Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
NEUROPATHIC PAIN Candy Lauwrenz

2
Definisi nyeri : International Association for the Study of Pain (IASP) : “Nyeri adalah pengalaman sensorik dan emosional yang tidak menyenangkan akibat kerusakan jaringan, baik aktual maupun potensial atau yang digambarkan dalam bentuk kerusakan tersebut”.
 : Nyeri adalah pengalaman sensorik dan emosional yang tidak menyenangkan akibat kerusakan jaringan, baik aktual maupun potensial atau yang digambarkan dalam bentuk kerusakan tersebut .")
3
Nyeri adalah suatu pengalaman sensorik yang multi dimensional.
Fenomena ini dapat berbeda dalam intensitas (ringan, sedang, berat), kualitas (tumpul, seperti terbakar, tajam), durasi (transien, intermiten, persisten), dan penyebaran (superfisial vs dalam, terlokalisir vs difus)
, kualitas (tumpul, seperti terbakar, tajam), durasi (transien, intermiten, persisten), dan. penyebaran (superfisial vs dalam, terlokalisir vs difus)")
4
Pain: “The Fifth Vital Sign“ the Joint Commission on
Accreditation of Healthcare Organizations menyebutkan nyeri sebagai “The Fifth Vital Sign“ yg harus di monitor pada perawatan pasien , bersama dng suhu , nadi , respirasi , dan tekanan darah . (Campagnolo. 2005)
")
5
CLINICAL PAIN PHYSIOLOGIC PAIN /
Classification: PAIN CLINICAL PAIN PHYSIOLOGIC PAIN / TRANSIENT PAIN Nociceptive Psychogenic Neuropathic (inflammatory) Somatic Visceral Peripheral Central Superficial Symphatic Deep • Acute : < 3-6 months, mostly nociceptive • Chronic : > 3-6 months, mostly neuropathic
 Somatic Visceral Peripheral Central. Superficial Symphatic. Deep. • Acute : < 3-6 months, mostly nociceptive. • Chronic : > 3-6 months, mostly neuropathic.")
6
There are Two Sensory Afferent Neurons
Large myelinated A fibers Very fast conduction velocity Respond to innocuous stimuli Small myelinated A & C unmyelinated fibers Slow conduction velocity Respond to noxious stimuli Large fibers A Dorsal root ganglion Dorsal Horn A Small fibers C Peripheral sensory Nerve fibers

7
Normal Nerve Impulses Leading to Pain
Perceived pain Noxious stimuli Coba cari film transduksi – transmisi – modulasi – persepsi Descending modulation Ascending input Nociceptive afferent fiber Spinal cord

8
Nociception Perception Modulation Transmission Transduction Pain
Descending modulation Dorsal Horn Transmission Ascending input Dorsal root ganglion Transduction Spinothalamic tract Peripheral nerve Trauma Peripheral nociceptors Adapted from Gottschalk A et al. Am Fam Physician. 2001;63:1981, and Kehlet H et al. Anesth Analg. 1993;77:1049. 8

9
CAUSES OF NOCICEPTIVE PAIN
ACUTE PAIN SYNDROME Skin/subcutan Muscle Tendon Ligment Bone Joint Vascular Visceral Cancer Postoperative strain tendinitis sprain Abscess,bruise ischemic avulsion fracture superficial pain d e e p p a i n PAD angina visceral pain

10
NEUROPATHIC PAIN vs NOCICEPTIVE PAIN
Characteristic Nociceptive Neuropathic • Cause Often identifiable Rarely unidentifiable • Duration Mostly acute Mostly chronic (<3 months) (>3 months) • Sensation = stimulus ≠ stimulus 1 cause 1 sen- 1 cause > 1 sen- sation sation
 (>3 months) • Sensation = stimulus ≠ stimulus 1 cause 1 sen- 1 cause > 1 sen- sation sation")
11
Neuropathic Pain

12
Menurut IASP (International Association for the Study of Pain);
Nyeri neuropatik adalah nyeri yang diawali atau disebabkan lesi primer atau disfungsi atau gangguan yang menetap pada sistem saraf perifer ataupun saraf sentral (Planjar et al dan Treede et al. 2007).
.")
13
CAUSES OF NEUROPATHIC PAIN

14
Central Causes of Neuropathic Pain
Spinal Rood/Dorsal Ganglion Prolapsed disc Root avulsion Post herpetic neuralgia Surgical rhizotomy Trigeminal neuralgia Arachnoiditis Tumour Spinal Cord. Trauma including compression Syringomyelia and intrinsic tumour Vascular: Infarction, hemorrhagic and AVM Syphilis Anterolateral cordotomy Multiple sclresosis Spinal dysraphisme Vitamin B12 deficiency HIV Brain Stem Lateral medulary syndrome Multiple sclerosis Tuberculoma Thalamus Infarction Hemorrhage Tumours Surgical lesion Sub-cortical and Cortical Infarct Trauma AVM Tumour

15
Peripheral Causes of Neuropathic Pain
Mononeuropathies and multiple mononeuropathies Trauma: compression, transaction, post thoracothomy, painful scars Diabetic: mononeurpathy and amyothropy Neuralgic amyothrophy. Connection tissue diseases. Malignant and radiation plexopathy,Trench foot ,Borreliosis. Polyneuropathies Metabolic Nuritional Diabetic Alcoholic Pellagra Beri beri Amyloid Cuban neuropathy Tanzanian neuropathy Burning feet syndrome Jamaican neuropathy Drugs/Toxic Isoniazid Cisplatin Thalium Vincristin Arsenic Clioquinol Disulfiram Nitrofurantoin Infection HIV Acute Inflammatory polyneuropathy (Guillain Barre) / CIDP Hereditary Fabry’s disease Dominantly inherited sensory neuropathy / HSAN Malignant Myeloma
 / CIDP. Hereditary. Fabry’s disease. Dominantly inherited sensory neuropathy / HSAN. Malignant. Myeloma.")
16
Presentation Across Pain States Varies
Neuropathic Pain Pain initiated or caused by a primary lesion or dysfunction in the nervous system (either peripheral or central nervous system)1 Nociceptive Pain Pain caused by injury to body tissues (musculoskeletal, cutaneous or visceral)2 Mixed Pain Pain with neuropathic and nociceptive components Examples Peripheral Post-herpetic neuralgia Trigeminal neuralgia Diabetic peripheral neuropathy Post-surgical neuropathy Post-traumatic neuropathy Central Post-stroke pain Common descriptors2 Burning Tingling Hypersensitivity to touch or cold Examples Low back pain with radiculopathy Cervical radiculopathy Cancer pain Carpal tunnel syndrome Examples Pain due to inflammation Limb pain after a fracture Joint pain in osteoarthritis Post-operative visceral pain Common descriptors2 Aching Sharp Throbbing This slide illustrates three broad categories of pain: neuropathic (pathologic), nociceptive (physiologic), and mixed pain states that encompass both nociceptive and neuropathic components, with examples of common causes of each type of pain. The key talking points on this slide are as follows: Neuropathic pain has been defined by the International Association for the Study of Pain as ‘initiated or caused by a primary lesion or dysfunction in the nervous system’.1 Depending on where the lesion or dysfunction occurs within the nervous system, neuropathic pain can be peripheral or central in origin. Causes of peripheral neuropathic pain include postherpetic neuralgia (PHN) and diabetic peripheral neuropathy (DPN). Due to the prevalence and characteristics of PHN and DPN, these states may be considered representative of peripheral neuropathic pain. Nociceptive pain is an appropriate physiologic response that occurs when specific peripheral sensory neurons (nociceptors) respond to noxious stimuli. Nociceptive pain has a protective role because it elicits reflex and behavioral responses that keep tissue damage to a minimum. Acute pain, such as that seen with tissue inflammation and chronic pain, such that accompanying osteoarthritis, are examples of nociceptive pain. Although there are no specific descriptors for each type of pain, neuropathic pain is frequently described as ‘burning or tingling’ in quality, while nociceptive pain is often described as ‘aching or throbbing’. There are cases in which an individual experiences pain sensations that are a blend of pain having a nociceptive and a neuropathic origin. For example, in carpal tunnel syndrome, it is common experience to have nociceptive pain, felt around the wrist, and neuropathic pain, felt in the distribution territory of the median nerve (fingers). References International Association for the Study of Pain. IASP Pain Terminology. Raja et al. in Wall PD, Melzack R (Eds). Textbook of pain. 4th Ed. Edinburgh, UK: Harcourt Publishers Limited ;11-57 Additional key words: descriptor 1. International Association for the Study of Pain. IASP Pain Terminology. 2. Raja et al. in Wall PD, Melzack R (Eds). Textbook of pain. 4th Ed ;11-57
1. Nociceptive Pain. Pain caused by injury to body tissues (musculoskeletal, cutaneous or visceral)2. Mixed Pain. Pain with. neuropathic and. nociceptive. components. Examples. Peripheral. Post-herpetic neuralgia. Trigeminal neuralgia. Diabetic peripheral neuropathy. Post-surgical neuropathy. Post-traumatic neuropathy. Central. Post-stroke pain. Common descriptors2. Burning. Tingling. Hypersensitivity to touch or cold. Examples. Low back pain with radiculopathy. Cervical radiculopathy. Cancer pain. Carpal tunnel syndrome. Examples. Pain due to inflammation. Limb pain after a fracture. Joint pain in osteoarthritis. Post-operative visceral pain. Common descriptors2. Aching. Sharp. Throbbing. This slide illustrates three broad categories of pain: neuropathic (pathologic), nociceptive (physiologic), and mixed pain states that encompass both nociceptive and neuropathic components, with examples of common causes of each type of pain. The key talking points on this slide are as follows: Neuropathic pain has been defined by the International Association for the Study of Pain as ‘initiated or caused by a primary lesion or dysfunction in the nervous system’.1 Depending on where the lesion or dysfunction occurs within the nervous system, neuropathic pain can be peripheral or central in origin. Causes of peripheral neuropathic pain include postherpetic neuralgia (PHN) and diabetic peripheral neuropathy (DPN). Due to the prevalence and characteristics of PHN and DPN, these states may be considered representative of peripheral neuropathic pain. Nociceptive pain is an appropriate physiologic response that occurs when specific peripheral sensory neurons (nociceptors) respond to noxious stimuli. Nociceptive pain has a protective role because it elicits reflex and behavioral responses that keep tissue damage to a minimum. Acute pain, such as that seen with tissue inflammation and chronic pain, such that accompanying osteoarthritis, are examples of nociceptive pain. Although there are no specific descriptors for each type of pain, neuropathic pain is frequently described as ‘burning or tingling’ in quality, while nociceptive pain is often described as ‘aching or throbbing’. There are cases in which an individual experiences pain sensations that are a blend of pain having a nociceptive and a neuropathic origin. For example, in carpal tunnel syndrome, it is common experience to have nociceptive pain, felt around the wrist, and neuropathic pain, felt in the distribution territory of the median nerve (fingers). References. International Association for the Study of Pain. IASP Pain Terminology. Raja et al. in Wall PD, Melzack R (Eds). Textbook of pain. 4th Ed. Edinburgh, UK: Harcourt Publishers Limited ; Additional key words: descriptor. 1. International Association for the Study of Pain. IASP Pain Terminology. 2. Raja et al. in Wall PD, Melzack R (Eds). Textbook of pain. 4th Ed ;")
17
Pathophysiology of Neuropathic Pain
Peripheral mechanisms Peripheral Neuron hyperexcitability Central mechanisms Abnormal Discharges Loss of inhibitory controls NeP Central Neuron hyperexcitability (central sensitization)
")
18
MECHANISM OF NEUROPATHIC PAIN
I. PERIPHERAL MECHANISM 1. Ectopic discharge 2. Peripheral sensitization 3. Sensitization to catecholamine II CENTRAL MECHANISM 1. Central sensitization 2. loss of descending inhibition 3. Structural reorganization at posterior horn

19
Peripheral Mechanism (Ectopic Discharges)
Nerve lesion induces hyperactivity due to changes in ion channel function Perceived pain Nerve lesion Descending modulation Ascending input Nociceptive afferent fiber Spinal cord Ectopic discharges

20
Central Mechanism (Loss of Inhibitory Controls)
Loss of descending modulation causes exaggerated pain due to an imbalance between ascending and descending signals Exaggerated pain perception Noxious stimuli Loss of descending modulation Ascending input Nociceptive afferent fiber Spinal cord

21
Central Mechanism (Central Sensitization)
After nerve injury, increased input to the dorsal horn can induce central sensitization Perceived pain Nerve lesion Descending modulation Ascending input Nociceptive afferent fiber Perceived pain (allodynia) Abnormal discharges induce central sensitization Tactile stimuli Descending modulation Ascending input Intact tactile fiber
 Abnormal discharges induce central sensitization. Tactile stimuli. Descending modulation. Ascending input. Intact tactile fiber.")
22
Beberapa sindroma NP yang banyak ditemukan
A. Mononeuropati Sindroma yangn disebabkan kompresi saraf perifer atau radiks, seperti; radikulopati lumbar dan servikal Sindroma yang berhubungan dengan inflamasi saraf perifer; acute herpetic neuralgia Sindroma yang berhubungan dengan ischaemic/infark pada saraf perifer; neuropatik diabetika Painful mononeuropathy di daerah orofasial; trigeminal neuralgia Sindroma sehubungan dengan formasi neuroma; stump pain (nyeri puntung), nyeri paska mastektomi Causalgia (CRPS tipe II) B. Polyneuropati; misalnya dengan gejala burning feet. Berbagai keadaan seperti: defisiensi vitamin, DM, Chemoteraphy
, nyeri paska mastektomi. Causalgia (CRPS tipe II) B. Polyneuropati; misalnya dengan gejala burning feet. Berbagai keadaan seperti: defisiensi vitamin, DM, Chemoteraphy.")
23
Neurological deficits
MAIN CLINICAL FEATURES Positive symptoms Painful symptoms Spontaneous pain Allodynia Hyperalgesia Non-painful symptoms Paresthesia dysesthesia Negative symptoms Neurological deficits Sensory++ Motor cognitive

24
Gejala Nyeri Neuropatik
1. Stimulus – Independent Pain ( Gejala diutarakan oleh pasien ) seperti: Rasa terbakar kontinyu Nyeri seperti ditusuk, menyentak intermiten Nyeri seperti tersetrum Beberapa parestesia Sensasi abnormal yang tidak mengganggu Beberapa disestesia Sensasi abnormal yang mengganggu Baron, 2000; Woolf, 1999.
 seperti: Rasa terbakar kontinyu. Nyeri seperti ditusuk, menyentak intermiten. Nyeri seperti tersetrum. Beberapa parestesia. Sensasi abnormal yang tidak mengganggu. Beberapa disestesia. Sensasi abnormal yang mengganggu. Baron, 2000; Woolf,")
25
(Nyeri dibangkitkan pada pemeriksaan)
2. Stimulus evoked pain (Nyeri dibangkitkan pada pemeriksaan) Hiperalgesia Reaksi yang meningkat terhadap stimulus nyeri (noksius) Alodinia Nyeri akibat stimulus yang tidak nyeri (non- noksius/inocuous)
 Hiperalgesia. Reaksi yang meningkat terhadap stimulus nyeri (noksius) Alodinia. Nyeri akibat stimulus yang tidak nyeri (non- noksius/inocuous)")
26
ASESMEN DAN MESUREMENT NYERI NEUROPATIK

27
CLINICAL FEATURES OF NOCICEPTIVE PAIN
▪ Sudden onset. ▪ Quality: sharp, stabbing, pricking ▪ Localized. ▪ Self-limiting. ▪ Autonomic response: Palpitation, elevated blood pressure, sweating etc. ▪ Usually the cause is identifiable.

28
KARAKTERISTIK KLINIK NYERI NEUROPATIK
Umumnya menunjukkan gejala: Continuous burning pain Paroxysmal (electric shock-like) pain Allodynia Radiating dysesthesias Paresthesias Tanda-tanda umumnya: Sensory loss Weakness Autonomic changes
 pain. Allodynia. Radiating dysesthesias. Paresthesias. Tanda-tanda umumnya: Sensory loss. Weakness. Autonomic changes.")
29
DIAGNOSE Anamnese penyebab nyeri Pemeriksaan fisik neurologik
Pemeriksaan Khusus Alodinia Hiperalgesia

30
PEMERIKSAAN NYERI KHUSUS PADA ALODINIA
Jenis Alodinia Cara Periksa Respon Mekanis statis (serabut C) Tekanan ringan dengan benda tumpul Rasa nyeri tumpul (dull pain) Mekanis pungtat Beberapa tusukan ringan dengan jarum Rasa nyeri tajam superfisial Mekanisme dinamis (A ) Usapan ringan dengan kapas Rasa nyeri tajam terbakar, superfisial Mekanisme somatik dalam Tekanan ringan pada sendi Rasa nyeri yang dalam Termal panas Tabung air hangat 40oC Rasa seperti terbakar Termal dingin Tabung air dingin 20oC Rasa nyeri terbakar
 Tekanan ringan dengan benda tumpul. Rasa nyeri tumpul (dull pain) Mekanis pungtat. Beberapa tusukan ringan dengan jarum. Rasa nyeri tajam superfisial. Mekanisme dinamis (A ) Usapan ringan dengan kapas. Rasa nyeri tajam terbakar, superfisial. Mekanisme somatik dalam. Tekanan ringan pada sendi. Rasa nyeri yang dalam. Termal panas. Tabung air hangat 40oC. Rasa seperti terbakar. Termal dingin. Tabung air dingin 20oC. Rasa nyeri terbakar.")
31
PEMERIKSAAN NYERI KHUSUS PADA HIPERALGESIA
Jenis Hiperalgesia Cara Periksa Respon Mekanisme tusukan Tusukan dengan jarum Rasa nyeri tajam superfisial Termal dingin Kontak dengan pendingin (aseton, alkohol) Rasa nyeri terbakar Termal panas Kontak dengan tabung air hangat 40oC
 Rasa nyeri terbakar. Termal panas. Kontak dengan tabung air hangat 40oC.")
32
Freezing, like the feet are on ice, although they feel warm to touch
Burning, feeling like the feet are on fire Stabbing, like sharp knives Modified by Meliala 2006 Lancinating, like electric shocks

33
Pain assessment scales
Verbal pain intensity scale No Mild Moderate Severe Very Worst pain pain pain pain severe possible pain pain Visual analog scale The slide depicts four of the pain scales that are used to assess a patient’s pain. The scales are considered simple for patients to use as well as being valid methods for measuring the severity of pain.1 These scales can be used at the patient’s bedside, and patients can be asked to respond to either a spoken or written question. With some scales, especially the visual analog scale, the patient marks the line at the point that best indicates the pain’s intensity. The Wong-Baker FACES Pain Rating Scale is validated and recommended for patients aged 3 years and older. On this scale, Face 0 indicates no pain an all, Face 1 feels mild pain, Face 2 feels moderate pain, Face 3 feels severe pain, Face 4 feels very severe pain, and Face 5 feels the worst possible pain. The original appears above, and can be used as is or with the brief word descriptions under each number. In a study of 148 children aged 4 to 5 years, there were no differences in pain scores when children used the original or brief word instructions.2 1. Portenoy RK, Kanner RM. Definition and Assessment of Pain. In: Portenoy RK, Kanner RM, eds. Pain Management: Theory and Practice. Philadelphia, Pa: FA Davis Company; 1996:8- 10. 2. Wong DL. Waley and Wong’s Essentials of Pediatric Nursing 5th ed. Mosby, Inc : 3. McCaffery M, Pasero C. Pain: Clinical Manual. Mosby, Inc. 1999:16. No pain Worst possible pain Portenoy RK, Kanner RM, eds. Pain Management: Theory and Practice :8-10. Wong DL. Waley and Wong’s Essentials of Pediatric Nursing 5th ed. 1997: McCaffery M, Pasero C. Pain: Clinical Manual. Mosby, Inc. 1999:16.

34
Pain assessment scales
0–10 Numeric pain intensity scale No Moderate Worst pain pain possible pain “Faces” scale The slide depicts four of the pain scales that are used to assess a patient’s pain. The scales are considered simple for patients to use as well as being valid methods for measuring the severity of pain.1 These scales can be used at the patient’s bedside, and patients can be asked to respond to either a spoken or written question. With some scales, especially the visual analog scale, the patient marks the line at the point that best indicates the pain’s intensity. The Wong-Baker FACES Pain Rating Scale is validated and recommended for patients aged 3 years and older. On this scale, Face 0 indicates no pain an all, Face 1 feels mild pain, Face 2 feels moderate pain, Face 3 feels severe pain, Face 4 feels very severe pain, and Face 5 feels the worst possible pain. The original appears above, and can be used as is or with the brief word descriptions under each number. In a study of 148 children aged 4 to 5 years, there were no differences in pain scores when children used the original or brief word instructions.2 1. Portenoy RK, Kanner RM. Definition and Assessment of Pain. In: Portenoy RK, Kanner RM, eds. Pain Management: Theory and Practice. Philadelphia, Pa: FA Davis Company; 1996:8- 10. 2. Wong DL. Waley and Wong’s Essentials of Pediatric Nursing 5th ed. Mosby, Inc : 3. McCaffery M, Pasero C. Pain: Clinical Manual. Mosby, Inc. 1999:16. Portenoy RK, Kanner RM, eds. Pain Management: Theory and Practice :8-10. Wong DL. Waley and Wong’s Essentials of Pediatric Nursing 5th ed. 1997: McCaffery M, Pasero C. Pain: Clinical Manual. Mosby, Inc. 1999:16.

35
PENATALAKSANAAN NYERI NEUROPATIK
Tujuan : Meningkatkan kualitas hidup pasien dengan melakukan pendekatan secara holistik, berupa pengobatan terhadap pain triad, yaitu nyeri, gangguan tidur dan gangguan mood ( ansietas, depresi dan obsesi konvulsi ) yang dilakukan oleh tim multidisiplin. Konsensus Nasional Diagnostik & Penatalaksanaan Nyeri Neuropatik, Pokdi Nyeri PERDOSSI, 2011
 yang dilakukan oleh tim multidisiplin. Konsensus Nasional Diagnostik & Penatalaksanaan Nyeri Neuropatik, Pokdi Nyeri PERDOSSI, 2011")
36
Successful Management of Neuropathic Pain has a Positive Impact for The Patient
Treatment of underlying conditions and symptoms Diagnosis Improved Quality of Sleep Improved Overall Quality of Life Improved Physical Functioning Improved Psychological State Reduced pain

37
BRAIN MECHANISTIC APPROACH TO TREATMENT Tx Central Sensitization Lesi
Beydoun, 2002 TCAs SSRIs SNRIs Tramadol Opiates Descending Inhibitors NE/5HT Opiate receptors Tx Lesi Central Sensitization Ca++ : Pregabalin, GBP,OXC,LTG,LVT NMDA : Ketamine, TPM Dextromethorphan Methadone Peripheral Sensitization Tx SPINAL CORD PNS Na+ CBZ OXC PHT TCA TPM LTG Mexiletine Lidocaine Tx Others Capsaicin NSAIDs Cox inhibitors Levodopa

38
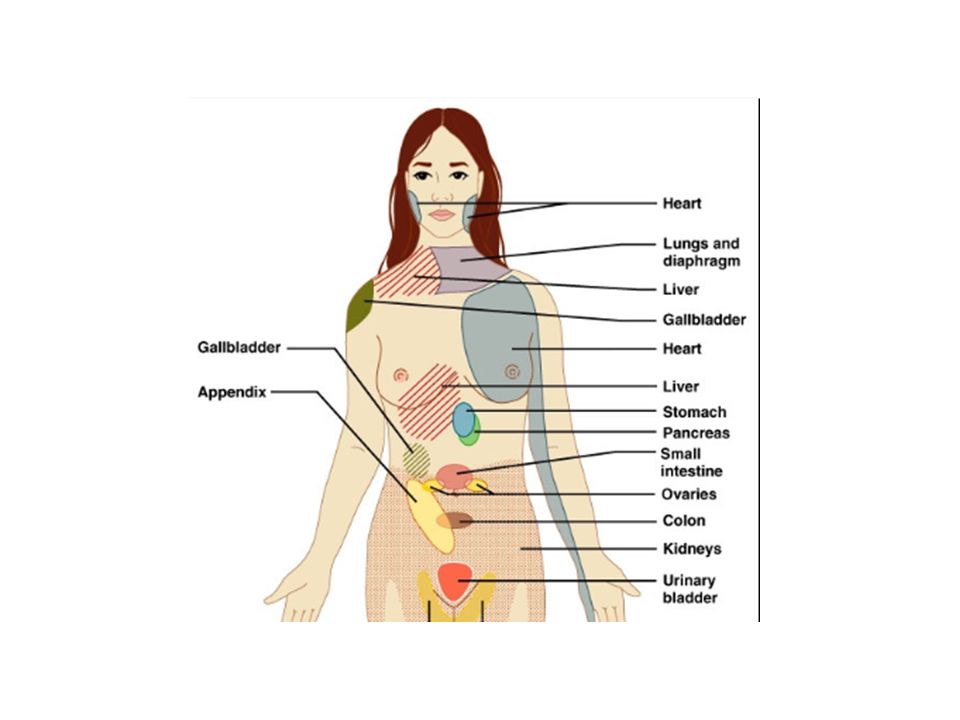
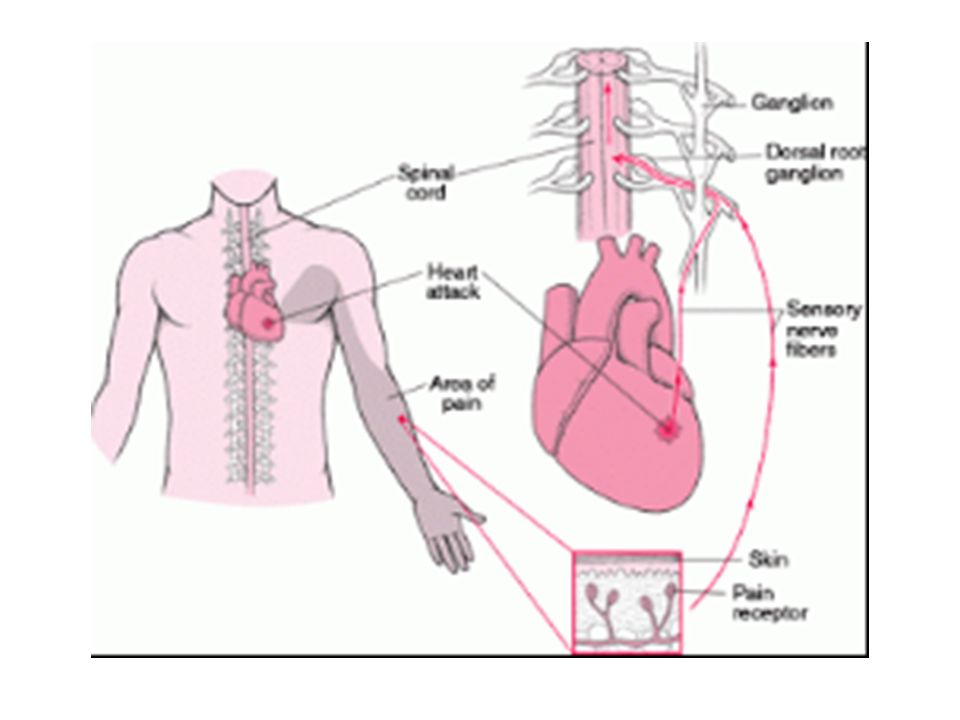
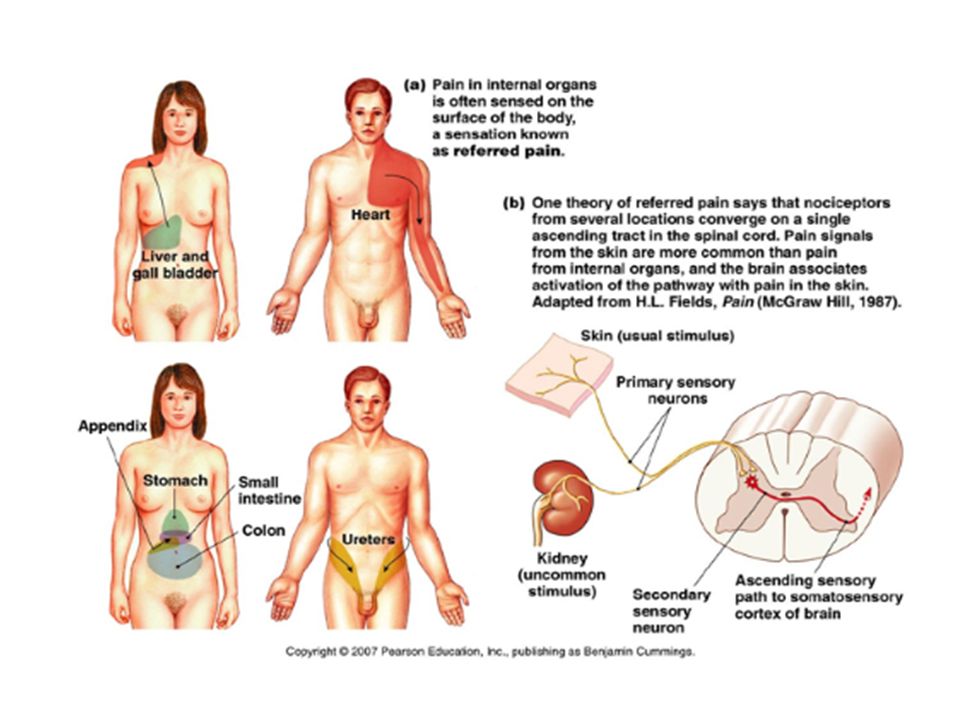
Referred Pain

39
Referred Pain Reflective pain : nyeri yang dirasakan pada lokasi yang berada jauh dari sumber nyerinya. Penyebab timbulnya referred pain ini sering disebabkan oleh adanya rangsangan pada organ organ visceral (organ dalam).
.")
41
CLINICAL PAIN PHYSIOLOGIC PAIN /
Classification: PAIN CLINICAL PAIN PHYSIOLOGIC PAIN / TRANSIENT PAIN Nociceptive Psychogenic Neuropathic (inflammatory) Somatic Visceral Peripheral Central Superficial Symphatic Deep • Acute : < 3-6 months, mostly nociceptive • Chronic : > 3-6 months, mostly neuropathic
 Somatic Visceral Peripheral Central. Superficial Symphatic. Deep. • Acute : < 3-6 months, mostly nociceptive. • Chronic : > 3-6 months, mostly neuropathic.")
42
Nociceptive Pain : Somatic Pain is the variety of nociceptive pain mediated by somatosensory afferent fibers. It is usually easly localizable and of sharp, aching or throbbing quality. Post operative, traumatic and local inflammatory pain are often of this variety. Visceral Pain is harder to localize, (e.q headache in meningitis, biliary colic, gastritis, mesenteric infarction) may be dull, cramplike, piercing or waxing and waning. It is mediated peripherally by C fibers, and centrally by spinal cord pathways terminating mainly in the limbic system.
 may be dull, cramplike, piercing or waxing and waning. It is mediated peripherally by C fibers, and centrally by spinal cord pathways terminating mainly in the limbic system.")
43
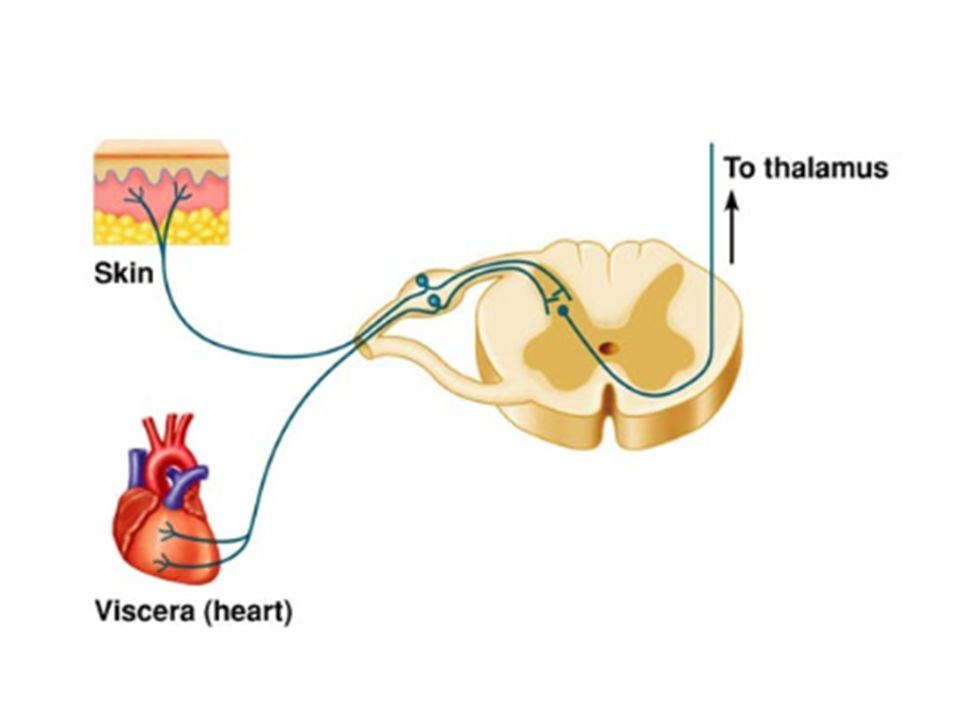
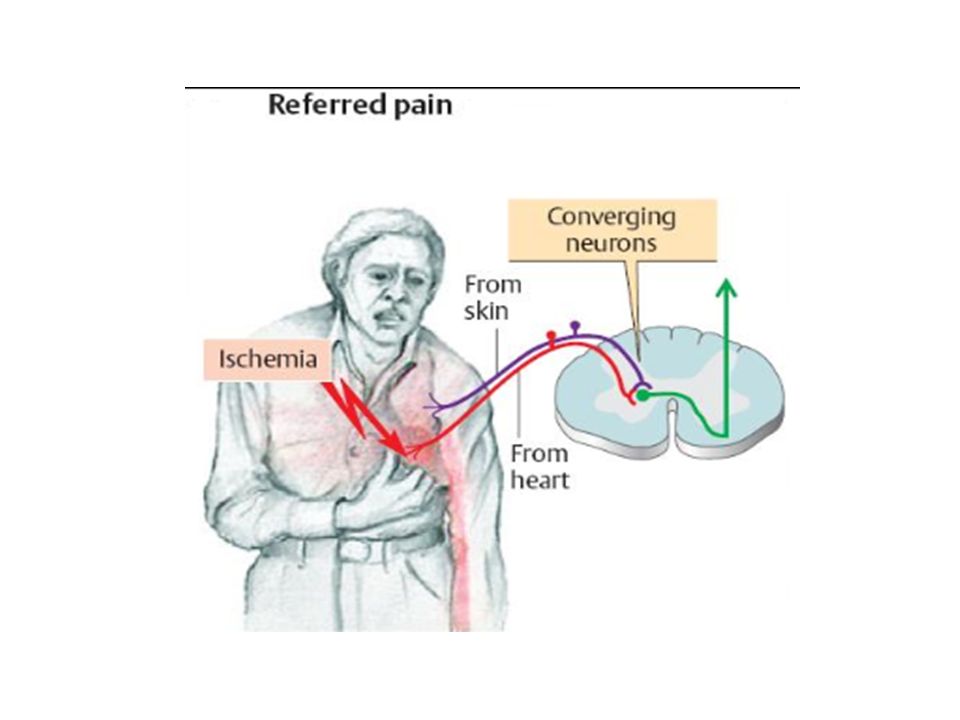
Visceral pain is not felt in its site origin (internal organ where it originates )or but is rather referred to a cutaneus zone (of head) specific to that organ. This phenomenon is explained by the arrival of sensory impulses from both the internal organ and its related zone of head at the posterior horn at the same level of the spinal cord. The brain thus (mis)interprets the visceral pain as originating in the related cutaneous zone.
interprets the visceral pain as originating in the related cutaneous zone.")
44
The pain may be describes as burning, pulling, pressure or soreness and there may be cutaneous hyperesthesia to light touch. In addition to the zones of head , referred pain may also be felt in muscles and connective tissue (pressure point, or mc Burney’s point)
.")
45
Mechanisms acute visceral Pain
Visceral sensory reseptors : Receptors responsible for the sensations of visceral pain are the same population of visceral receptors responding to innocuous stimuli and responsible for visceral reflex actions. This receptors would respond to noxious stimuli with higher frequencies of firing Receptors responsible for the sensations of visceral pain are a different population of visceral receptors which respond to the same stimuli that evoke visceral reflex actions but with different thresholds or by different mechanisms. This view postulates the existence of specific visceral nociceptors. Visceral nociceptors

51
One possible trigger for the sensation of visceral pain could be the sensitization of visceral nociceptors. According to this interpretation visceral nociceptors, which normally have a relatively high threshold and respond only to intense forms of stimulation, become abnormally sensitive by decreasing their threshold for activation thus responding to mild form stimulation.

52
Existence of silent nociceptors :
‘Silent’ nociceptors : normally unresponsive to physiological forms of stimulation but being able to respon to mild stimuli when the tissue suffers persistent damage Existence of silent nociceptors : Joints Colon Urinary bladder : in normal state could not be activated. But that became responsive to bladder distension and contraction following to inflammation.

53
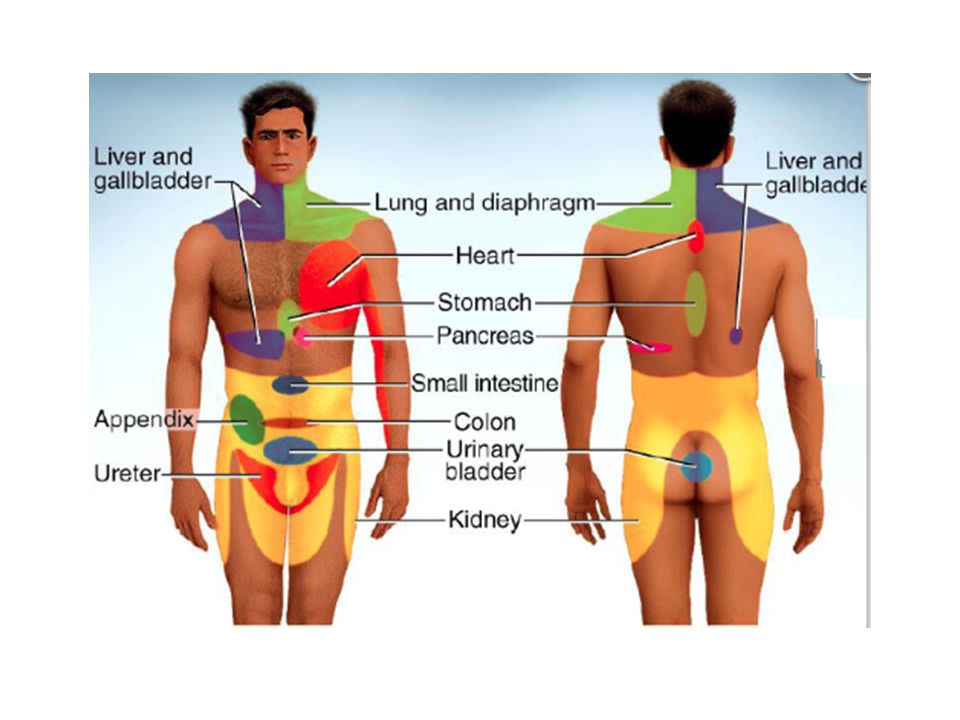
Common examples of referred pain
Shoulder Pain : this can caused by a disorders in the liver, gastric ulcer, gallstone, pericarditis, pneumonia or rupture of the spleen. Ice Cream Headache : also known as ‘brain freeze’ this is cuased by the vagus nerve being cooled when the throat is cooled by eating something cold, such as ice cream.

54
Common examples of referred pain
Appendicitis pain : sometimes people with acute appendicitis feel the pain in the right shoulder and not in the abdomen Pain in a Phantom Limb : a pain sensation felt from a limb that is no longer there or from which no physical signals are sent. This type is very common in people with amputated limbs and quadriplegics.

55
SELESAI

Presentasi serupa








 Fusiform (parallel)>")
 Suzy Rahardja.>")









