Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
EVOLUSI TEKNIK HEMODIALISIS FOKUS PADA HEMODIAFILTRASI
Afiatin Divisi Ginjal Hipertensi Departemen IP Dalam FK Unpad- RS. Hasan Sadikin Bandung

2
CURICULUM VITAE Afiatin SpPD KGH
Anggota PAPDI, PERNEFRI, INASH, ISN, ISPD and ISHD Staf Divisi Ginjal Hipertensi Dept IP Dalam FK Unpad-RSHS Penanggung Jawab Unit HD : RSHS, Klinik Perisai Husada dan RS. Santosa Bandung Supervisor Penjamin Mutu Unit HD : beberapa RS di Jawa Barat

3
Diffusion for for small molecules >large molecules

4
Diffusion

5
Filtration of water with small and medium sized molecules

6
Convection

7
To remove the solutes HD Low Flux HD High Flux HDF HFR Diffusion
Convection Adsorbimento su membrana Middle molecular weight toxins Low molecular weight toxins

8
Molecular bond of a substance
on the surface or inner structure of a membrane

9
Adekuasi 2000 – masa datang Adequacy of Dialysis Kontrol Harga
Klirens online HD dengan monitoring secara komputerisasi Pembuangan Toksin Middle Molecule Hemo-diafiltrasi dan Filtrasi Internal Menurunkan Inflamasi Biocompatibilitas yang lebih baik Dan Ultrapure dialysate Adequacy of Dialysis Dialisis satiap hari dan atau malam hari (nocturnal) untuk mengontrol TD dan Ca x P Monitor volume darah untuk ultrafiltrasi yang lebih aman OUTCOME: Kualitas hidup Rehabilitasi Morbiditas & Mortalitas Kontrol Harga
 untuk mengontrol. TD dan Ca x P. Monitor volume darah untuk ultrafiltrasi yang lebih aman. OUTCOME: Kualitas hidup. Rehabilitasi. Morbiditas & Mortalitas. Kontrol Harga.")
10
TOKSIN UREMIK DAN DAMPAK PADA VASKULAR
10

11
SOLUT BERAT MOLEKUL RENDAH
LARUT DALAM AIR Conventional Hemodialysis Table 1. Free water-soluble low-molecular-weight solutes (N 45) Abbreviations are: CN, normal concentration; CU, mean/median uremic concentration; CMAX, maximal uremic concentration; MW, molecular weight; ref, reference; ADMA, asymmetrical dimethylarginine; SDMA, symmetrical dimethylarginine. The underlined numbers behind the slash point to the number of data on which the means or medians have been obtained. No underlined number indicates that no data about the number of samples were available. Normal values are reported as meansSD, or in the case of a single value as a maximum (accompanied by ); uremic values are reported as meansSD or, in the case of a single value, as a median. aCMAX values are original data (all other values were calculated as mean 2 SD based on CU) Review on uremic toxins: Classification, concentration, and interindividual variability RAYMOND VANHOLDER, RITA DE SMET, GRIET GLORIEUX, ANGEL ARGILE´ S, ULRICH BAURMEISTER, PHILIPPE BRUNET, WILLIAM CLARK, GERALD COHEN, PETER PAUL DE DEYN, REINHOLD DEPPISCH, BEATRICE DESCAMPS-LATSCHA, THOMAS HENLE, ACHIM JO RRES, HORST DIETER LEMKE, ZIAD A. MASSY, JUTTA PASSLICK-DEETJEN, MARIANO RODRIGUEZ, BERND STEGMAYR, PETER STENVINKEL, CIRO TETTA, CHRISTOPH WANNER, and WALTER ZIDEK, For the EUROPEAN UREMIC TOXIN WORK GROUP (EUTOX) Kidney International, Vol. 63 (2003), pp. 1934–1943
 Abbreviations are: CN, normal concentration; CU, mean/median uremic concentration; CMAX, maximal uremic concentration; MW, molecular weight; ref, reference; ADMA, asymmetrical dimethylarginine; SDMA, symmetrical dimethylarginine. The underlined numbers behind the slash point to the number of data on which the. means or medians have been obtained. No underlined number indicates that no data about the number of samples were available. Normal values are reported as. meansSD, or in the case of a single value as a maximum (accompanied by ); uremic values are reported as meansSD or, in the case of a single value, as a. median. aCMAX values are original data (all other values were calculated as mean 2 SD based on CU) Review on uremic toxins: Classification, concentration, and. interindividual variability. RAYMOND VANHOLDER, RITA DE SMET, GRIET GLORIEUX, ANGEL ARGILE´ S, ULRICH BAURMEISTER, PHILIPPE BRUNET, WILLIAM CLARK, GERALD COHEN, PETER PAUL DE DEYN, REINHOLD DEPPISCH, BEATRICE DESCAMPS-LATSCHA, THOMAS HENLE, ACHIM JO RRES, HORST DIETER LEMKE, ZIAD A. MASSY, JUTTA PASSLICK-DEETJEN, MARIANO RODRIGUEZ, BERND STEGMAYR, PETER STENVINKEL, CIRO TETTA, CHRISTOPH WANNER, and WALTER ZIDEK, For the EUROPEAN UREMIC TOXIN WORK GROUP (EUTOX) Kidney International, Vol. 63 (2003), pp. 1934–1943.")
12
SOLUT BERAT MOLEKUL SEDANG
Convective HD Table 3. Middle molecules (N 22) Abbreviations are: CN, normal concentration; CU, mean/median uremic concentration; CMAX, maximal uremic concentration; MW, molecular weight; ref, reference. The underlined numbers behind the slash point to the number of data on which the means or medians have been obtained. No underlined number indicates that no data about the number of samples were available. No number indicates that no n value was given. Normal values are reported as mean SD, or in the case of a single value as a maximum (accompanied by ); uremic values are reported as mean SD or, in the case of a single value, as a median. aCMAX values are original data (all other values were calculated as mean 2 SD based on CU) b S Schmaldienst, Vienna: personal communication c Degranulation inhibiting protein I corresponds to angiogenin
 Abbreviations are: CN, normal concentration; CU, mean/median uremic concentration; CMAX, maximal uremic concentration; MW, molecular weight; ref, reference. The underlined numbers behind the slash point to the number of data on which the means or medians have been obtained. No underlined number indicates that. no data about the number of samples were available. No number indicates that no n value was given. Normal values are reported as mean SD, or in the case of. a single value as a maximum (accompanied by ); uremic values are reported as mean SD or, in the case of a single value, as a median. aCMAX values are original data (all other values were calculated as mean 2 SD based on CU) b S Schmaldienst, Vienna: personal communication. c Degranulation inhibiting protein I corresponds to angiogenin.")
13
Definisi Hemodiafiltrasi
HDF suatu RRT ekstrakorporeal dengan prinsip kombinasi difusi dan konveksi untuk meningkatkan pembuangan solut dengan berat molekul beragam. Ultrafiltrasi akan berlebih sehingga diperlkan cairan substitusi untuk mempertahankan target balans cairan. Membran yang dipakai : permeabilitas tinggi

14
Hemodiafiltration to waste Blood In Blood Out (from patient)
Replacement Solution Dialysate Blood In Blood Out to waste (from patient) (to patient) HIGH PRESS LOW PRESS HIGH CONC LOW CONC Describe flow paths on slide. Note: Point out again that … Replacement fluids may be administered either pre or post filter. We will discuss these options later in the program. 14
 (to patient) HIGH PRESS. LOW PRESS. HIGH CONC. LOW CONC. Describe flow paths on slide. Note: Point out again that … Replacement fluids may be administered either pre or post filter. We will discuss these options later in the program. 14.")
15
Sirkuit ekstrakorporeal dengan biocompatibilitas tinggi
HDF Kombinasi ultrafiltrasi dan difusiion Modalitas dialisis efektifAn effective dialysis modality Memperluas spektrum toksin uremik yang terbuang sampai berat molekul sedang sd berat Cairan dialisat ultrapure Cairan substitusi steril Membran : High-flux dan sintetik Sirkuit ekstrakorporeal dengan biocompatibilitas tinggi

17
PILIHAN UNTUK REINFUSION
PRE-DILUTION POST-DILUTION MIXED MID-DILUTION INFUSION PRE INFUSION PRE < Hemoconcentration < TMP < Depurative efficiency < Hemoconcentration < TMP < Depurative efficiency INFUSION POST INFUSION POST

18
Predilution On-Line HDF
Filtrate (UF + HDF ) blood (in) blood pump Substituate (pre) HDF pump blood (out) Permeabilitas membran meningkat - filtrasi dari darah yang terdilusi - Kecepatan infus lebih tinggi konveksi lebih baik klirens solut BM sedang meningkat tetapi … Dilusi akan menurunkan efisiensi : gradien konsentrasi akan menurun sehingga difusi menurun menurunkan klirens solut dengan BM rendah Cairan substitusi masuk ke dalam sirkuit sebelum dializer dialyzer 18
 blood (in) blood pump. Substituate. (pre) HDF pump. blood (out) Permeabilitas membran meningkat - filtrasi dari darah yang terdilusi. - Kecepatan infus lebih tinggi. konveksi lebih baik. klirens solut BM sedang meningkat. tetapi … Dilusi akan menurunkan efisiensi : gradien konsentrasi akan menurun sehingga difusi menurun. menurunkan klirens solut dengan BM rendah. Cairan substitusi masuk ke dalam sirkuit sebelum dializer dialyzer. 18.")
19
Postdilution On-Line HDF
Pembuangan solut BM rendah paling baik dengan teknik ini, – filtrasi dari darah yang belum terdilusi Tetapi … ultrafiltrasi terbatas karena hemokonsentrasi viskositas darah yang tinggi terbentuknya lapisan protein sekunder polarisasi membran Dan membutuhkan QB yang tinggi blood (out) Substituate (post) HDF pump Filtrate (UF + HDF) blood pump blood (in) Cairan substitusi masuk ke dalam sirkuit setelah dializer 19
 Substituate (post) HDF pump. Filtrate. (UF + HDF) blood pump. blood (in) Cairan substitusi masuk ke dalam sirkuit setelah dializer. 19.")
20
Meningkatkan permeabilitas dializer terhadap air dan solut krn…
Dilusi diatur secara individual dan memperbaiki rheologi darah Kecepatan filtrasi tinggi → memperbaiki proses konveksi → meningkatkan pembuangan solut Aman dari kehilangan albumin yang terjadi pada TMP tinggi Best of both worlds! Mid-dilution HDF feedback control Filtrate (UF + HDF) blood (in) blood pump Substituate (pre) HDF pump 1 blood (out) Substituate (post) HDF pump 2 Cairan substitusi masuk ke sirkuit secara bersamaan (simultan) sebelum dan sesudah dializer dan diatur oleh sistem ( feedback system) 20
 blood (in) blood pump. Substituate. (pre) HDF pump 1. blood (out) Substituate (post) HDF pump 2. Cairan substitusi masuk ke sirkuit secara bersamaan (simultan) sebelum dan sesudah dializer dan diatur oleh sistem ( feedback system) 20.")
21
Olpur Mid-Dilution HDF Filter

23
Indikasi HDF Pasien PGK yang tidak stabil :
Penyakit kardiovaskular berat Hipotensi kronik Diabetes Usia tua Pasien dengan kenaikan BB interdialitik yang tidak terkontrol Pasien PGK dengan kebutuhan dosis dialisis yang tinggi dan mencakup pengeluaran toksin dengan semua jenis BM Pasien Gangguan Ginjal Akut yang kritis unstable CKD patients presenting with severe cardiovascular risk factors, chronic hypotension, diabetics, elderly and uncompliant patients with large interdialytic fl uid gain; second, junior and senior CKD patients requiring a large dialysis dose covering the whole spectrum of uremic toxins or being exposed to prolonged periods of renal replacement therapy. Selection of CKD patients may be justifi ed by the better vascular stability and by the improved biocompatibility provided by the method. Hemodiafilter A high-fl ux, high-effi ciency dialyzer is required. The membrane should have a high hydraulic permeability (ultrafi ltration coeffi cient KUF 50 ml/h/mm Hg), high solute permeability (mass transfer-area coeffi cient KoA urea 600 and 2-microglobulin 60 ml/min) and large surface of exchange (1.50–2.10 m2). Prescription and Substitution Fluid Volume per Session The conventional ol-HDF treatment schedule is based on 3 dialysis sessions per week of 4 h (12 h/week). In this relatively short treatment time, it is of paramount importance to ensure high blood fl ows (400 ml/min) coupled with high dialysate and/or infusate fl ow rates in order to optimize solute exchange. By increasing the frequency and/or duration of HDF sessions, it is also possible to achieve a more physiological and more effective treatment. Follow-Up and Monitoring of Patients Treated with Online Hemodiafiltration Follow-up and monitoring of ol-HDF-treated patients are strictly equivalent to those of patients treated with regular conventional hemodialysis. Dialysis adequacy targets as recommended by the Kidney Disease Outcome Quality Initiative and the European Best Practice Guidelines should be equivalent in terms of extracellular fl uid volume control, blood pressure control, minimum dialysis dose delivered (urea Kt/Vdp 1.2), uremia control, acidosis and hyperkaliemia correction, phosphorus, calcium and parathyroid hormone control, and anemia correction. On a regular basis, ol-HDF provides a higher solute removal rate as compared to conventional low- and high-fl ux hemodialysis for low- and middle-size uremic toxins including the 2-microglobulin. On a long-term basis, this higher effi cacy translates in a reduction of the time-averaged concentration of blood 2-microglobulin concentrations meaning that this middle-size marker should be routinely incorporated in the criteria of dialysis adequacy. Due to the high volume of fl uid exchanged per session (25–50 l/session) it is also recommended to follow on a monthly basis the infl ammatory profi le of ol-HDF-treated patients (e.g. high-sensitivity C-reactive protein) and the nutritional markers (albumin and transthyretin).
, high solute permeability (mass transfer-area coeffi cient KoA urea 600 and. 2-microglobulin 60 ml/min) and large surface of exchange (1.50–2.10 m2). Prescription and Substitution Fluid Volume per Session. The conventional ol-HDF treatment schedule is based on 3 dialysis sessions. per week of 4 h (12 h/week). In this relatively short treatment time, it is. of paramount importance to ensure high blood fl ows (400 ml/min) coupled. with high dialysate and/or infusate fl ow rates in order to optimize solute. exchange. By increasing the frequency and/or duration of HDF sessions, it is also. possible to achieve a more physiological and more effective treatment. Follow-Up and Monitoring of Patients Treated with Online. Hemodiafiltration. Follow-up and monitoring of ol-HDF-treated patients are strictly equivalent. to those of patients treated with regular conventional hemodialysis. Dialysis. adequacy targets as recommended by the Kidney Disease Outcome Quality. Initiative and the European Best Practice Guidelines should be equivalent in. terms of extracellular fl uid volume control, blood pressure control, minimum. dialysis dose delivered (urea Kt/Vdp 1.2), uremia control, acidosis and hyperkaliemia. correction, phosphorus, calcium and parathyroid hormone control, and anemia correction. On a regular basis, ol-HDF provides a higher solute removal rate as compared. to conventional low- and high-fl ux hemodialysis for low- and middle-size. uremic toxins including the 2-microglobulin. On a long-term basis, this higher. effi cacy translates in a reduction of the time-averaged concentration of blood. 2-microglobulin concentrations meaning that this middle-size marker should. be routinely incorporated in the criteria of dialysis adequacy. Due to the high volume of fl uid exchanged per session (25–50 l/session) it. is also recommended to follow on a monthly basis the infl ammatory profi le of. ol-HDF-treated patients (e.g. high-sensitivity C-reactive protein) and the nutritional. markers (albumin and transthyretin).")
24
KEUNTUNGAN KLINIS HDF Klirens dialisis tercapai dengan mudah
Menurunkan risiko β2-microglobulin amyloidosis Menurunkan kadar toksin dengan BM sedang Memperbaiki toleransi kardiovaskular Menunjang keberhasilan terapi anemia Penurunan harga cairan substitusi dengan persediaan secara online (seperti dialisat) Keberhasilan : mortalitas dan morbiditas
 Keberhasilan : mortalitas dan morbiditas.")
26
2 microglobulin and risk of death
Relative Risk of Death <27.5 >50 [2M]2 mg/l Cheung AK et al NEMO Study JASN(ePub 2005)
")
27
Middle molecules removal in HDF versus LF-HD and HF-HD
P>0.01 P>0.01 P>0.01 Urea 60d Creat 113d Osteoc 5.8kd β2M 11.8kd Myogl 16kd

28
Bonforte G et al. Blood Purif, 2002

29
Risiko relatif mortalitas pada tipe dialisis
Mortality risk for patients receiving hemodiafiltration versus hemodialysis: European results from the DOPPS B Canaud1, JL Bragg-Gresham2, MR Marshall3, S Desmeules4, BW Gillespie5, T Depner6, P Klassen7 and FK Port2 Figure 1 | Relative risk of mortality by dialysis type. (Adjusted for age, sex, time on dialysis, 14 summary comorbid conditions, weight, catheter use, hemoglobin, albumin, normalized protein catabolic rate, cholesterol, triglycerides, Kt/V, erythropoietin, MCS, and PCS.) Kidney Int (2006) 69, 2087–2093 Conclusion This is the first large observational cohort study with robust adjustments for demographic and comorbid confounding factors to show an association with lower mortality risk for HDF. The modality’s beneficial effects on patient outcomes are not related to dialysis dose for small molecules (Kt/Vurea), but may be related to factors particular to HDF, which combines enhanced removal of larger molecular weight substances with an improved biocompatible system. n = 2165, adjusted for age, sex, time on dialysis, comorbidity. Weight, catheter, Hb, alb, nPCR, Kt/V, EPO, Qol Kidney Int (2006) 69, 2087–2093
 Kidney Int (2006) 69, 2087–2093. Conclusion. This is the first large observational cohort study with robust. adjustments for demographic and comorbid confounding. factors to show an association with lower mortality risk for. HDF. The modality’s beneficial effects on patient outcomes. are not related to dialysis dose for small molecules (Kt/Vurea), but may be related to factors particular to HDF, which. combines enhanced removal of larger molecular weight. substances with an improved biocompatible system. n = 2165, adjusted for age, sex, time on dialysis, comorbidity. Weight, catheter, Hb, alb, nPCR, Kt/V, EPO, Qol. Kidney Int (2006) 69, 2087–2093.")
30
Masalah Pada Hemodiafiltrasi
Penggabungan konveksi dan difusi Kualitas dan kuantitas cairan reinfusi Kehilangan komponen fisiologis dalam ultrafiltrat ?

31
Adsorption by hydrophobic resin
Hemo- diafiltration Reinfusion (HFR) Qbi Qbo Qdi Qdo Out QR Convection Diffusion QR = Out ∆ Weight Adsorption by hydrophobic resin HFR metoda dialisis yang menggunakan konveksi, difusi dan adsorpsi pada waktu yang sama . Dializer terdiri menjadi 2 bagian satu untuk konveksi dan satu untuk difusi
 Qbi. Qbo. Qdi. Qdo. Out. QR. Convection. Diffusion. QR = Out. ∆ Weight. Adsorption by hydrophobic resin. HFR metoda dialisis yang menggunakan konveksi, difusi dan adsorpsi pada waktu yang sama . Dializer terdiri menjadi 2 bagian satu untuk konveksi dan satu untuk difusi.")
32
Hemodiafiltrasi dengan reinfusi endogen
uf Convection (through protein leaking membrane) Pembuangan toksin uremik dengan adsorpsi Reinfusi dari molekul fisiologis Adsorption Dialysate out Diffusion Dialysate in
 Pembuangan toksin uremik dengan adsorpsi. Reinfusi dari molekul fisiologis. Adsorption. Dialysate out. Diffusion. Dialysate in.")
33
Selecta sorbent cartridge
40 mL of free resin in physiological solution Great sorbing surface (more than 700 m 2/mL of resin) High efficiency for medium-high molecular weight solutes.
 High efficiency for medium-high molecular weight solutes.")
34
HFR – APA SAJA YANG DIADSORPSI
Interleukin 5 Interleukin 6 Interleukin 7 Interleukin 8 Interleukin 10 (?) Interleukin 12p70 Interleukin 16 Interleukin 18 Macrophage inflammatory protein-a (MIP-a) Macrophage inflammatory protein-b (MIP-b) Tumor necrosis factor-a (TNF-a) Monocyte chemotactic protein (MCP-1) Epithelial neutrophil activating peptide 78 (ENA-78) Angiogenina b2 microglobulin Homosistein
 Interleukin 12p70. Interleukin 16. Interleukin 18. Macrophage inflammatory protein-a (MIP-a) Macrophage inflammatory protein-b (MIP-b) Tumor necrosis factor-a (TNF-a) Monocyte chemotactic protein (MCP-1) Epithelial neutrophil activating peptide 78 (ENA-78) Angiogenina. b2 microglobulin. Homosistein.")
35
HFR – APA YANG TIDAK DIADSORPSI
Urea Creatinin Uric acid Fosfat Glucosa Na + K + Ca ++ Mg ++ HCO3- Asam amino esensial Asam amino lain Albumin

36
PASIEN KANDIDAT HFR Malnutrition Inflammation Syndrome Malnutrition
Chronic Inflammation Atherosclerosis General Poor Condition

37
Inflammation is common in CKD and HD patients
Sweden Stenvinkel et al. 1990 Italy Zoccali et al. 2000 Sweden Qureshi et al. 1998 Germany Zimmermann et al. 1989 USA Yeun et al. 2000 Spain (Cordoba) Santamaria et al. 2001
 Santamaria et al")
38
Status Pro-inflammatory pada hemodialisis Faktor
Oxidative stress * Dialysis-dependents * Dialysis-independents PROSEDUR “UREMIA” 38

40
Variasi kadar serum CRP selama studi
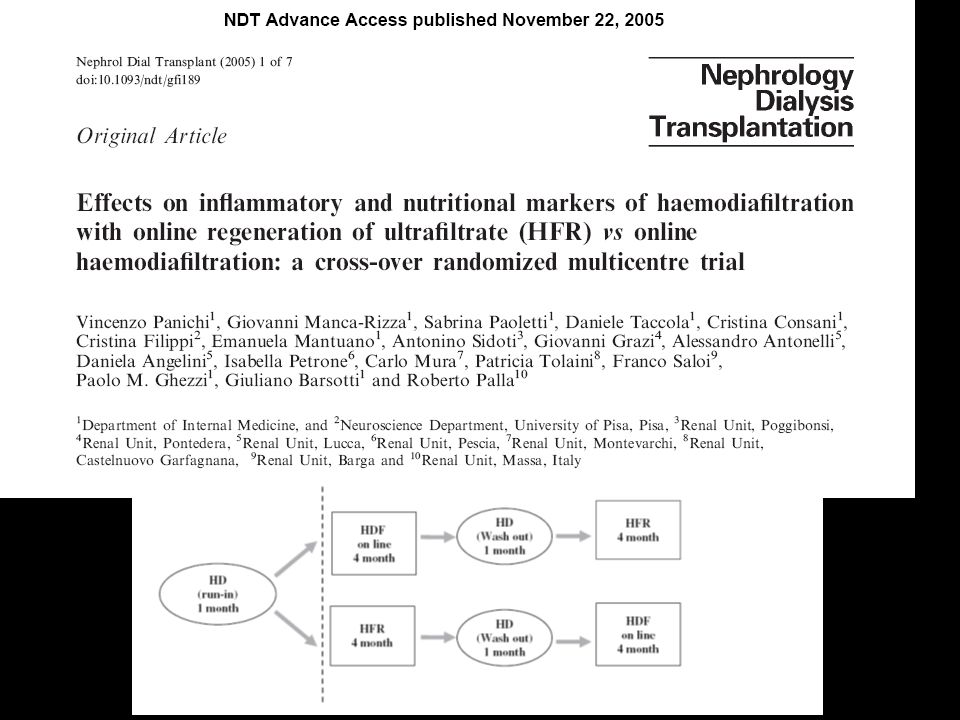
Fig. 2. Variations in serum CRP level during the study. Plasma CRP was significantly reduced after 1 and 4 months of HFR (P<0.04) in comparison to the HD month. Furthermore, CRP significantly increased (P<0.03) when patients were transferred from HFR4 to HD. Finally, CRP was significantly reduced after 4 months of HDF (P<0.05). As shown in Figure 1, after 1 month of bicarbonate dialysis (HD) patients were randomized to start either HFR or HDF. In this figure the cumulative results for each technique are depicted. Panichi, V. et al. Nephrol. Dial. Transplant : ; doi: /ndt/gfi189
 in comparison to the HD month. Furthermore, CRP significantly increased (P<0.03) when patients were transferred from HFR4 to HD. Finally, CRP was significantly reduced after 4 months of HDF (P<0.05). As shown in Figure 1, after 1 month of bicarbonate dialysis (HD) patients were randomized to start either HFR or HDF. In this figure the cumulative results for each technique are depicted. Panichi, V. et al. Nephrol. Dial. Transplant : ; doi: /ndt/gfi189.")
41
Variasi kadar serum IL-6 selama studi
Fig. 3. Variations in serum IL-6 level during the study. Plasma IL-6 was significantly reduced after 4 months of HFR (P<0.04) in comparison to the HD month. Furthermore, IL-6 significantly increased (P<0.04) when patients were transferred from HFR4 to HD. Finally, no significant reduction of IL-6 was observed during the 4 months of HDF (NS). As shown in Figure 1, after 1 month of bicarbonate dialysis (HD) patients were randomized to start either HFR or HDF. In this figure the cumulative results for each technique are depicted. Panichi, V. et al. Nephrol. Dial. Transplant : ; doi: /ndt/gfi189
 in comparison to the HD month. Furthermore, IL-6 significantly increased (P<0.04) when patients were transferred from HFR4 to HD. Finally, no significant reduction of IL-6 was observed during the 4 months of HDF (NS). As shown in Figure 1, after 1 month of bicarbonate dialysis (HD) patients were randomized to start either HFR or HDF. In this figure the cumulative results for each technique are depicted. Panichi, V. et al. Nephrol. Dial. Transplant : ; doi: /ndt/gfi189.")
42
Kebutuhan ESA Bolasco, Granada 2009 P = 0.01 BHD HFR AF 1 HFR std
BHD start HFR AF 1 end HFR std start HFR AF 2 end BHD end HFR AF 1 start HFR std end HFR AF 2 start Bolasco, Granada 2009

43
Korelasi antara Hb dan kebutuhan ESA
ESAs IU/month (x 1000) Y = x R2 = 0.63 r = Hb (g/dL) Bolasco, Granada 2009
 Y = x R2 = r = Hb (g/dL) Bolasco, Granada")
44
AA Non Esensial p < 0.05 * AA a catena ramificata in HFR e in HDF on-line Ragazzoni E et al. Giorn It Nefrol 2004; 21 (Suppl 30): S85-S90 Studio clinico comparativo su plasma (n = 11) Ragazzoni E et al. Giorn It Nefrol 2004; 21 S85-S90 Studio clinico comparativo su plasma (n = 11)
: S85-S90 Studio clinico comparativo su plasma (n = 11) Ragazzoni E et al. Giorn It Nefrol 2004; 21 S85-S90 Studio clinico comparativo su plasma (n = 11)")
45
AA Esensial p < 0.05 * AA essenziali in HFR e in HDF on-line Ragazzoni E et al. Giorn It Nefrol 2004; 21 (Suppl 30): S85-S90 Studio clinico comparativo su plasma (n = 11) Ragazzoni E et al. Giorn It Nefrol 2004; 21: S85-S90 Studio clinico comparativo su plasma (n = 11)
: S85-S90 Studio clinico comparativo su plasma (n = 11) Ragazzoni E et al. Giorn It Nefrol 2004; 21: S85-S90 Studio clinico comparativo su plasma (n = 11)")
46
46

47
47

48
Kadar Hemoglobin Pasien dengan HFR
Th/ EPO Stop 48

49
Kadar β2M pada pasien dengan HFR
Pasien A Pasien B 49

50
Kesimpulan (1) Evolusi teknologi HDF membuat teknik lebih sederhana dan aman Modifikasi HDF standar dapat mengeksplorasi modalitas terapi baru yang tetap mempertahankan prinsip kombinasi difusi dan konveksi HDF sudah jelas memberikan keuntungan tetapi pasien GGT tetap memiliki masalah dengan inflamasi, stress oksidatif dan morbiditas dan mortalitas tinggi karena kelainan kardiovaskular.

51
Kesimpulan (2) Berbagai tipe RRT harus memberikan efek yang baik dari pembuangan toksi dengan sesedikit mungkin kehilangan substansi fisiologis. HFR mungkin dapat menawarkan keuntungan dalam hal-hal yang berhubungan dengan inflamasi dan nutrisi pada pasien-pasien dengan faktor komorbid yang tinggi atau sindroma malnutrisi inflamasi dan atherosklerosis (MIA syndrome)
")
Presentasi serupa


 dan STATUS NUTRISI : MALNUTRISION INFECTION SCORE (MIS) PADA PASIEN YANG MENJALANI HEMODIALISIS REGULER.>")

















