Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
INSULIN DAN ANTI DIABETIK ORAL
Dr. dr. NURDIANA, M.Kes LAB. FARMAKOLOGI FK UNIBRAW MALANG

2
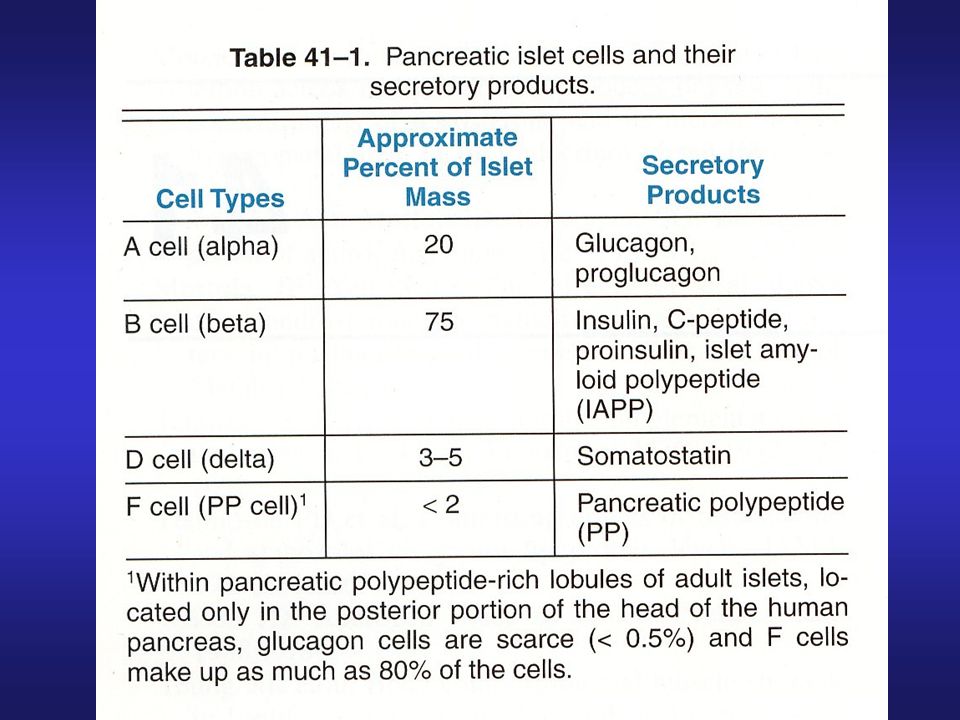
PANKREAS 1 juta pulau langerhans memproduksi hormon (lihat tabel)
SEL B PANKREAS SINTESIS oleh DNA ATAU RNA INSULIN BM : 5808 2 RANTAI : RANTAI A RANTAI B lihat gambar RANTAI DISULFIDA PROINSULIN RANTAI TUNGGAL, PANJANG DIPROSES DALAM GOLGI APPARATUS MENJADI INSULIN (HIDROLISA), SEGMEN SISANYA C-PEPTIDA INSULIN DISEKRESI SETARA DENGAN STIMULAN/ SECRETAGOGUES
, SEGMEN SISANYA C-PEPTIDA. INSULIN DISEKRESI SETARA DENGAN STIMULAN/ SECRETAGOGUES.")
4
STRUKTUR PROINSULIN MANUSIA

5
SEKRESI INSULIN Insulin dilepas dari sel B pankreas : Low basal rate : tanpa stimuli dari luar Much higher stimulated rate : ada stimuli dari luar terutama glukosa stimuli lain mannose, asam amino : leucine,arginin, rangs vagus EFEK FISIOLOGI INSULIN MENURUNKAN KADAR GULA DARAH Interaksi glukosa-insulin neg feed back mengatur agar kadar gula darah segera kembali normal

6
FARMAKODINAMIK INSULIN
INSULIN AGONIS INSULIN SIRKULASI BERIKATAN DENGAN RESEPTOR PADA MEMBRAN SEL , MENGHASILKAN RESPON BIOLOGIS YANG SESUAI SIFAT KOMPLEKS IKATAN. TARGET TISSUE TERUTAMA : HATI, OTOT, JARINGAN LEMAK INSULIN BERIKATAN DG RESEPTOR DG SPESIFISITAS DAN AFINITAS TINGGI (picomolar). FARMAKOKINETIK INSULIN INSULIN TIDAK DIBERIKAN PERORAL KARENA DIRUSAK OLEH PEPTIDASE DI G.I.T. , SEHINGGA DIBERIKAN SC, IM, IV, NASAL SPRAY DAN IMPLANTABLE PUMP INSULIN ABSORBSI DARAH CAIRAN EKSTRASEL DISTRB HALF LIFE : ORG SEHAT, CEPAT, DL BEBERAPA MENIT DM, LBH LBT, KARENA BERIKATAN DG ANTIBODI METAB : LIVER, OTOT DAN GINJAL EKSKRESI : METABOLIT, FRAKSI KECIL YG T’BERUBAH GINJAL
. FARMAKOKINETIK INSULIN. INSULIN TIDAK DIBERIKAN PERORAL KARENA DIRUSAK OLEH PEPTIDASE DI G.I.T. , SEHINGGA DIBERIKAN SC, IM, IV, NASAL SPRAY DAN IMPLANTABLE PUMP. INSULIN ABSORBSI DARAH CAIRAN EKSTRASEL DISTRB. HALF LIFE : ORG SEHAT, CEPAT, DL BEBERAPA MENIT. DM, LBH LBT, KARENA BERIKATAN DG ANTIBODI. METAB : LIVER, OTOT DAN GINJAL. EKSKRESI : METABOLIT, FRAKSI KECIL YG T’BERUBAH GINJAL.")
7
Efek fisiologis Insulin metab. glukosa
transport aktif glukosa utk masuk ke dl sel * meningkatkan penggunaan glukosa oleh jar. tbh * meningkatkan glikogenesis di otot dan hati * oksidasi KH utk enersi di otot bergaris Meningkatkan sintesis lemak di di jar lemak glukoneogenesis , glikogenolisis peningkatan sintesis protein dan as. nukleat pertumbh oksidasi lemak utk enersi ketosis insulin proses anabolik glukosa produksi enersi disimpan (storage)
")
8
Insulin hati otot Jar.lemak

9
Fluktuasi kadar glukosa dalam serum dipengaruhi faktor-faktor :
Glkogenolisis/glukoneogenesis Penggunaan glukosa oleh sel perifer Jumlah reseptor insulin pada sel Kadar antibodi insulin Hormon yg mempengaruhi metab. Glukosa : insulin, glucagon, cortison, epinefrin dan GH Insulin, vit C, chromium me metab glukosa. Exercise me penggn glukosa KONDISI PATOLOGIS Ggn sekresi insulin : meningkat : reactive hypoglycemia, insulinoma menurun : defisiensi insulin DM DM bisa disebabkan antibodi yg menghalangi kerja insulin atau kurangnya reseptor insulin, kemampuan jar menggunakan glukosa (obesitas)
")
10
Sifat preparat insulin
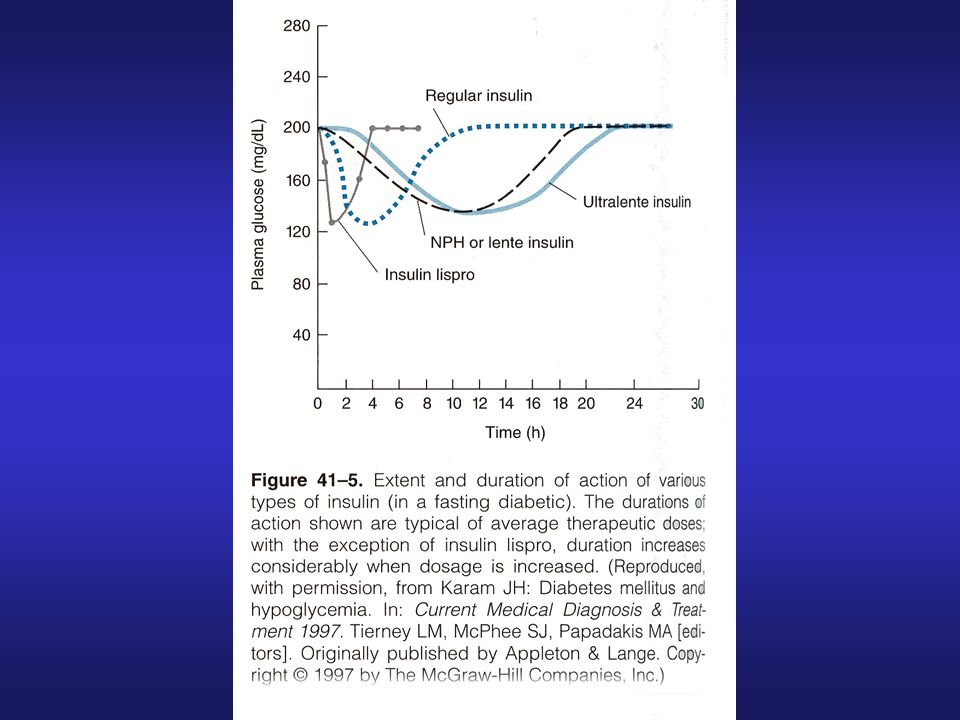
A. Tipe dan lama kerja Ultra short acting, very rapid onset, short duration Short acting, rapid onset of action Intermediate-acting Long – acting, slow onset of action tabel

12
Degradasi insulin Pengukuran insulin
- dilakukan oleh hati dan ginjal, membersihkan insulin dari sirkulasi Cara hidrolisis ikatan disulfid antara rantai A dan B melalui kerja insulinase (glutathione insulin transhidrogenase) proteolysis Insulin endogen hati : 60 % ginjal % Insulin eksogen, sebaliknya Circulating insulin half life 3-5’ Pengukuran insulin RIA picomolar, berdasarkan reaksi dg antibodi bisa mengukur insulin sapi, babi dan manusia basal insulin value, 5 – 15 U/ml (30-90 mol/L)pada manusia, kadar puncak U/ml ( mol/L), pada saat makan.
 proteolysis. Insulin endogen hati : 60 % ginjal % Insulin eksogen, sebaliknya. Circulating insulin half life 3-5’ Pengukuran insulin. RIA picomolar, berdasarkan reaksi dg antibodi. bisa mengukur insulin sapi, babi dan manusia. basal insulin value, 5 – 15 U/ml (30-90 mol/L)pada manusia, kadar puncak U/ml ( mol/L), pada saat makan.")
13
TERAPI INSULIN DIABETES TIPE 1 INSULIN DEPENDENT GROUP DIABETES TIPE 2TDK BTH INSULIN UTK SURVIVAL, TP UTK OPTIMAL HEALTH “GLYCEMIC CONTROL” PADA DM DM TIPE 1 COMPREHENSIVE SELF-MANAGEMENT TRAINING, DIMULAI SESUDAH PUBERTAS UMUR 7 TH , TDK BOLEH KONTROL KETAT, KARENA HIPOGLIKEMI DPTBRAIN DAMAGE KOMPLIKASI TERAPI INSULIN HIPOGLIKEMI PENYEBAB : TERLAMBAT MAKAN AKTIVITAS FISIK TDK SESUAI DOSIS INSULIN > UTK KEPERLUAN MENDADAK

14
ORANG TUA DG DMMENDPT “LONG ACTING INSULIN”
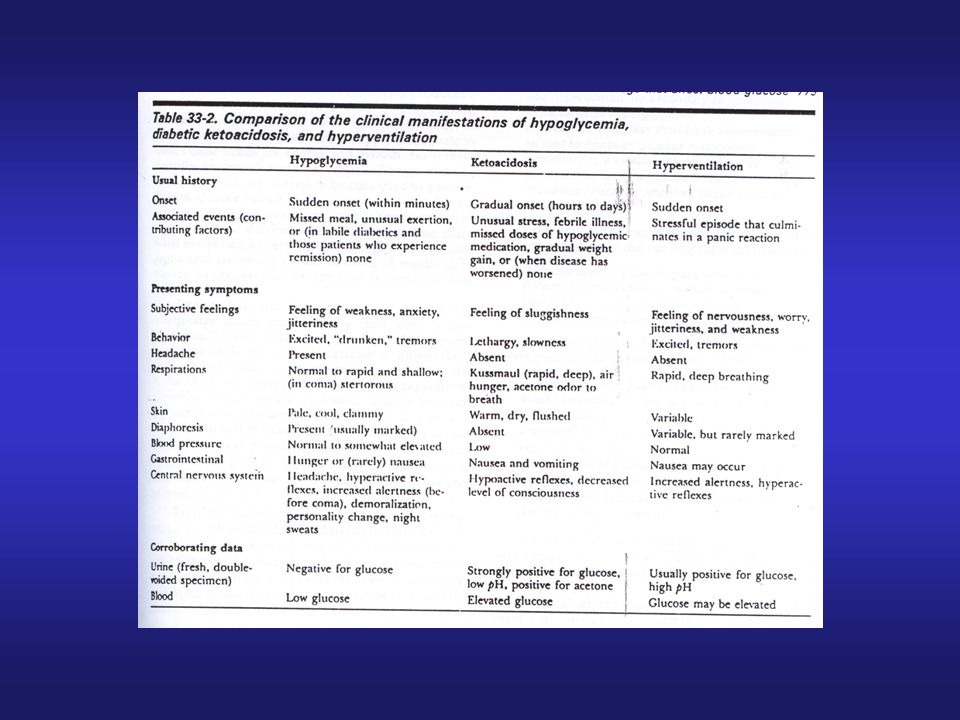
-AUTONOMIC WARNING : SIMP : Takikardi, palpitasi,sweating, tremor SIGNAL P.SIMP : Nausea, lapar -KEGGL FS CNS : Mental confusion, bizzare behaviour, coma TERAPI HIPOGLIKEMIA Berikan glukosa * mild hipoglycemia, sadar, dpt menelan : makanan manis * more severe, stupor ml gluc 50 % i.v glucagon 1 mg s.c atau i.m. B. IMMUNOPATHOLOGY OF INSULIN THERAPY Insulin antibodi IgA, IgD, IgE, IgG dan IgM 2 gangguan immunitas pd DM dg terapi insulin : 1 Alergi insulin : urtikaria , syok anafilaktik,nodul ditempat suntikan makin murni insulin, alergi

15
2. Immune insulin resistance :
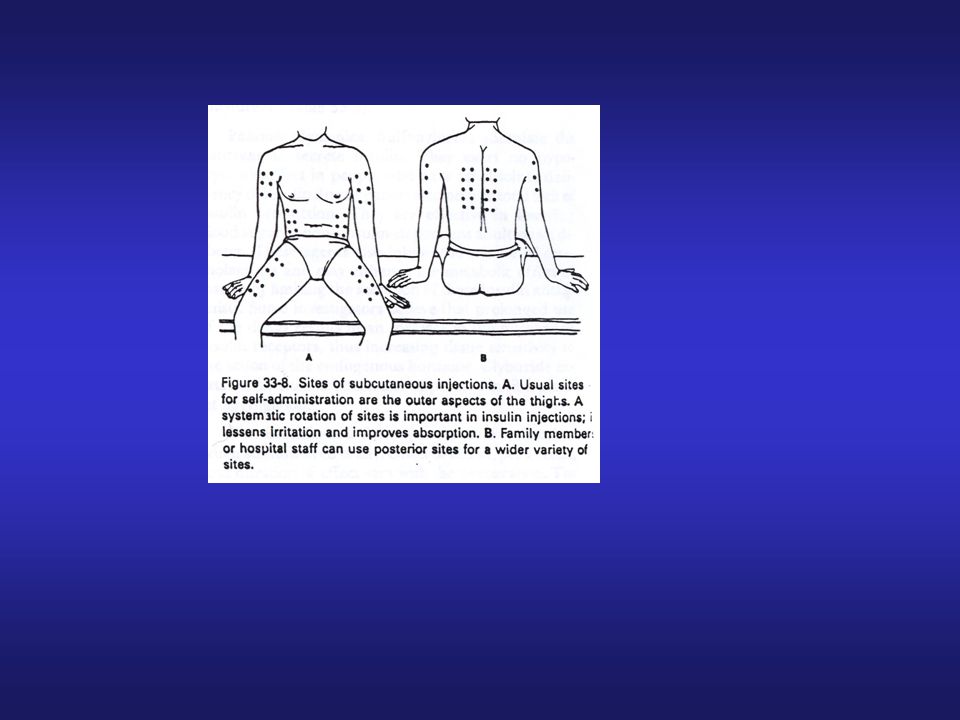
a. Tx insulin : low titer IgG anti insulin antibodies b. a+ terapi insulin kurang murni +jar kurang sensitif insulinIgG antiinsulin antibodies kebutuhan insulin > 200 U/hari LIPODISTROPI PADA TEMPAT INJEKSI Sudah berkurang karena insulin babi dan manusia yang murni, pH netral. Sekarang terjadi hipertropi lemak s.c bl disuntik berulang ditempat yg sama liposuction

17
Type 2 diabetes: the role of insulin resistance and -cell failure
Hyperinsulinaemia Increasing insulin resistance + -cell failure Impaired glucose tolerance It is not clear whether it is insulin resistance or -cell failure that is the primary defect in Type 2 diabetes – it is likely to be a combination of both. The onset of insulin resistance results in compensatory hyperinsulinaemia. With increasing insulin resistance, the -cells fail to compensate fully for the increased insulin resistance and a state of impaired glucose tolerance arises. As -cell function deteriorates further, glucose tolerance continues to fall resulting in overt Type 2 diabetes. Eventually, when the -cells fail completely, a state of hypoinsulinaemia arises and the individual will require therapy with insulin. Type 2 diabetes Adapted from: Reaven GM. Diabetes 1988;37:1595–1607 and Beck-Nielsen H, Groop LC. J Clin Invest 1994;94:1714–1721 Reaven GM. Diabetes 1988;37:1595–1607 Beck-Nielsen H, Groop LC. J Clin Invest 1994;94:1714–1721

18
OAD (oral anti diabetic)
OBAT DoA (jam) SULFONILUREA Chlorpropamid -Tolbutamid -Glimepirid -Glipizid -Gliburid MIGLITINID Repaglinid S/d 60 6-12 12-24 10-24 1-3 BIGUANID Metformin 10-12 THIAZOLIDINNEDION -Pioglitazone -Rosiglitazone 15-24 >24 -GLUCOSIDASE INHIBITOR -Acarbose 3-4
 SULFONILUREA -Chlorpropamid. -Tolbutamid. -Glimepirid. -Glipizid. -Gliburid. MIGLITINID -Repaglinid. S/d BIGUANID -Metformin THIAZOLIDINNEDION -Pioglitazone. -Rosiglitazone >24. -GLUCOSIDASE INHIBITOR. -Acarbose")
19
INSULIN SECRETAGOGUES
1. SULFONYLUREA : GENERASI 1 : CHLORPROPAMIDE, TOLBUTAMIDE, TOLAZAMIDE GENERASI 2 : GLYBURIDE, GLIPIZIDE, GLIMEPIRIDE kelebihan generasi 2 : efek samping dan interaksi obat lbh sedikit hati-hati pada pasien dg penderita peny.jantung dan orang tua hipoglikemia 2. MEGLITINIDE : REPAGLINIDE onset of action cepat, peak conc.1 jam, duration of act 5-8 jam kontrol gula darah postprandial 3. D-PHENYLALANINE DERIVATIVE : NATEGLINIDE digunakan sebelum makan, masa kerja pendek (<4jam). tdk perlu titrasi dosis, insiden hipoglikemi rendah
. tdk perlu titrasi dosis, insiden hipoglikemi rendah.")
20
Sulphonylureas 1st generation : chlorpropamid 2nd generation : gliclazide, glipizide gliburid, glibenklamid 3nd generation : glimepiride Others : Meglitinide : Repaglinide utk DM tipe 2 yg alergi sulfonylurea Nateglinide Stimulate beta cells to release insulin (assumes there is residual beta cell activity) Side effects: hypoglycaemia, weight gain, GI disturbances, headache
 Side effects: hypoglycaemia, weight gain, GI disturbances, headache.")
21
EFEK SAMPING Sulfonilurea -nausea, vomiting -jaundice
-agranulositosis, anemia aplastik -teratogenik -toksik : Hipoglikemi

22
Sulfonylureas: Mechanism of Action
1 Intestine: glucose absorption 2 Muscle and adipose tissue: glucose uptake Insulin resistance Blood glucose 4 Liver: hepatic glucose output Insulin resistance Pancreas: insulin secretion Sulfonylureas insulin secretion DeFronzo RA. Diabetes. 1988;37: Lebovitz HE. In Joslin's Diabetes Mellitus. 1994:

23
Meglitinides: Mechanism of Action
1 Intestine: glucose absorption 2 Muscle and adipose tissue: glucose uptake Insulin resistance Blood glucose 4 Liver: hepatic glucose output Insulin resistance 3 Pancreas: insulin secretion Meglitinides Insulin secretion Wolffenbuttel BHR. Eur J Clin Pharmacol. 1993;45:

24
Biguanides Metformin Drug of choice in obese patients only
Monotherapy or adjunct Decreases gluconeogenesis Increases peripheral uptake of glucose in to cells Basal & post prandial glucose levels Weight neutral Increased insulin sensitivity Beneficial effect on plasma lipid profile

25
Metformin: Mechanism of Action
1 Intestine: glucose absorption 2 Muscle and adipose tissue: glucose uptake Metformin glucose utilization Insulin resistance Blood glucose 4 Liver: hepatic glucose output Metformin HGO Insulin resistance 3 Pancreas: insulin secretion DeFronzo RA et al. J Clin Endocrinol Metab. 1991;73:

26
Metformin cont’d Side effects
Nausea, vomiting, diarrhoea, abdominal discomfort

27
a-Glucosidase Inhibitors :Mechanism of Action
1 Intestine: glucose absorption Acarbose glucose absorption secondary to digestion of carbohydrate 2 Muscle and adipose tissue: glucose uptake Insulin resistance Blood glucose 4 Liver: hepatic glucose output Insulin resistance 3 Pancreas: insulin secretion Amatruda JM. In: Diabetes Mellitus

28
Alpha glucosidase inhibitors
Acarbose monotherapy or adjunct Inhibits intestinal enzyme, specific activity on sucrase, delaying digestion of starch and sucrose into absorbable monosaccharides such as glucose Safe Weight neutral

29
Acarbose cont’d Side effects: GI intolerance
flatulence, diarrhoea, abdominal distension & pain

30
Thiazolidinediones: Mechanism of Action
Muscle and adipose tissue: Thiazolidinediones insulin resistance glucose uptake Intestine: glucose absorption Liver: hepatic glucose output Thiazolidinediones HGO Blood glucose Improve b-cell function Pancreas: insulin secretion Whitcomb RW et al. In: Diabetes Mellitus Cavaghan MK et al. J Clin Invest. 1997;100: Ehrmann DA et al. J Clin Endocrinol Metab. 1997;82:

31
The PPAR Family (Peroxisome proliferator-activated receptor)
Fibrates Thiazolidinediones Fatty acids Ligand Receptor PPAR-a PPAR-g PPAR-d Effect on: Lipoprotein expression Peroxisome proliferation Lipid synthesis Carbohydrate metabolism Saltiel AR, Olefsky JM. Diabetes. 1996;45:

32
Thiazolidinediones Counteract insulin resistance
Bind to PPAR-gamma (receptor), forming a complex promoting transcription of genes sensitive to insulin. Receptors are present in skeletal muscle, adipose tissue &liver, thereby promoting uptake of fatty acids &glucose at these sites
, forming a complex promoting transcription of genes sensitive to insulin. Receptors are present in skeletal muscle, adipose tissue &liver, thereby promoting uptake of fatty acids &glucose at these sites.")
33
Thiazolidinediones cont’d
Pioglitazone, rosiglitazone Adjunct with either metformin or SU

34
Thiazolidinediones ? Alternative to insulin Side effects:
oedema, weight gain, GI disturbances, headache, dizziness

35
Sites of Action by Therapeutic Options
PANCREAS LIVER Therapy: Biguanides Thiazolidinediones Therapy: Sulfonylureas Meglitinides Insulin DECREASED INSULIN SECRETION INCREASED GLUCOSE PRODUCTION HYPERGLYCEMIA DECREASED PERIPHERAL GLUCOSE UPTAKE INTESTINE Slide V/13 Biguanides work principally at the liver, decreasing hepatic glucose output.155 Metformin, the only biguanide available, is particularly useful in obese patients as it does not produce weight gain and may facilitate weight reduction. Side effects, particularly those affecting the gastrointestinal system, are not uncommon, however, and care is necessary to avoid lactic acidosis, the most dangerous side effect. The UKPDS provides evidence of its benefit as single therapy, with equivocal results in combination with a sulfonylurea.107 Sulfonylureas reduce blood glucose concentrations by stimulating insulin secretion through their effect on ATP-sensitive potassium channels in the beta cell.155 Their use is associated with weight gain, their long-term safety as regards macrovascular disease has been in doubt since publication of the UGDP study;137 however, this was not confirmed in the UKPDS.50 Alpha-glucosidase inhibitors decrease glucose absorption by inhibiting the breakdown of disaccharides to monosaccharides. They reduce postprandial glycemia and HbA1c levels.156 Poor tolerability due to mild to moderate gastrointestinal side effects limits their use. The thiazolidinediones are a new class whose first member is troglitazone.157 These agonists for peroxisome proliferator-activated receptor (PPAR) gamma improve insulin sensitivity in muscle and adipose tissue.155 The class is effective alone and particularly in combination with sulfonylureas or metformin. Use of troglitazone requires careful monitoring because of idiosyncratic hepatic toxicity.157 Type 2 diabetics often need insulin eventually,158 but it can be associated with weight gain. Combining insulin with metformin or troglitazone is useful. INCREASE GLUCOSE ABSORPTION ADIPOSE TISSUE Therapy: Alpha-glucosidase inhibitors Therapy: Thiazolidinediones (Biguanides) MUSCLE Adapted from Sonnenberg and Kotchen Curr Opin Nephrol Hypertens 1998;7(5):
 gamma improve insulin sensitivity in muscle and adipose tissue.155 The class is effective alone and particularly in combination with sulfonylureas or metformin. Use of troglitazone requires careful monitoring because of idiosyncratic hepatic toxicity.157. Type 2 diabetics often need insulin eventually,158 but it can be associated with weight gain. Combining insulin with metformin or troglitazone is useful. INCREASE. GLUCOSE. ABSORPTION. ADIPOSE TISSUE. Therapy: Alpha-glucosidase. inhibitors. Therapy: Thiazolidinediones. (Biguanides) MUSCLE. Adapted from Sonnenberg and Kotchen Curr Opin Nephrol Hypertens 1998;7(5):")
36
EFEK SAMPING Sulfonilurea -nausea, vomiting -jaundice
-agranulositosis, anemia aplastik -teratogenik -toksik : Hipoglikemi Biguanid : -asidosis laktat -nausea, diare -menghambat absorpsi vit.B12 Thiazolidindione -jarang hipoglikemi -udema, anemia ringan Glukosidase inhibitor: -flatulen, diare, nyeri abdomen

37
TAHAPAN TERAPI DIABETES MELITUS
Diagnosis Health education Diet, exercise, weight control Oral agent monotherapy SU, metformin, meglitinide, thiazolidinedione, acarbose Oral agent combination therapy (2 different classes) Insulin + oral agent Insulin
 Insulin + oral agent. Insulin.")
38
Stepwise management of type 2 diabetes
Insulin ± oral agents Oral combination Oral monotherapy Type 2 diabetes is traditionally treated in a stepwise manner. Initial therapy is usually diet and increased exercise. However, lifestyle measures generally fail to control glycaemia and, therefore, pharmacological treatment is instigated. Initial therapy is with a single oral drug although monotherapy often fails over a period of time and a combination of two or more oral therapies is used. Subsequently, failure of all oral combination therapy may occur when -cell failure has progressed to such a degree that additional, exogenous insulin is required. Diet & exercise

Presentasi serupa
 atau oleh makanan, obat tradisional dan senyawa.>")


















