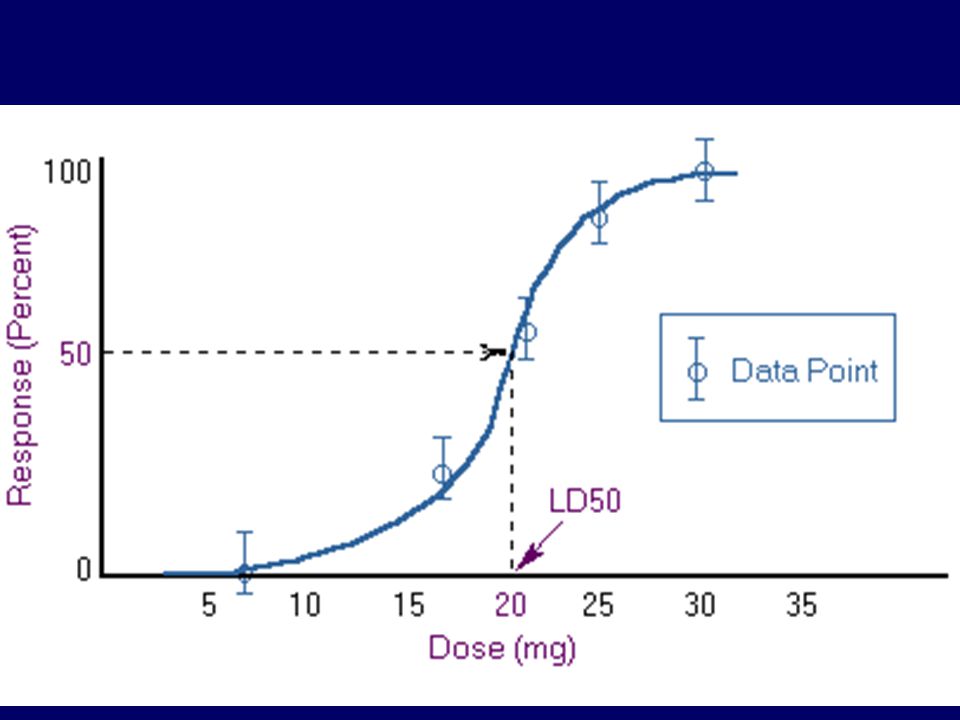
LD50 Quantal responses dihitung bila data dari populasi. Bila mortality berupa response, maka dosis pada 50% dari populasi LD50 LD 50 paling kecil paling toxic Therapeutic Index (TI) is the ratio of the dose required to produce a toxic effect to that required to produce a desired therapeutic response(LD50/ED50)
 is the ratio of the dose required to produce a toxic effect to that required to produce a desired therapeutic response(LD50/ED50)")
116
LD50 berbagai bahan kimia
Toxicant LD50 (mg/kg) Ethyl alcohol 10,000 Salt (sodium chloride) 4,000 Iron (Ferrous sulfate) 1,500 Morphine Mothballs (paradichlorobenzene) 500 Aspirin DDT Cyanide 10 Nicotine 1 Black Widow Spider venom 0.55 Rattle Snake venom Tetrodotoxin (from fish) 0.01 Dioxin (TCDD) Botulinum Toxin
 Ethyl alcohol 10,000. Salt (sodium chloride) 4,000. Iron (Ferrous sulfate) 1,500. Morphine 900. Mothballs (paradichlorobenzene) 500. Aspirin 250. DDT 250. Cyanide 10. Nicotine 1. Black Widow Spider venom Rattle Snake venom Tetrodotoxin (from fish) Dioxin (TCDD) Botulinum Toxin")
117
Subchronic toxicity tests
Uji toksisitas selama 90 hari Dua species (rats dan dogs) 3 dosis level Tiap dosis minimum 15 binatang (jantan/betina) Pengamatan : Mortality, body weight, diet consumption, hematology dan clinical chemistry. Pemeriksaan Gross dan microscopic dari tiap organs dan jaringan.
 3 dosis level. Tiap dosis minimum 15 binatang (jantan/betina) Pengamatan : Mortality, body weight, diet consumption, hematology dan clinical chemistry. Pemeriksaan Gross dan microscopic dari tiap organs dan jaringan.")
118
Long term / chronic exposure studies
Dilakukan mirip dengan pengamatan pada studi sub chronic, kecuali dengan periode lebih lama . Mis, uji toksisitas Antimicrobial agents dan food additives. Terutama penentuan carcinogenic potential Dilakukan pada tikus, mice, spesies lainnya selama life spent (masa hidup) dari tiap spesies
 dari tiap spesies.")
119
Chronic Toxicity: (repeated exposures) 119
 119")
120
Dose levels (animal studies)
NOEL no-observed effect level NOAEL no-observed-adverse effect level LOAEL lowest-observed-adverse effect level MTD maximum tolerated dose LD dose which kills 50% of population LC concentration which kills 50% of population; must include time frame Increasing dose 120

123
Toxicity Rating Chart (Casarett & Doulls)
Clasification Probable lethal oral dose for humans Dosage For average adult Toxicity rating/ Class Practically non toxic > 15 g/kg More than 1 quart Slightly toxic 5 – 15 g/kg Between pint and quart Moderately toxic 0.5 – 5 g/kg Between ounce and quart Very toxic 50 – 500 mg/kg Between teaspoonful and ounce Extremely toxic 5 – 50 mg/kg Between 7 drops and teaspoonful Supertoxic < 5 mg/kg A taste (less than 7 drops)
")
124
Uji Dermal dan Ocular - Uji Dermal biasanya umumnya dilakukan pada kelinci. Chemical toxicant dikenakan pada kulit dean dibiarkan kontak selama jam. - Iritasi kulit ditandai dengan adanya erythema scar, pembentukan edema, sifat corrosive - Pada Ocular test, toxicant diteteskan pada satu mata dan lainnya sebagai kontrol pada kelinci Perubahan pada mata diamati pada beberapa interval ttt

126
Qualitative Observation
Body Weight and Food Consumption Ophthalmology interval Hematology parameters Clinical Chemistry Parameters Urinalysis Parameters Organ Weight Microscopic Pathology Animal Responses Clinical Signs of Toxicity Autonomic Signs Etc CRC Handbook of Toxicology,2005

128
Toxicity rating Toxicity rating or class Dosage for average adult
Probable lethal oral dose for human Dosage for average adult 1. Practically nontoxic > 15 g/kg more than 1 quart (>0.94 L) 2. Slightly toxic 5-15 g/kg between pint and quart ( L) 3. Moderately toxic 0.5-5 g/kg between ounce and pint (28 mL-0.47L) 4. Very toxic mg/kg between teaspoon and ounce (5-28 mL) 5. Extremely toxic 5-50 mg/kg between 7 drops and teaspoon 6. Supertoxic < 5 mg/kg a taste (less than 7 drops) 128
 2. Slightly toxic g/kg. between pint and quart ( L) 3. Moderately toxic g/kg. between ounce and pint (28 mL-0.47L) 4. Very toxic mg/kg. between teaspoon and ounce (5-28 mL) 5. Extremely toxic mg/kg. between 7 drops and teaspoon. 6. Supertoxic. < 5 mg/kg. a taste (less than 7 drops) 128.")
Presentasi serupa