Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
INFECTIONS OF THE CENTRAL NERVOUS SYSTEM
MENINGITIS - BACTERIAL - TUBERCULOSIS - VIRAL - JAMUR ENCEPHALITIS Dr. KIKING RITARWAN, MKT, SpS NEUROLOGY DEPARTMENT OF ADAM MALIK GENERAL HOSPITAL/ UNIVERSITY OF SUMATERA UTARA 2009

2
introductions MENINGITIS
- Inflamations of the meningeal covering of Brain and and spinal cord LEPTOMENINGITIS (arachnoid + pia) PACHYMENINGITIS (Duramater)
 PACHYMENINGITIS. (Duramater)")
3
ACUTE PYOGENIC MENINGITIS =BACTERIAL MENINGITIS
INFLAMATION OF THE LEPTOMENINGES CAUSED BY BACTERIAL INFECTION MANY ORG.CAN PRODUCE PYOGENIC MENINGITIS ex: Escherichia coli (50%), Strep. Pneumoniae (40%), Group B Streptococci (40%), L. monocytogenes (10), etc. It can be categorized into: Spontaneous community acquired meningitis Post traumatic meningitis following neurosur- gery or fx of the skull. c. Device associated meningitis particularly in assoc. With CSF Shunts and drain. Incidence rate are influenced by country, ethnic group, social class and deprivation, and immunization programmes
, Strep. Pneumoniae (40%), Group B Streptococci (40%), L. monocytogenes (10), etc. It can be categorized into: Spontaneous community acquired meningitis. Post traumatic meningitis following neurosur- gery or fx of the skull. c. Device associated meningitis. particularly in assoc. With CSF Shunts and drain. Incidence rate are influenced by country, ethnic group, social class and deprivation, and immunization programmes.")
4
Emperical therapy for suspected bacterial meningitis
AGE Bact. Path Emp. Th. 0-4 weeks E. coli (50%) Amoxycillin + cefo, Group B. Strep (30%) or amoxycillin+ amino- L. monocytogenes (10%) glycoside Klebsiella pneumoniae 4-12 weeks E. coli, Group B Streptocci, Amox + 3rd gen Ceph L. monocytogenes, H. infl (cefotaxime or ceftr) Strep. Pneumoniae, N. meningitidis 3 mo-18 ys H. influenzae, N. meningitidis, 3rd cephaloporin, Strep. Pneumoniae Amox. 18-50ys Strep. Pneumoniae (40%), 3rd cephalosporine, N.meningitidis(30%) Amox >50ys Strep. Pneumo, N.meningitidis, Amox + Aerobic gram (-) bacilii, rd gen cephalosp. L. monocytogenes
 Amoxycillin + cefo, Group B. Strep (30%) or amoxycillin+ amino- L. monocytogenes (10%) glycoside. Klebsiella pneumoniae weeks E. coli, Group B Streptocci, Amox + 3rd gen Ceph. L. monocytogenes, H. infl (cefotaxime or ceftr) Strep. Pneumoniae, N. meningitidis. 3 mo-18 ys H. influenzae, N. meningitidis, 3rd cephaloporin, Strep. Pneumoniae Amox ys Strep. Pneumoniae (40%), 3rd cephalosporine, N.meningitidis(30%) Amox. >50ys Strep. Pneumo, N.meningitidis, Amox + Aerobic gram (-) bacilii, 3rd gen cephalosp. L. monocytogenes.")
5
Clinical picture Bact. Meningitis
The conditions occurs equally in both sexes Children aged 6 month to 1 year are at the greatest risk and children under 15 years of age comprise 75% of all cases. Patients aged 60 and older may be atypical. Symptoms and signs I. early infection: fever, headache, malaise,vomite II. Higher ICP: vomite, headache, seizure, alteration of consciousness, papiledema III. Meningeal irritation: nuchal rigidity, Kernig and Brudzinski + IV. CSF:neutrophilic pleocytosis, low glucose level, elevated protein concentration

6
Neck Stiffness in meningitis

7
Kernig Sign’s

8
DIAGNOSTIC PROSEDURE Lumbal Puncture
Blood should be drawn for blood culture before administration of antibiotic. Bacterial antigen Chest, skull mastoid and paranasal sinus x rays MRI or CT Neuroimaging shoul be performed before LP in the following settings:60 yo or older, Depressed LOC, Focal neurologic signs, papilledema, Patients is immunocompromised.

9
CSF Findings CSF Parameter Bacterial meningitis
WBC Count > 2000/ ul, >60% PMN Glucose < 40 mg/ dl Protein > 200 mg/ dl Gram stain % Culture > 90%

10
Treatment of Bact. Meningitis
1.Antibiotic therapy should be administrated. A minimum of 2 weeks of therapy is recommended. Age Antibiotic 0 – 4 mgg Cefotaxim + Ampi 4-12 mgg Gen III. Cephalos+ Ampi 3 bln- 18 thn Gen III. Ceph + Ampi atau Ampi + chloramph. 18 thn – 50 thn Gen III. Ceph + Ampi 50 thn Gen III. Ceph + ampi. 2. When possible etiologies for meningitis include H. Influenza or S Pneumoniae in child, or S Pneumoniae in adults, give dexamethasone 0,15 mg/kg (IV) every 6 hours for 2-4 days in child and 10 mg IV every 6 hours for 4 days in adults.
 every 6 hours for 2-4 days in child and 10 mg IV every 6 hours for 4 days in adults.")
11
Complication Bacterial meningitis
Cerebral abscess Empyema subdural Convulsie Shock septic Cerebral edema Infarck serebral Herniation

12
Sequele bacterial meningitis
Mental retardation Hydrocephalus Convulsie, psikose Parese, deafness, blind.

13
Tuberculous meningitis
TBM:is an infection of the meninges caused by the acid fast bacillus Mycobacterium tuberculosis The first clinical descrip. Of TBM in 18 century-Sir roberts Whytt, even before Robert Koch (1882) TB haematogenous spread infection to brain parenchyma or meninges In the west country,the first make not much difference again, but lately incident mount drastically in all the world. TBM happened at all of age. Before important HIV factor in prevalens is age
 TB haematogenous spread infection to brain parenchyma or meninges. In the west country,the first make not much difference again, but lately incident mount drastically in all the world. TBM happened at all of age. Before important HIV factor in prevalens is age.")
14
TB in Indonesian occupy 3rd rank from 22 high burden countries
+ 1,7 milyar people ( 1/3 worldwide people) Mycobacterium tuberculosa infected. Reported CDC 2002 was 5,36 cases per people, but worldwide the infection rate is much higher. TB in Indonesian occupy 3rd rank from 22 high burden countries Mycobacterium tuberculosis gol ordo Actinomycetales, famili Mycobacteriaceae, genus Mycobacterium Sifat : aerob, spora (-), motil (-), berkembang biak lambat Mati dgn pemanasan & sinar UV Bakteri batang tahan asam dgn pewarnaan Ziehl–Neelsen /Auramin leading to nickname “ red snapper”.
 Mycobacterium tuberculosa infected. Reported CDC 2002 was 5,36 cases per people, but worldwide the infection rate is much higher. TB in Indonesian occupy 3rd rank from 22 high burden countries. Mycobacterium tuberculosis. gol ordo Actinomycetales, famili. Mycobacteriaceae, genus Mycobacterium. Sifat : aerob, spora (-), motil (-), berkembang biak lambat. Mati dgn pemanasan & sinar UV. Bakteri batang tahan asam dgn pewarnaan Ziehl–Neelsen /Auramin leading to nickname red snapper .")
15
Microscopic Acid fast of M. TB
Meninges tubercle; a central zone of caseation surrounded by epitheloid cells and some giants cells Exudate: composed of fibrin, lymphocytes, plasma cells and other monoclear cells, some PMN leucocytes and areas of caseation necrosis. Arterial become inflamed and occluded, leading to focal brain infarction Acid fast of M. TB

16
RISK FACTORS TBM CLINICAL FEATURES
HIV INF.: 500 TIMES HIGHER INCIDENCE OF TBM IN THE GENERAL POPULATION; HIV INFECTION INCREASES THE LIFETIME RISK OF DEVELOPING TB TO ONE IN THREE ALCOHOL ABUSE, DIABETES MELLITUS MALIGNANCY RECENT CORTICOSTEROID USE POPULATIONS WITH A HIGH PREVALENCE OF PULMONARY TB CLINICAL FEATURES HEADACHE, LETHARGY, CONFUSION, DROWSINESS, FEVER, STIFF NECK, KERNIG AND BRUDZINSKI SIGNS, FOCAL NEUROLOGIC DEFICIT: DUE TO BRAIN INFARCTION CAUSED BY INFECTIOUS ARTERITIS RAISED INTRACRANIAL PRESSURE; DUE TO HYDROCEPHALUS

17
CLINICAL STAGING WITH tbm

18
The course of the illness depends:
- on the extend of meningeal involvement, - the immune response of the host, - the virulence of the organism, - and the stage at which treatment is administered.

19
Ogawa category Definite - bila kultur positi
- otopsi positip, atau keduanya Probable - likuor pleiositosis (>5/mm3), kultur bak- teri dan jamur negatip + salah satu: 1. test tuberkulin positip 2. TB diluar SSP atau TB aktip sebelumnya 3. glukosa likuor < 40 mg/dl 4. protein likuor > 60 mg/dl
, kultur bak- teri dan jamur negatip + salah satu: 1. test tuberkulin positip. 2. TB diluar SSP atau TB aktip sebelumnya. 3. glukosa likuor < 40 mg/dl. 4. protein likuor > 60 mg/dl.")
20
COMPLICATION OF TBM Arteritis thrombosis of a major artery cerebral infarction. Hydrocephalus Seizures Focal motor deficits and impaired cognitive Hypopituitarism in childhood

21
DIFFERENTIAL DIAGNOSIS
Viral encephalitis Partially treated pyogenic meningitis Fungal infection Other inflammatory disorders The presence of active TB elsewhere, and the results of CSF examination are usually sufficient to establish the dx.

22
DIAGNOSTIC PROCEDURE 1. Lumbal Puncture CSF Parameter TB meningitis
WBC Count < 500/ ul, MN Gluco moderate or marked decrease Protein marke increse Gram stain CSF lactic acid > 35 mg/dl.

23
2. Laju endap Darah 3. Radiologic 3a. Chest x ray: detect pulmonary involvement 3b. CT scan8 enhancement of the basal cistern. 3b. MRI are more sensitive than CT sans in detecting basal meningitis infarction owing to arteritis hydrocephalus and parenchymal tuberculomas often in combination in AIDS patient. 4. Arteriografi

24
Images of CT Scans file 1: Contrast- enhanced computed tomography (CT) scan in a patient with tuberculous meningitis demonstrating marked enhancement in the basal cistern and meninges, with dilatation of the ventricles.
 scan in a patient with tuberculous meningitis demonstrating marked enhancement in the basal cistern and meninges, with dilatation of the ventricles.")
25
file 2: Petechial hemorrhages in the subcortical white matter of the brain as a result of tuberculous meningitis– associated vasculitis.

26
file 3: Extensive infarcts of the right basal ganglia and internal capsule after the appearance of vasculitis in the thalamoperforating arteries in a child treated for tuberculous meningitis.

27
Treatment 1. Combination of antituberculous drug
Therapy WHO GILROY ATS - Initial INH+R+PZA+E INH+R+PZA INH+R+PZA atau S atau R+ PZA+S -2MO MO MO - Continued INH+R INH+R INH+R -7 MO MO MO Pyridoxine 50 mg/ hr 2. Spinal arachnoiditis and arteritis may show improvement when terated with corticosteroid. 3. Seizure anticonvulsant 4. ventriculoperitoneal shunt.

28
Prognosis Mortality 10 & 20%
The prognosis is poor in infants, the elderly, when treatment is delayed, and in patients with poor nutrition or debilation from HIV infection or other chronic disease. The outcome is clearly associated with the stage of the disease at dx and the introduction of early treatment. Those who are conscious and without neurological deficits have a good prognosis; those in coma at the beginning of treatment have 20% mortality and only 20 oercent make complete recovery.

29
Viral meningitis Viral meningitis shares clinical features with bacterial meningitis, but patients appear less ill and the disease follows a more benign course. Headache, often meningismus and photophobia, is often the presenting symptoms. The most pathogens include herpes simplex-1 (HSV1), mumps, enterovirus, herpes zoster, adenoviruses and Epstein barr virus.
, mumps, enterovirus, herpes zoster, adenoviruses and Epstein barr virus.")
30
Dx procedure Viral meningitis
Lumbal Puncture Cells Glucose Protein Smear CSF lactic < Normal Mild incr No org < 35 mg/dl MN /mm3 PCR MRI predominant temporal lobe and insular changes in HSE-1 and basal ganglia lesion in japanese encephalitis. TREATMENT: ACICLOVIR 10 mg/ kg iv every 8 hours for days.

31
FUNGAL MENINGITIS ETIOLOGY
Fungi invade of CNS producing meningitis in a small fraction of patients with systemic fungal infection (mycoses) The most pathogens are Cryptococcus neoformans, Coccidiodes immitis, Candida albicans, Aspergillus, H. Capsulatum, Blastomyces, and Mucor Mucormycosis and aspergillosis usually spreads to the CNS from infected sinuses and generally cause local inflamation and necrosis rather than a diffuse meningitis
 The most pathogens are Cryptococcus neoformans, Coccidiodes immitis, Candida albicans, Aspergillus, H. Capsulatum, Blastomyces, and Mucor. Mucormycosis and aspergillosis usually spreads to the CNS from infected sinuses and generally cause local inflamation and necrosis rather than a diffuse meningitis.")
32
Fungi can cause infection in patients with:
1. Cancer 2. Receiving corticosteroids 3. Other immunosuppressive drugs (Diabetes, malignancy, immunosuppressive th., or AIDS) 4. IV drug abuse. Route of entry A. Haematogenous: from the heart, lung, GIT and skin B. Direct: from the orbit and paranasal sinuses.
 4. IV drug abuse. Route of entry. A. Haematogenous: from the heart, lung, GIT and skin. B. Direct: from the orbit and paranasal sinuses.")
33
Clinical Picture Symptoms progress over days, sometimes weeks, with headache, nausea, vomiting and mild encephalopathy. Neurologic examination: 1. meningeal irritation (+) 5, Visual loss 2. papilledema Confusional state 3. Cranial nerve palsies Focal paralysis 4. Ptosis
 5, Visual loss. 2. papilledema 6. Confusional state. 3. Cranial nerve palsies 7. Focal paralysis. 4. Ptosis.")
34
Investigations Lab investigations: 1. Blood culture 2. Serum glucose
3.Arterial blood gases 4. Electrolyte 5. Liver function test 6. Urinalysis CSF Examinations: Imaging

35
Invest….. CSF Exam: - Pressure: Increased
- Appearance: varies with organism - White Blood cells: 50 – (mixed or lymphocytic). - Glucose :Normal - Protein: increased - Cryptoccal antigen is more sensitive - Fungal culture of CSF(+)
. - Glucose :Normal. - Protein: increased. - Cryptoccal antigen is more sensitive. - Fungal culture of CSF(+)")
36
Invest…. Chest X-ray : Hilar lymphadenopathy, cavitation, effusion.
CT or MRI: mass lesion (Cryptococcus)
")
37
Treatment Amphotericin B - Protocol, starting with 1 mg/ day
- doubling the dose daily until reaching 16 mg per day, than increasing at increments of 10 mg until reaching full therapeutic dose of 0,5 to 1,5 mg/ kg per day IV.

38
Dr. Kiking Ritarwan MKT, SpS Email: kritarwan@ yahoo.com
Encephalitis viral Dr. Kiking Ritarwan MKT, SpS yahoo.com

39
ENCEPHALITIS VIRUS Virus Representative virus for Neurologic Disease
DNA - Herpesviruses HSV,VZV,CMV,EBV - Papovavirus PML - Posvirus Vaccinia - Adenovirus Adenovirus serotype RNA - Enterovirus ( Picornavirus) Poliovirus, coxsackivirus, echovirus, enterovirus , Hepatitis A - Togavirus, alphavirus ( arbovirus) Equine encephalitis - Flavivirus (arbovirus) St louis enceph, Japanese and Tic Borne enceph - Orbovirus (Arbovirus) Colorado Tick fever - Bunyavirus (arbovirus) California enceph - Togavirus, rubivirus Rubella - Orthomyxovirus Influenza - Rhabdovirus Rabies - Retrovirus HIV, HTLV
 Poliovirus, coxsackivirus, echovirus, enterovirus , Hepatitis A. - Togavirus, alphavirus ( arbovirus) Equine encephalitis. - Flavivirus (arbovirus) St louis enceph, Japanese and Tic Borne enceph. - Orbovirus (Arbovirus) Colorado Tick fever. - Bunyavirus (arbovirus) California enceph. - Togavirus, rubivirus Rubella. - Orthomyxovirus Influenza. - Rhabdovirus Rabies. - Retrovirus HIV, HTLV.")
40
Saluran pernafasan : parotitis, varicella, morbilli
RUTE INFEKSI: Saluran pernafasan : parotitis, varicella, morbilli Saluran makanan : polio, enterovirus Mukosa kelamin : Herpes simpleks Inokulasi : spt gigitan binatang (rabies a nyamuk) Placenta : CMV + Rubella HIV AND BRAIN (1) Meningitis HIV itself TB Cryptococcal Syphilitic Space occupying lesions Toxoplasmosis Tuberculomas Lymphoma
 Placenta : CMV + Rubella. HIV AND BRAIN (1) Meningitis. HIV itself. TB. Cryptococcal. Syphilitic. Space occupying lesions. Toxoplasmosis. Tuberculomas. Lymphoma.")
41
Strokes and intracerebral haemorrhage HIV AND SPINAL CORD
Encephalitis HIV dementia Progressive multifocal leukoencephalopathy (PML) CMV, HSV, HZV encephalitis Toxoplasmosis Strokes and intracerebral haemorrhage HIV AND SPINAL CORD Vacuolar myelopathy Syphilis HZV, HSV, CMV, HTLV-1 TB Lymphoma HIV AND PNS (1) Radiculopathy CMV Inflammatory demyelinating polyneuropathies Guillain-Barre CIDP
 CMV, HSV, HZV encephalitis. Toxoplasmosis. Strokes and intracerebral haemorrhage. HIV AND SPINAL CORD. Vacuolar myelopathy. Syphilis. HZV, HSV, CMV, HTLV-1. TB. Lymphoma. HIV AND PNS (1) Radiculopathy. CMV. Inflammatory demyelinating polyneuropathies. Guillain-Barre. CIDP.")
42
HIV AND PNS (2) Distal sensory neuropathy Mononeuropathies, mononeuritis multiplex Drugs INH D4T, ddI D4T associated HIV neuromuscular weakness syndrome Diffuse Infiltrative Lymphocytosis Syndrome (DILS) Nutritional neuropathies
 Nutritional neuropathies.")
44
Defenition Viral encephalitis
Is an acute febrile illness with evidence of damage to the parenchymal tissue of the CNS, producing alteration of consciousness, focal neurological signs and seizures. Etiology:viral infection of the nervous system, Herpes simpleks Eastern equine Venezuela St Louis Japanese – B Russian tick-borne Rabies

45
Etiology viral encephalitis
Viral is the most common cause The commonest is HSV type I in adults and type 2 in neonates. It may occur sporadically or in epidemics 50-70% mortality if untreated So establishment of on early specific diagnosis and early initiation of antiviral chemotherapy is of great importance 2/3 of cases involve patients over 40 yo. In Asia, Japenese encephalitis is the commonest cause encephalitis, while measles, rabies and Nipah also occur.

46
PATHOGENESIS THE RARE OCCURANCE OF ENCEPHALITIS AFTER VIRAL INFECTION DEPENS ON THE NATURE AND VIRULENCE OF THE ORGANISM AND THE HOST IMMUNE REPONS. Acces route to brain: - Viruses generally gain access to the CNS by hematogenous or peripheral intraneuronal routes.

47
Access route viral to the brain
Haematogenous herpes simplex sitomegalovirus Epstein-Barr Coxsackie HIV Morbilli Echovirus khoriomeningitis limfositik paravirus Neurogen herpes simplex B-virus Varisela-zoster Rabies.

48
Clinical feature Prodrome fever, malaise, myalgia, irritability, mild upper resp. tract inf., rash or parotitis lasts 4-10 days. Headache Stiff neck (meningismus) Photophobia Disorientation Behavioral disturbances Focal neurologic ex dysphasia and hemiparesis (frontal lobes), epileptic seizure (cerebral cortex), ataxia ( cerebelum) Depressed consciousness Raised ICP.
 Photophobia. Disorientation. Behavioral disturbances. Focal neurologic ex dysphasia and hemiparesis (frontal lobes), epileptic seizure (cerebral cortex), ataxia ( cerebelum) Depressed consciousness. Raised ICP.")
49
Kriteria diagnosis ensefalitis viral
Bentuk asimptomatik analisis LP Bentuk abortif : Nyeri kepala, demam yg tdk tinggi, kaku kuduk. ISPA/ Infeksi GIT Bentuk fulminan: Berlangsung bbrp jam sampai dengan beberapa hari yg berakhir dengan kematian. Bentuk khas ensefalitis: NK, demam, keasadaran menurun, kejang fokal atau umum, hemiparesis, ggn koordinasi, disorientasi, ggn bicara, ggn mental

50
Prosedur diagnostik. LP : CSF jernih, tekanan normal atau meningkat, Pleositosis limfositik < 1000/ul, glukosa dan klorida nornal, protein normal atau sedikit meninggi ( mg/dl MRI atau CT scan SOL (?) EEG Liquor virus DNA dg “polymerase chain reaction” (prosedur cepat, sensitif, akurat) Virus kadang2 dikultur dari liquor,feces,urine nasofaring atau darah. Titer antibodi thd virus tertentu.
 EEG. Liquor virus DNA dg polymerase chain reaction (prosedur cepat, sensitif, akurat) Virus kadang2 dikultur dari liquor,feces,urine nasofaring atau darah. Titer antibodi thd virus tertentu.")
51
Pengobatan. Tidak bisa diidentifikasi dianggap sebagai ensefalitis herpes simpleks dan terapi dgn. Acyclovir atau ganciclovir Jalan nafas diawasi Keseimbangan cairan dan elektrolit dijaga Atasi kejang Atasi peninggian ICP

52
NEUROLOGIC COMPLICATION OF HIV INFECTION

53
INTRODUCTION HIV Neurotropic virus
Can cross BBB at early stage of infection Nervous system is one amongst most targeted by HIV Neurologic manifestation occurr in all HIV stages. These include a wide variety of disorders affecting all parts of the nervous system ( the brain, medula spinalis, meningens, peripheral nerves and muscle). (Ramiandrison et al., 1991).
. (Ramiandrison et al., 1991).")
54
HIV and the brain (1) Meningitis Space occupying lesions HIV itself TB
Cryptococcal Syphilitic Space occupying lesions Toxoplasmosis Tuberculomas Lymphoma

55
HIV and the brain (2) Encephalitis
HIV dementia Progressive multifocal leukoencephalopathy (PML) CMV, HSV, HZV encephalitis Toxoplasmosis Strokes and intracerebral haemorrhage
 CMV, HSV, HZV encephalitis. Toxoplasmosis. Strokes and intracerebral haemorrhage.")
56
HIV and the spinal cord Vacuolar myelopathy Syphilis
HZV, HSV, CMV, HTLV-1 TB Lymphoma

57
HIV and the peripheral nervous system (1)
Radiculopathy TB CMV Inflammatory demyelinating polyneuropathies Guillain-Barre CIDP

58
HIV and the peripheral nervous system (2)
Distal sensory neuropathy Mononeuropathies, mononeuritis multiplex Drugs INH D4T, ddI D4T associated HIV neuromuscular weakness syndrome Diffuse Infiltrative Lymphocytosis Syndrome (DILS) Nutritional neuropathies
 Nutritional neuropathies.")
59
HIV and the muscles HIV myopathy DILS AZT myopathy Pyomyositis

60
MAIN HIV TARGET OF INFECTION

61
Possible mechanisms by which HIV may cross the blood brain barrier (BBB)
As free virus, By passage CD4 + T Lymphocyte cell, By passage within macrophages and Via intermediary endothelial cell infection.

63
TERMINOLOGI toxoplasmosis
Toxoplasmosis penyakit yang disebabkan parasit berupa protozoa obligat intraseluler yang bernama Toxoplasma gondii. Terminologi diambil dari bentuk parasit yang berbentuk cresent shape (bulan sabit) atau toxon yang dalam bahasa Yunani berarti busur/setengah lingkaran. Sedangkan gondii berasal dari kata yang diambil dari sejenis tikus yang hidup di Afrika Utara.
 atau toxon yang dalam bahasa Yunani berarti busur/setengah lingkaran. Sedangkan gondii berasal dari kata yang diambil dari sejenis tikus yang hidup di Afrika Utara.")
64
EPIDEMIOLOGI Transminsi Toxoplasma gondii memakan daging yang kurang matang tertelannya oocyst feses kucing. Susu yang tidak dipasteurisasi dengan baik, terutama susu kambing dan air yang terkontaminasi menyebarluaskan penularan. Di AS rata-rata seropositifnya berkisar 20% - 40% Di Eropa, prevalensi tertinggi dengan seropositif Toxoplasma didapatkan di Prancis sebesar 90% - 95%, Di Belgia, 50% - 80% dari populasi terinfeksi toksoplasma dibandingkan di Inggris sebesar 20% - 40%.

65
ETIOLOGI Toxoplasma gondii parasit coccidian family sarcocystidae
Pertama kali diidentifikasi pada tahun 1908 oleh Nicolle dan Manceaux di Afrika Utara & oleh Spledore di Brazil. Berukuran kecil (sekitar 2 x 3 m), bentuk oval, pyriformis, bundar atau massa protoplasmic memanjang dengan nukleus sentral. Parasit ini hidup dalam beberapa bentuk yang berbeda : Tachyzoite atau endozoite, dulunya disebut sebagai trophozoite. Tissue cyst (mengandung bradyzoites) Oocyst mengandung sporozoites yang menular
, bentuk oval, pyriformis, bundar atau massa protoplasmic memanjang dengan nukleus sentral. Parasit ini hidup dalam beberapa bentuk yang berbeda : Tachyzoite atau endozoite, dulunya disebut sebagai trophozoite. Tissue cyst (mengandung bradyzoites) Oocyst mengandung sporozoites yang menular.")
66
PENULARAN Gambar 1. Siklus Hidup Toxoplasma gondii

67
GAMBARAN KLINIS Infeksi primer T.Gondii pasien imunokompeten asimptomatik atau sub klinis. Manifestasi klinis paling sering kelelahan, terasa dingin, nyeri kepala dan limfadenopati umum. Beberapa pasien disertai dengan demam rendah. Jarang Toxoplasmosis menimbulkan keparahan atau infeksi yang fatal pada pasien dengan imunokompeten. Bila SSP terlibat drowsiness, confusion, iritabilitas berlanjut sampai koma dan kejang juga pernah dilaporkan. Pemeriksaan fisik hiperrefleksi dan disertai tanda keterlibatan upper motor neuron.

68
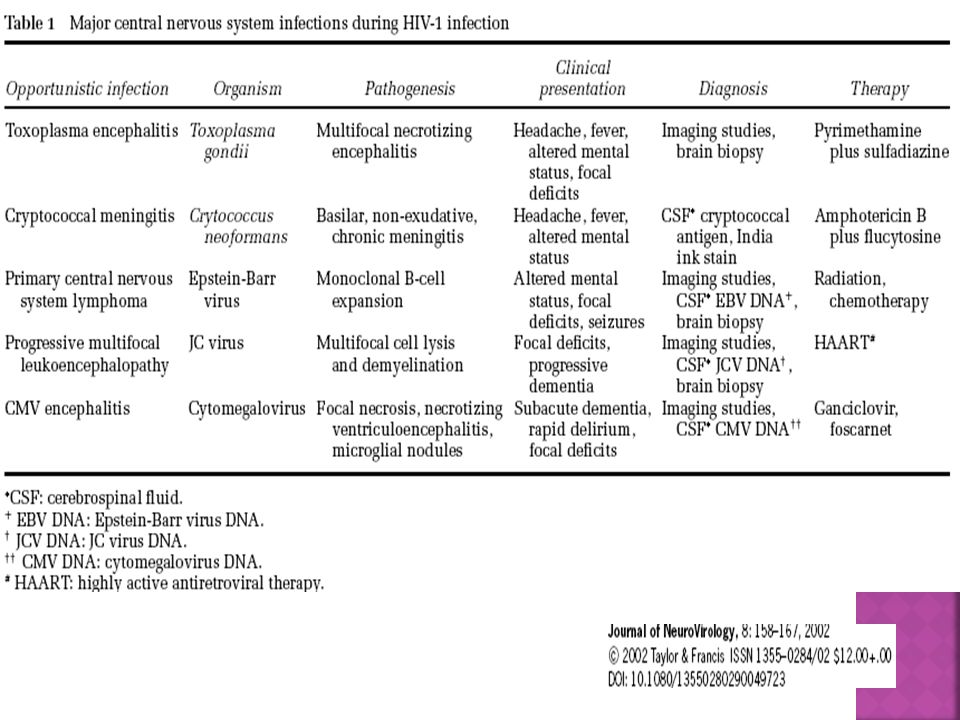
TOXOPLASMOSIS IN HIV INFECTION
SYMTOMS / SIGNS RANGE % Focal neurological abnormality 49 – 95 Fever 41 – 74 Headache 49 – 73 Confusion 15 – 58 Seizure 15 – 40

69
PROSEDUR DIAGNOSTIK Identifikasi dan Isolasi Parasit Test Serologis
TSP Dye Test Tes Differential Agglutination Avidity Antibodi IgM, IgG, IgA, dan IgE Neuroimaging Biopsi Otak

70
TOXOPLASMOSIS IN HIV INFECTION
Laboratory finding : CSF non specific CT scan positive in >90% - enhancing ring lesions - basal ganglia / cortico- Medullary junction - multiple lesion MRI more sensitive in detecting lesion Serology, if negative help to exclude the diagnosis Brain biopsy if in doubt

71
Dx Cerebral Toxoplasmosis
Headache or focal symptoms/signs + focal enhancing lesion(s) on CT brain scan + response to antitoxoplasmosis therapy after 2 weeks (APNAC Study)
 on CT brain scan + response to antitoxoplasmosis therapy after 2 weeks. (APNAC Study)")
72
Pemeliharaan/rumatan
PENATALAKSANAAN Fase akut (3-6 minggu) Pemeliharaan/rumatan Pilihan pertama Pilihan kedua Pilihan ketiga Pyrimethamine oral 200 mg hari pertama, selanjutnya mg/hr + leucovorin oral mg/hr + sulfadiazine oral mg/hr Pyrimethamine + leucovorin (dosis di atas) + clindamycin oral atau IV 4 x 600 mg Pyrimethamine + leucovorin (dosis di atas) + salah satu : Atovaquone oral 2 x 1500 mg Azithromycin oral 1 x 900 – 1200 mg Clarithromycin oral 2 x 500 mg Dapson oral 1 x 100 mg Minocyclin oral 2 x mg Pyrimethamine oral mg/hr + leucovorin oral mg/hr + sulfadiazine oral mg/hr. Pyrimethamine + leucovorin (dosis di atas) + clindamycin oral 4 x 300 mg – 450 mg Pyrimethamine + leucovorin (dosis di atas) + salah satu antibiotika tersebut dosis sama.
 Pemeliharaan/rumatan. Pilihan pertama. Pilihan kedua. Pilihan ketiga. Pyrimethamine oral 200 mg hari pertama, selanjutnya mg/hr + leucovorin oral mg/hr + sulfadiazine oral mg/hr. Pyrimethamine + leucovorin (dosis di atas) + clindamycin oral atau IV 4 x 600 mg. Pyrimethamine + leucovorin (dosis di atas) + salah satu : Atovaquone oral 2 x 1500 mg. Azithromycin oral 1 x 900 – 1200 mg. Clarithromycin oral 2 x 500 mg. Dapson oral 1 x 100 mg. Minocyclin oral 2 x mg. Pyrimethamine oral mg/hr + leucovorin oral mg/hr + sulfadiazine oral mg/hr. Pyrimethamine + leucovorin (dosis di atas) + clindamycin oral 4 x 300 mg – 450 mg. Pyrimethamine + leucovorin (dosis di atas) + salah satu antibiotika tersebut dosis sama.")
73
PROGNOSIS Prognosis Toxoplasmosis pada orang dewasa baik selama sistem imunnya baik. Toxoplasmosis akut penderita yang immunocompromised terutama dengan keterlibatan SSP dapat menyebabkan kejadian fatal

74
PENCEGAHAN Pencegahan infeksi yang dapat dilakukan adalah :
Memakan daging yang sudah dimasak hingga matang, atau yang telah dibekukan hingga -20°C. Membersihkan dan mengurangi kepadatan populasi kucing. Konsisten untuk selalu mencuci tangan setelah memegang kucing dan kotoran kucing. Wanita hamil dan penderita immunocompromized dihindarkan kontak dengan kucing dan hanya memakan daging yang dimasak matang. Buah-buahan dan sayur-sayuran harus dicuci dahulu sebelum dikonsumsi dan menggunakan sarung tangan bila hendak berkebun.

76
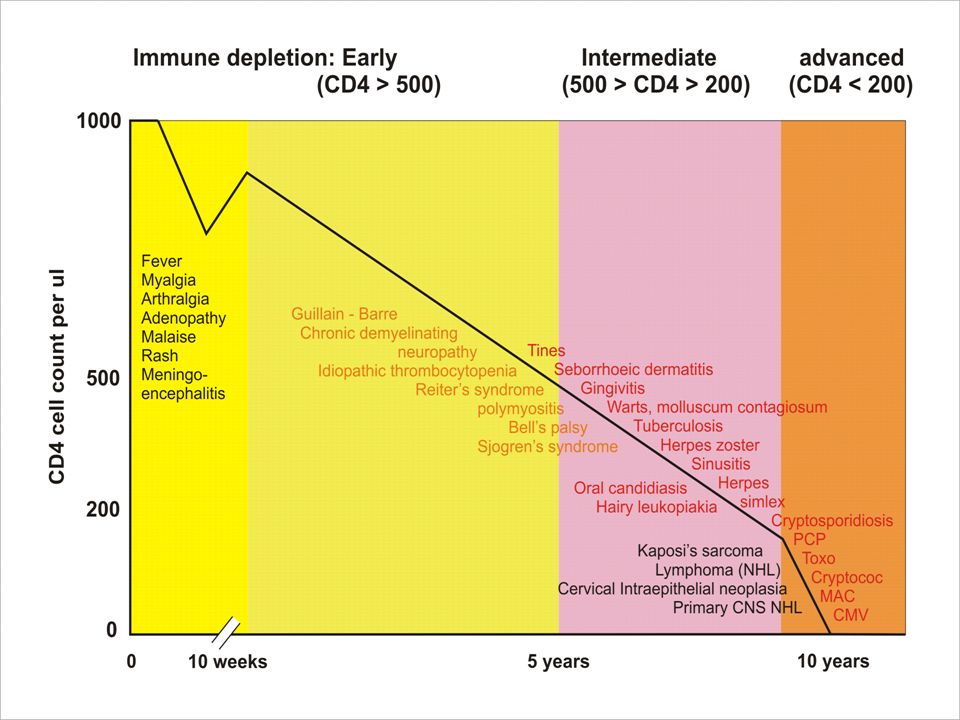
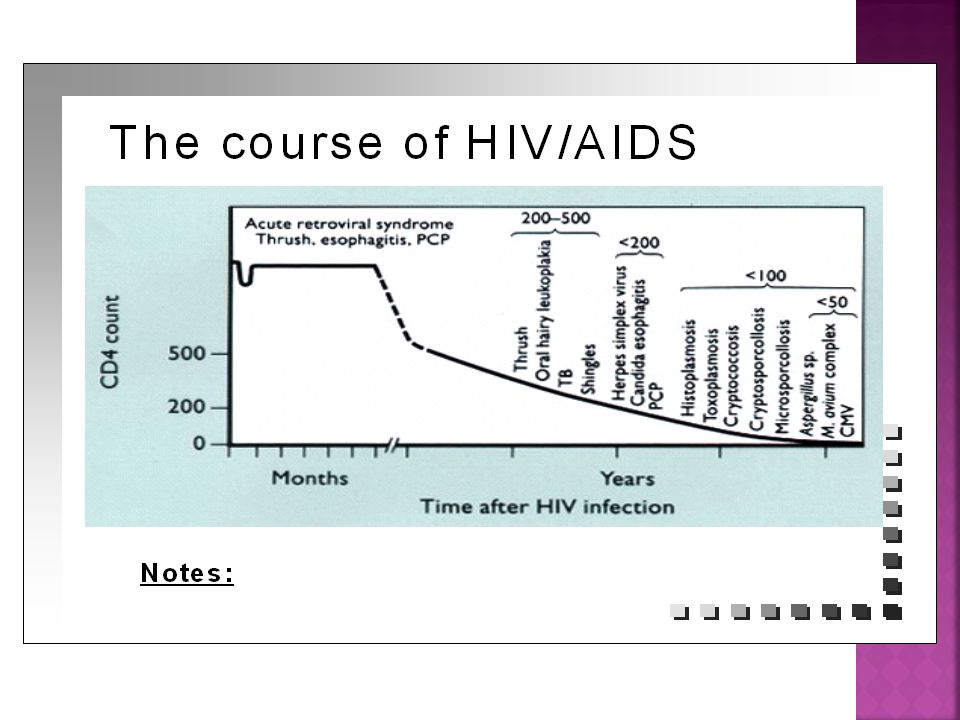
HUBUNGAN CD4 DENGAN INFEKSI OPPORTUNISTIK
STADIUM HIV Jumlah CD4 Gejala Neurologi Stadium Awal > 500 sel / mm3 Aseptic meningitis Ensefalitis GBS Cranial nerve palsy Herpes zoster Stadium Pertengahan 200 – 500 sel / mm3 Gangguan kognitif Distal sensory polyneuropathy Myelopathy Myopathy Stadium Lanjut < 200 sel / mm3 HIV ensefalopati CNS Toxoplasmosis Infeksi CMV Limfoma PML

77
Myelitis Inflamation of the spinal cord
I. Transverse Myelitis, II. Disseminata, III. Difussa Transverse myelitis (MYELOPATHY) is a syndrome characterized by acute spinal cord dysfunction both halves the cord in transverse section.
 is a syndrome characterized by acute spinal cord dysfunction both halves the cord in transverse section.")
78
MYELITIS CLASSIFICATION OF INFLAMMATORY DISEASE
Gray matter…… Poliomyelitis. White matter …. Leukomyelitis. The whole crossectional are…Tranversemyelitis. Lesions are multiple and wide spreadOver a long vertical extent….. DiffuseOr Disseminated. Combined meninges and spinal cord…Meningomyelitis. Combined meninges and root--- meningpradiculitis. Inflammatory disease limited to the spinal dura…. Pachymeningitis. Infected material collects in the epidural or subdural space… Epidural spinal Or subdural spinal abcess or Granulomatous. CLASSIFICATION OF INFLAMMATORY DISEASE OF THE SPINAL CORD … SEE TRANSPARANTS

79
ACUTE TRANSVERSE MYELITIS
IS USUALLY BILATERAL AND TENDS TO CAUSE MORE SEVERE WEAKNESS THAN THE TYPICAL ATTACKS OF PARTIAL MYELITIS. The condition may be peri infectious or postinfectious process and has been associated with many viral infection, including poliovirus, echovirus and coxsackieviruses.

80
Etiologie Transverse myelitis
1. Congenital – vascular malformation 2. Infectious – viral infection 3. Autoimune- peri or post infection or vaccinial myelitis. 4. Multiple sclerosis 5. Neoplastic 6. Toxic- secondary to heroin injection 7. Vascular 8. Degenerative- irradiation 9. Idiopathic.

81
Clinical manifestation
Acute paraplegic or Quadriplegic. Urinary retention. Sensory disturbances

82
Diagnostic prosedure CSF examination:
- mild to moderate lymphocytic pleocytosis ( cell/mm3), elevated protein ( mg/dl), and normal or mildly depressed glucose level. PCR- virus spesific PCR and antibody titer should be performed. MRI-T2 weighted shows increased signal intensity involving gray matter and surronding white matter.
, elevated protein ( mg/dl), and normal or mildly depressed glucose level. PCR- virus spesific PCR and antibody titer should be performed. MRI-T2 weighted shows increased signal intensity involving gray matter and surronding white matter.")
83
PROSEDUR DIAGNOSTIK Dikutip dari : Transverse Myelitis Consortium Working Group. Proposed diagnostic criteria and nosology of acute transverse myelitis. Neurology 2002 ; 59 :

84
Treatment Viral myelitis
Antiviral treatment: Glucocorticoid Spasticity: baclofen (lioresal) 10 mg q6h, benzodiazepin and tizanidine.
 10 mg q6h, benzodiazepin and tizanidine.")
Presentasi serupa
. The genome is surrounded by a large number of proteins (coat.>")

















 MAIDI SAMEKTO>")
