Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
PELVIC ORGAN PROLAPS

2
Risk Factors Pregnancy Vaginal childbirth
Menopause ( Aging, Hypoestrogenism Chronically increased intra-abdominal pressure (COPD, Constipation, Obesity )
")
3
Risk Factors Pelvic floor trauma Genetic factors Race
Connective tissue disorders Hysterectomy Spina bifida

4
Drawing displays the anatomic landmarks used during pelvic organ prolapse quantification (POP-Q).
.")
5
Grid system used for charting in pelvic organ prolapse quantification (POP-Q).
.")
6
The Pelvic Organ Prolapse Quantification (POP-Q) Staging System of Pelvic Organ Support
Stage 0: No prolapse is demonstrated. Points Aa, Ap, Ba, and Bp are all at –3 cm and either point C or D is between –TVL (total vaginal length) cm and –(TVL–2) cm (i.e., the quantitation value for point C or D is –[TVL – 2] cm).
 cm and –(TVL–2) cm (i.e., the quantitation value for point C or D is –[TVL – 2] cm).")
7
The Pelvic Organ Prolapse Quantification (POP-Q) Staging System of Pelvic Organ Support
Stage I: The criteria for stage 0 are not met, but the most distal portion of the prolapse is >1 cm above the level of the hymen (i.e., its quantitation value is < – 1 cm). Stage II: The most distal portion of the prolapse is 1 cm proximal to or distal to the plane of the hymen (i.e., its quantitation value is –1 cm but +1 cm).
. Stage II: The most distal portion of the prolapse is 1 cm proximal to or distal to the plane of the hymen (i.e., its quantitation value is –1 cm but +1 cm).")
8
The Pelvic Organ Prolapse Quantification (POP-Q) Staging System of Pelvic Organ Support
Stage III: The most distal portion of the prolapse is >1 cm below the plane of the hymen but protrudes no further than 2 cm less than the total vaginal length in centimeters (i.e., its quantitation value is > + 1 cm but < + [TVL–2] cm).
.")
9
The Pelvic Organ Prolapse Quantification (POP-Q) Staging System of Pelvic Organ Support
Stage IV: Essentially, complete eversion of the total length of the lower genital tract is demonstrated. The distal portion of the prolapse protrudes to at least (TVL–2) cm (i.e., its quantitation value is +[TVL–2] cm). In most instances, the leading edge of stage IV prolapse will be the cervix or vaginal cuff scar
 cm (i.e., its quantitation value is +[TVL–2] cm). In most instances, the leading edge of stage IV prolapse will be the cervix or vaginal cuff scar.")
10
Baden-Walker Halfway System for the Evaluation of Pelvic Organ Prolapse on Physical Examinationa
Grade 0 Normal position for each respective site Grade 1 Descent halfway to the hymen Grade 2 Descent to the hymen Grade 3 Descent halfway past the hymen Grade 4 Maximum possible descent for each site

11
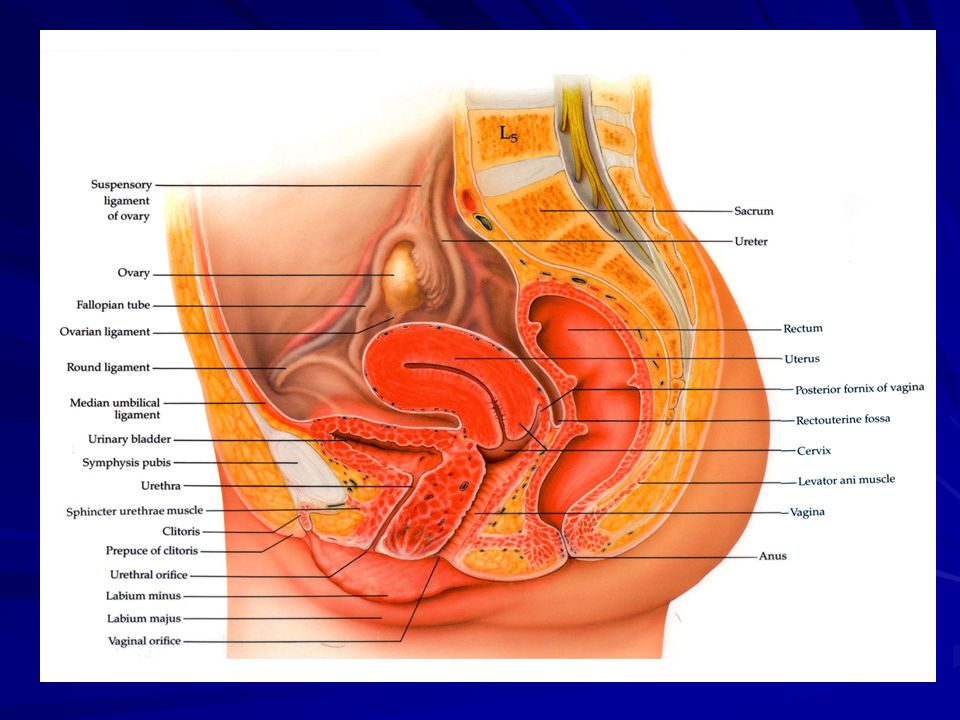
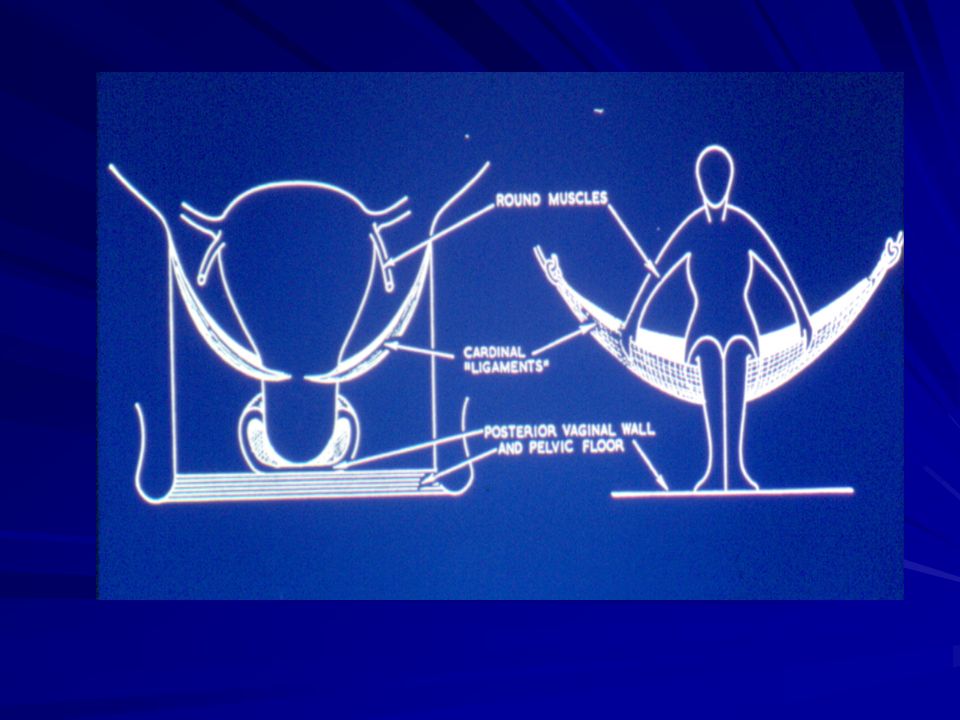
Pathophysiology Pelvic organ support is maintained by complex interactions between the levator ani muscle, vagina, and pelvic floor connective tissue. However, these mechanisms have not been fully delineated.

12
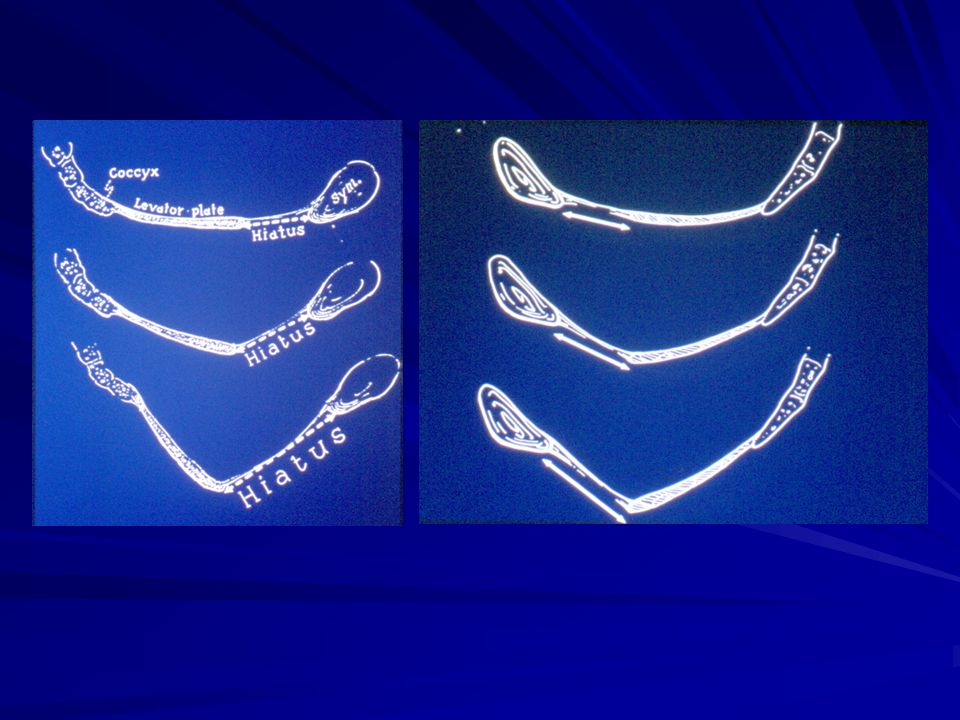
Mechanism of Levator Ani Damage
Skeletal muscle is a dynamic tissue that is constantly remodeling and regenerating. A heterogeneous population of fibers with different functions allows skeletal muscle to adapt to different situations, such as stretch and mechanical load. Damage to the levator ani muscles follows direct muscle tissue injury or may result from damage to its nerve supply.

13
Mechanism of Levator Ani Damage
Labor and vaginal delivery has the potential to cause this type of damage. However, it is unclear what effect other pathologic conditions, such as chronically increased intra-abdominal pressure, may have on the levator ani muscle.

14
Levels of Vaginal Support
Level I support suspends the upper or proximal vagina. Level II support attaches the mid-vagina along its length to the arcus tendineus fascia pelvis. Level III support results from fusion of the distal vagina to adjacent structures. * Defects in each level of support result in identifiable vaginal wall prolapse: anterior, apical, and posterior.

15
Bulge Symptoms Sensation of vaginal bulging or protrusion
Rectal prolapse Seeing or feeling a vaginal or perineal bulge Vulvar or vaginal cyst/mass Pelvic or vaginal pressure Pelvic mass Heaviness in pelvis or vagina Hernia (inguinal or femoral)
")
16
Urinary symptoms Urinary incontinence
Urethral sphincter incompetence Urinary frequency Detrusor overactivity Urinary urgency Hypoactive detrusor function Weak or prolonged urinary stream Bladder outlet obstruction

17
Urinary symptoms Hesitancy Excessive fluid intake
Feeling of incomplete emptying Interstitial cystitis Manual reduction of prolapse to start or complete voiding Urinary tract infection Position change to start or complete voiding

18
Bowel symptoms Incontinence of flatus or liquid/solid stool
Anal sphincter disruption or neuropathy Feeling of incomplete emptying Diarrheal disorder Hard straining to defecate Rectal prolapse Urgency to defecate Irritable bowel syndrome

19
Bowel symptoms Digital evacuation to complete defecation
Rectal inertia Splinting vagina or perineum to start or complete defecation Pelvic floor dyssynergia Feeling of blockage or obstruction during defecation Hemorrhoids Anorectal neoplasm

20
Sexual symptoms Dyspareunia Vaginal atrophy
Decreased lubrication Levator ani syndrome Decreased sensation Vulvodynia Decreased arousal or orgasm Other female sexual disorder

21
Pain Pain in vagina, bladder, or rectum Interstitial cystitis
Pelvic pain Levator ani syndrome Low back pain Vulvodynia Lumbar disc disease Musculoskeletal pain Other causes of chronic pelvic pain

22
Physical Examination Physical examination begins with a full body systems evaluation to identify pathology outside the pelvis. Systemic conditions such as cardiovascular, pulmonary, renal, or endocrinologic disease may affect treatment choices and should be identified early.

23
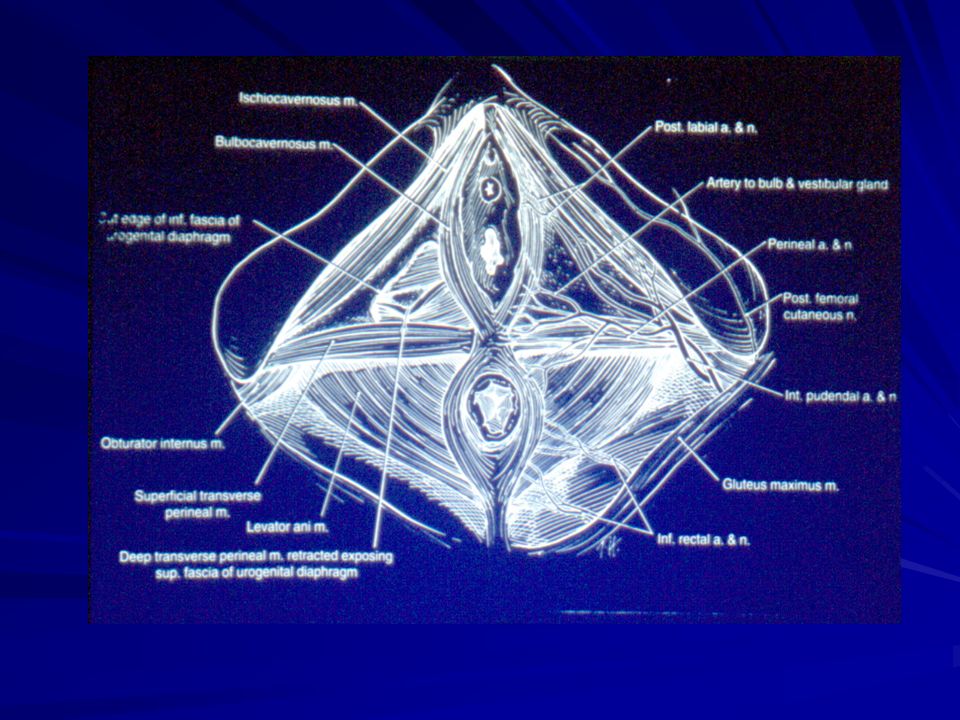
Perineal Examination Lithotomy position. The vulva and perineum are examined for signs of vulvar or vaginal atrophy, lesions, or other abnormalities A neurologic examination of sacral reflexes is performed using a cotton swab (bulbocavernosus reflex , anal wink reflex.

24
Perineal Examination Pelvic organ prolapse examination begins by asking a woman to attempt Valsalva maneuver prior to placing a speculum in the vagina. Importantly, this assessment helps answer three questions: (1) Does the protrusion come beyond the hymen?; (2) What is the presenting part of the prolapse (anterior, posterior, or apical)?; (3) Does the genital hiatus significantly widen with increased intra-abdominal pressure?
 Does the protrusion come beyond the hymen ; (2) What is the presenting part of the prolapse (anterior, posterior, or apical) ; (3) Does the genital hiatus significantly widen with increased intra-abdominal pressure")
25
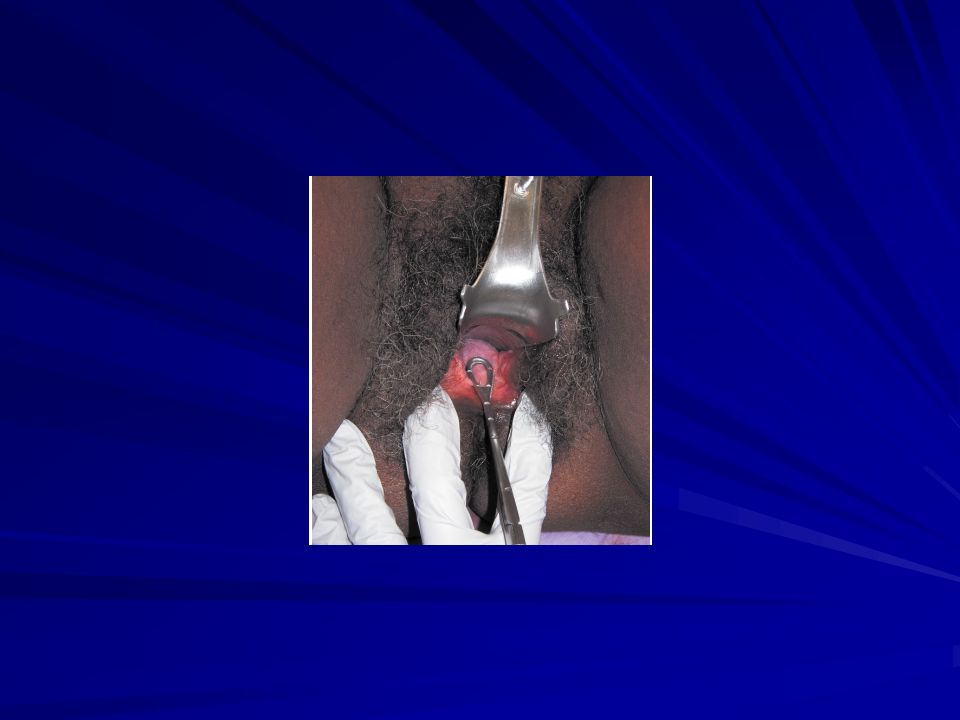
Vaginal Examination If the POP-Q examination is performed, the genital hiatus (gh) and perineal body (pb) are measured during Valsalva maneuver. The total vaginal length (TVL) is then measured by placing the marked ring forceps at the vaginal apex and noting the distance to the hymen.
 is then measured by placing the marked ring forceps at the vaginal apex and noting the distance to the hymen.")
26
Vaginal Examination A bivalve speculum is then inserted to the vaginal apex. It displaces the anterior and posterior vaginal walls C and D are then measured. The speculum is slowly withdrawn to assess descent of the apex. A split speculum is then used to displace the posterior vaginal wall and allow for visualization of the anterior wall and measurement of points Aa and Ba

27
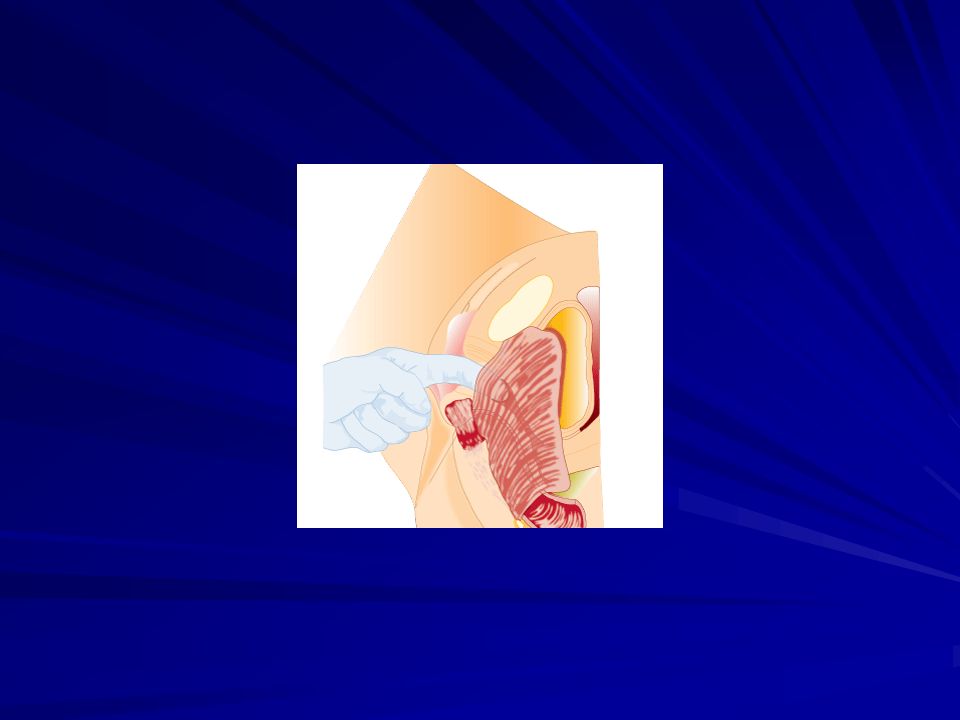
Bimanual examination is performed to identify other pelvic pathology
. During evaluation, an index finger is placed 2 to 3 cm inside the hymen, at 4 and then 8 o'clock. Muscle resting tone and strength is assessed using the 0 through 5 Oxford grading scale. Five represents strong tone and strength (Laycock, 2002). Muscle symmetry is also evaluated. Asymmetric muscles, with palpable defects or scarring, may be associated with a prior obstetric forceps delivery or laceration.
. Muscle symmetry is also evaluated. Asymmetric muscles, with palpable defects or scarring, may be associated with a prior obstetric forceps delivery or laceration.")
35
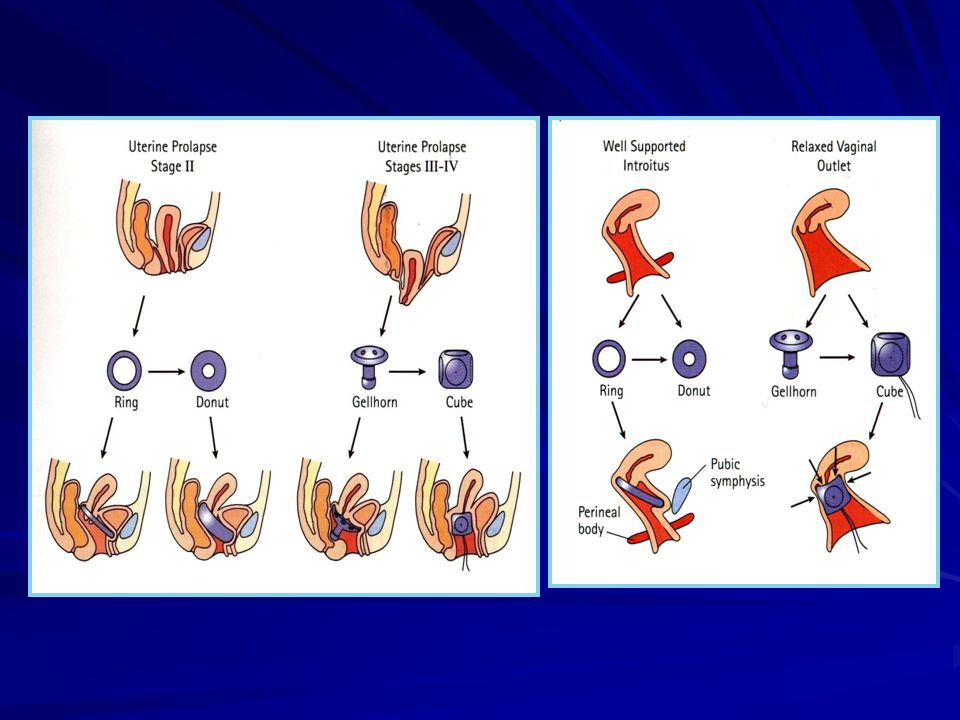
Treatment Nonsurgical Treatment Pessary Use in Pelvic Organ Prolapse
Pelvic Floor Muscle Exercise Pelvic floor muscle exercise has been suggested as a therapy that might limit progression and alleviate prolapse symptoms.

36
Surgical Treatment Obliterative Procedures Reconstructive Procedures

37
Anterior Compartment Anterior colporrhaphy .
. In a randomized trial of three anterior colporrhaphy techniques ( traditional midline plication, ultralateral repair, and traditional plication plus lateral reinforcement with synthetic mesh.

38
Vaginal Apex There is a growing appreciation that support of the vaginal apex provides the cornerstone for a successful prolapse repair. Some experts believe that isolated surgical repair of the anterior and posterior walls is doomed for failure if the apex is not adequately supported (Brubaker, 2005b).
.")
39
Abdominal Sacrocolpopexy
This surgery suspends the vaginal vault to the sacrum using synthetic mesh. Sacrospinous Ligament Fixation (SSLF ) Uterosacral Ligament Vaginal Vault Suspension
 Uterosacral Ligament Vaginal Vault Suspension.")
40
Hysterectomy at the Time of Prolapse Repair
In the United States, hysterectomy is often performed concurrently with prolapse surgery

41
Posterior Compartment
Enterocele Repair Posterior vaginal wall prolapse may be due to enterocele or rectocele. Rectocele Repair Mesh Reinforcement Sacrocolpoperineopexy Perineorrhaphy

48
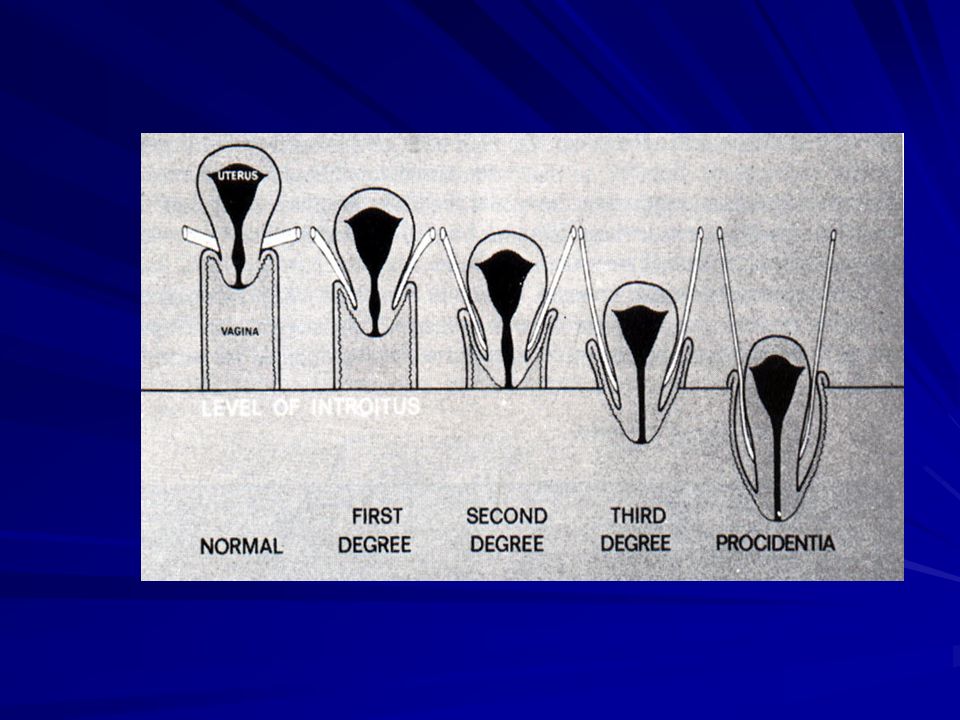
Derajat Prolaps Uteri

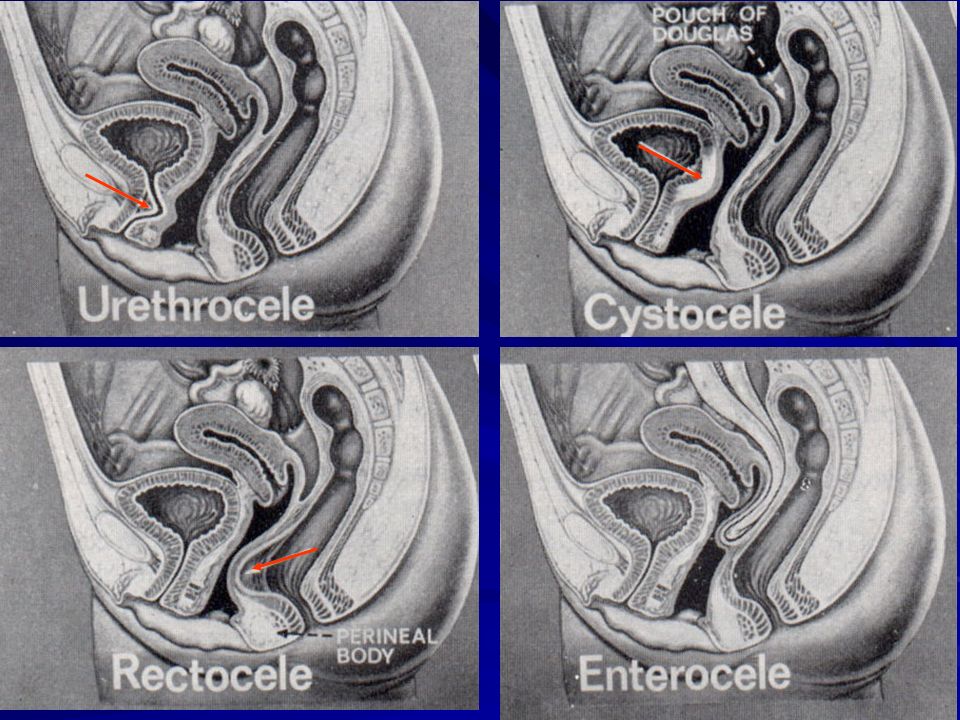
50
Diagram Posisi Normal genitalia dan Eversi komplit dari vagina

51
Diagram defek dinding anterior vagina dan posterior vagina

52
Cara Mudah Patokan Himen Di atas - 1cm Grade I 1 cm sp +1cm Grade II Di bawah + 1cm Grade III Eversi komplit Grade IV

53
PROSEDUR PEMERIKSAAN Hasil tergantung pengetahuan & pengalaman
Abnormal Harus tahu normal Pemeriksaan : Inspeksi, Palpasi, Penilaian Apeks – Perineum Alat : Spekulum Graves Spekulum Sims Sonde

54
PROSEDUR PEMERIKSAAN Posisi : Berdiri Berbaring Posisi berdiri :
Penilaian lebih baik Posisi aktif normal Gejala timbul bila duduk/berdiri Saat Penilaian Istirahat Peregangan : Manuver Valsalva Tarikan dengan Tenakulum

55
PENATALAKSANAAN Pencegahan : Penanganan persalinan yang baik
Terapi hormon pengganti Latihan otot dasar panggul

56
PENATALAKSANAAN Konservatif Penggunaan pesarium vagina
Indikasi penggunaan: Kontra indikasi operasi Menunggu operasi (mengurangi simptom) Masih ingin hamil Trimester pertama kehamilan Pemeriksaan diagnostik memastikan koreksi sistouretrokel besar bukan penyebab stres inkontinensia urin
 Masih ingin hamil. Trimester pertama kehamilan. Pemeriksaan diagnostik memastikan koreksi sistouretrokel besar bukan penyebab stres inkontinensia urin.")
57
Smith (silicone, folding)
Hodge without support (silicone. folding) Hodge with support (silicone, folding) Gehrung with support (silicone, folding) Risser (silicone, folding) Ring with support (slllcone, folding) Ring without support (slllcone, folding) Cube (silicone, flexible) Tandem-Cube (silicone, flexible) Rigid Gellhom (acrylic, multiple drain) 95% Rigid Gellhom (silicone, multiple drain) Flexible Gellhom (silicone, multiple drain) Ring incontinence (silicone) Shaatz (silicone. folding) Incontinence dish (silicone, folding) Inflate Ball (latex) Donut (silicone)
 Hodge with support (silicone, folding) Gehrung with support (silicone, folding) Risser (silicone, folding) Ring with support (slllcone, folding) Ring without support (slllcone, folding) Cube (silicone, flexible) Tandem-Cube (silicone, flexible) Rigid Gellhom (acrylic, multiple drain) 95% Rigid Gellhom (silicone, multiple drain) Flexible Gellhom (silicone, multiple drain) Ring incontinence (silicone) Shaatz (silicone. folding) Incontinence dish (silicone, folding) Inflate Ball (latex) Donut (silicone)")
59
PENATALAKSANAAN Pembedahan Kompartemen Melalaui Vagina
Melalaui Suprapubik Anterior Vagina Anterior repair dgn atau tanpa mesh Kolposuspension Middle Vaginal hysterektomy; vault repair ( fascia); sacrospinous fixation; bilateral iliococcygeal hitch Sacrosphysteropexy ; sacrocolpopexy Posterior Levator plication; fascia repair with or without mesh; transanal repair Mesh interposition; sacrocolpopexy with mesh interposition
; sacrospinous fixation; bilateral iliococcygeal hitch. Sacrosphysteropexy ; sacrocolpopexy. Posterior. Levator plication; fascia repair with or without mesh; transanal repair. Mesh interposition; sacrocolpopexy with mesh interposition.")
60
MASALAH REKURENSI Prolaps puncak vagina akan terjadi bila puncak vagina tidak dijahit pada ligamenta sakro uterina Perbaikan bisa dikerjakan pervaginam atau suprapubik Prosedur sederhana seperti kolpokleisis bisa dikerjakan (khususnya pada wanita yang tidak aktif seksual)
")
61
Fiksasi sakrospinosus dapat dikerjakan dengan menjahit puncak vagina pada ligamentum sakrospinosus tanpa mengurangi kapasitas vagina dengan angka penyembuhan selama 1tahun sebesar 90% Tindakan sakrokolpopeksi melalui abdomen, puncak vagina dijahit dengan proline mesh pada promotorium dengan angka penyembuhan 1-10 tahun sebesar 88-97%

62
KESIMPULAN Mengerti tentang pato anatomi prolaps genitalia akan memberikan hasil yang lebih baik dalam tatalaksana prolapsus genitalia Angka rekurensi sesudah pembedahan vagina perlu mendapat perhatian terutama dalam mengantisipasi berbagai defek yang mungkin terjadi

63
Vagina Normal

65
Perubahan dinding anterior vagina paska persalinan

66
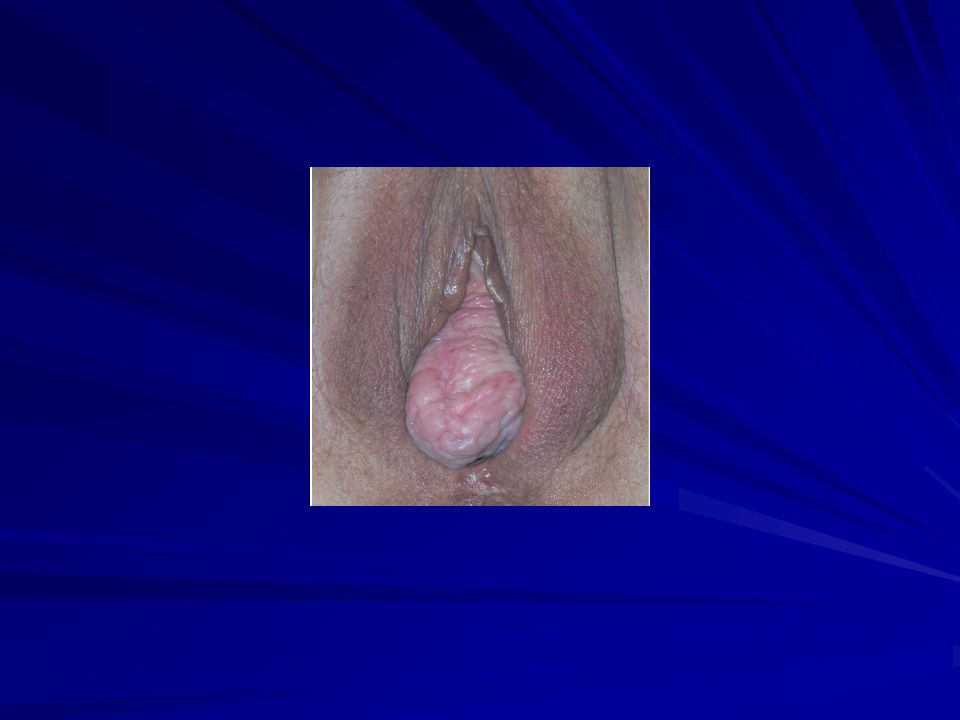
Prolaps Uteri Grade III Dengan Penonjolan Dinding Depan Vagina Yang Dominan

67
Prolaps Uteri Grade IV Dengan Kehilangan Penunjang Dinding Anterior Vagina Komplit

68
Dinding Vagina Posterior Wanita Yang Pernah Melahirkan

69
Rektokel Grade III

70
Rektokel Grade IV

71
Dinding Vagina Posterior Wanita Yang Pernah Melahirkan

72
Prolaps Puncak Vagina

73
Prolaps Genitalia Dan Prolaps Rekti

74
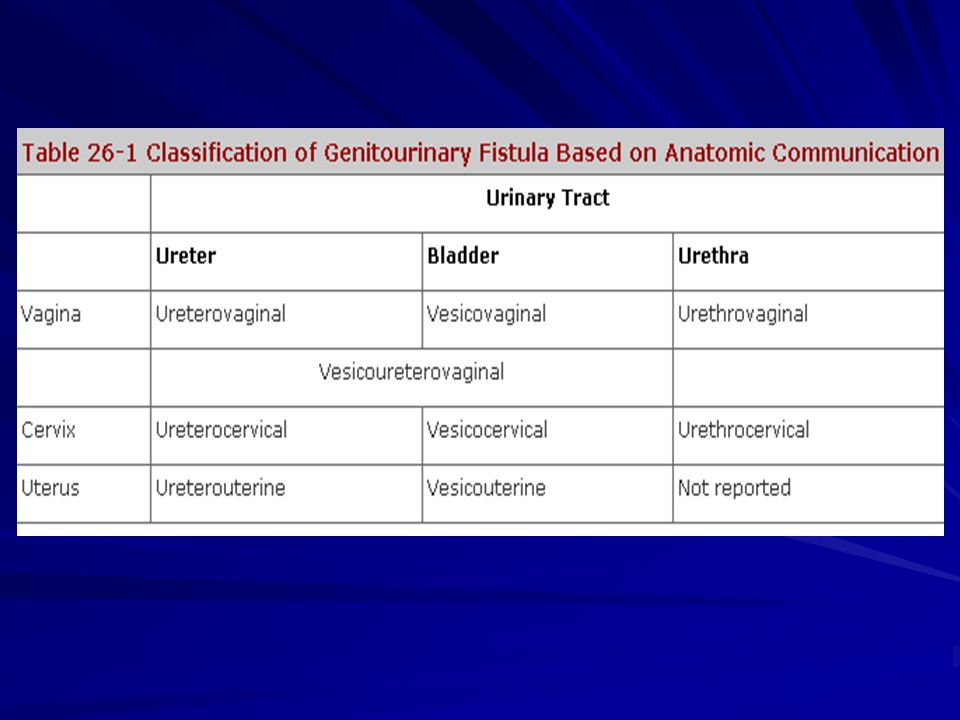
Fistula Urogenital Terdapat hubungan banormal anatara traktus urinarius ( uretra, vesica, ureter dan uterus, cervik vagina

77
Fistula Vesikovaginalis

78
Etiologi Kelainan kongenital
Didapat ( Trauma Obstetri dan Pembedahan Panggul ) Penyebab lain ( Radiasi, keganasan, trauma, benda asing, infeksi )
 Penyebab lain ( Radiasi, keganasan, trauma, benda asing, infeksi )")
79
Diagnosa Anamnesa Pemeriksaan Fisik Metilen Blu test Cystoskopi
Cystouretrogram

81
Penatalaksanaan Konservatif Operatif ( Cure rate dan Timing )
Pervaginam Perabdominam

82
Penutupan perabdominam

83
Thank You

84
Persiapan insersi ring pessarium

85
Caramemegang Ring pesarium
Langkah 2 Jari tangan yang lain membuka labia minora sehingga liang vagina tampak Pessarium dimasukkan kedalam liang vagina sejajar dengan lantai dan didorong sepanjang dinding posterior Caramemegang Ring pesarium

86
Pessarium dimasukkan ke vagina sejajar dinding posterior

87
Pessarium terpasang dalam vagina

88
Memeriksa posisi pessarium

89
Mengait dan memutar pessarium dengan 1 jari

90
Memegang pessarium agar dalam posisi tertekuk

Presentasi serupa


















>")


 (Part 2)>")





