Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
Telaah Laporan Proyek Divisi Mutu & Divisi RS 30 April 2015 PKMK FK UGM

2
PKMK & MMR FK UGM. (2008). Quality Improvement of TB Care in Hospital after Clinical Audit Finding: An Action Research. Objective: to improve the quality of TB clinical care in hospitals. Design: Intervention case study (pretest-posttest without control cases). oxooxo
. oxooxo.")
3
Setting: Persahabatan Hospital (public, teaching hospital, Jakarta) and Bethesda Hospital (private hospital, Jogjakarta). Subjects: Managers (director, vice director of medical care, medical committee staff, adminitrators, medical records staff, support staff) and operating core (doctors, nurses).
 and operating core (doctors, nurses)..")
4
Method: Pretest (O): Retrospective audit of TB clinical care conducted during 2007 in eight hospitals and pulmonology clinics in Jakarta, West Java, Yogyakarta, Central Java and East Java. Of these eight institutions two hospitals were selected for intervention.

5
Intervention (X): 1. Setting up a quality management system – preparatory meeting to secure commitment and participation; 2. Two-day workshop to identify quality improvement activities and tools (clinical guidelines, clinical pathways, audit forms, checklists); and, 3. Four-month implementation of quality improvement.
; and, 3. Four-month implementation of quality improvement..")
6
Posttest (O): Retrospective audit of TB clinical care in the two intervention hospitals – 43 cases (11 paediatrics and 32 adult) of the Bethesda Hospital and 33 cases (5 paediatrics and 28 adult) of the Persahabatan Hospital Main Outcome Measures: TB clinical care deficiencies. Main Results: Considerable decrease in deficiencies (See Table 3).
..")
7
Conclusion: The high number of deficiensies identified in the first audit (and, therefore, the substantial decrease in deficiencies in the second audit) can be explained by the failure of doctors to record performance in the medical records and TB clinical care forms. Corrective actions subsequent to the first clinical audit in the two intervention hospitals consisted of development of clinical pathways forms, followed by pilot testing, socialization and training.

8
Not all operating core members were happy with the clinical pathways forms. The decision to adopt clinical audit/clinical pathways was not made with sufficient participation of the operating core and not fully integrated with other quality improvement programs (e.g., hospital accreditation, ISO).
..")
9
Commentary: A systematic review by Jamtvedt et al. (2008) of 118 RCT reports on the effectiveness of audit and feedback in improving professional practice concluded that the effects are small and that greater effects are achieved when baseline compliance is low and when feedback is strong.
 of 118 RCT reports on the effectiveness of audit and feedback in improving professional practice concluded that the effects are small and that greater effects are achieved when baseline compliance is low and when feedback is strong..")
10
The substantial decrease of TB clinical care deficiencies in the two intervention hospitals cannot be attributed to the quality improvement program introduced by the PKMK/MMR UGM team. The shift in deficiencies were mainly caused by lack of recording and many confounding variables cannot be controled by a simple pretest-postest design.

11
x 1 o -------- x 0 o A more meaningful examination of the intervention efficacy can be conducted by selecting matched control hospitals and to train both the intervention and control hospitals in how to conduct retrospective clinical audits

12
Deviations from audit criteria cannot be right away regarded as deficiencies. Professionals have justified exceptions and the audit criteria need constant updating. This can be facilitated by introducing EBP (Evidence-Based Practice) - to train professionals in how to use valid empirical research results and to establish a unit that brings up to date better diagnostic and therapeutic methods.
 - to train professionals in how to use valid empirical research results and to establish a unit that brings up to date better diagnostic and therapeutic methods..")
13
Nih Luh Putu Eka Andayani, Yos Hendra, Heru Aryadi, dan Yvonne Palijama. (2014). Laporan Akhir Pendampingan Penyusunan Regulasi Implementasi BLUD – Rancangan Peraturan Bupati Belitung Timur terkait BLUD RSUD. Pusat Kebijakan & Manajemen Kesehatan, FK UGM.
. Laporan Akhir Pendampingan Penyusunan Regulasi Implementasi BLUD – Rancangan Peraturan Bupati Belitung Timur terkait BLUD RSUD. Pusat Kebijakan & Manajemen Kesehatan, FK UGM..")
14
Tujuan: mendampingi Pokja RSUD Belitung Timur menyusun draft beberapa Peraturan Kepala Daerah untuk implementasi BLUD (i.e., Kebijakan keuangan BLUD, Pengadaan barang dan jasa, Pengangkatan pegawai non-PNS, dan Remunerasi) dan melakukan sosialisasi-advokasi kepada PemDa dan DPRD Belitung Timur. Rancangan: Laporan kasus. Tempat & waktu: Belitung Timur, Oktober – Desember 2014. Subyek: Pokja RSUD.

15
Metoda: Tiga kali kunjungan untuk mendampingi Pokja menyusun draft Rancangan Peraturan Bupati, konsultasi draft dengan Biro Hukum PemDa, merevisi draft dan menyusun sistem penilaian kinerja & sistem remunerasi, dan diskusi dengan Komisi III DPRD tentang legislasi dan penganggaran BLUD.

16
Ukuran keberhasilan Kegiatan: Pengesahan Rancangan Peraturan Bupati Belitung Timur terkait BLUD RSUD oleh Bupati dan penganggaran kepada Satuan Kerja perangkat Daerah (SKPD) yang menerapkan Pola Pengelolaan Keuangan (PPK) BLUD.
 yang menerapkan Pola Pengelolaan Keuangan (PPK) BLUD.")
17
Hasil Kegiatan: Rancangan Peraturan Bupati Belitung Timur terkait BLUD RSUD. Kesimpulan: Tim konsultan berhasil mendampingi Pokja RSUD Belitung Timur dalam hal menyusun dan melakukan sosialisasi-advokasi draft Rancangan Peraturan Bupati dengan PemDa dan DPRD.

18
Tanggapan: Inti dari kebijakan keuangan BLUD adalah flexibiltas pengelolaan keuangan, yang mencakup flexibilitas dalam hal pengumpulan, penghimpunan dan penggunaan keuangan. Keberhasilan memanfaatkan flexibiltas ini selain tergantung dari pengesahan peraturan oleh PemDa dan DPRD juga sangat tergantung dari kemampuan dan motivasi anggota organisasi untuk melaksanakan peraturan tsb.

19
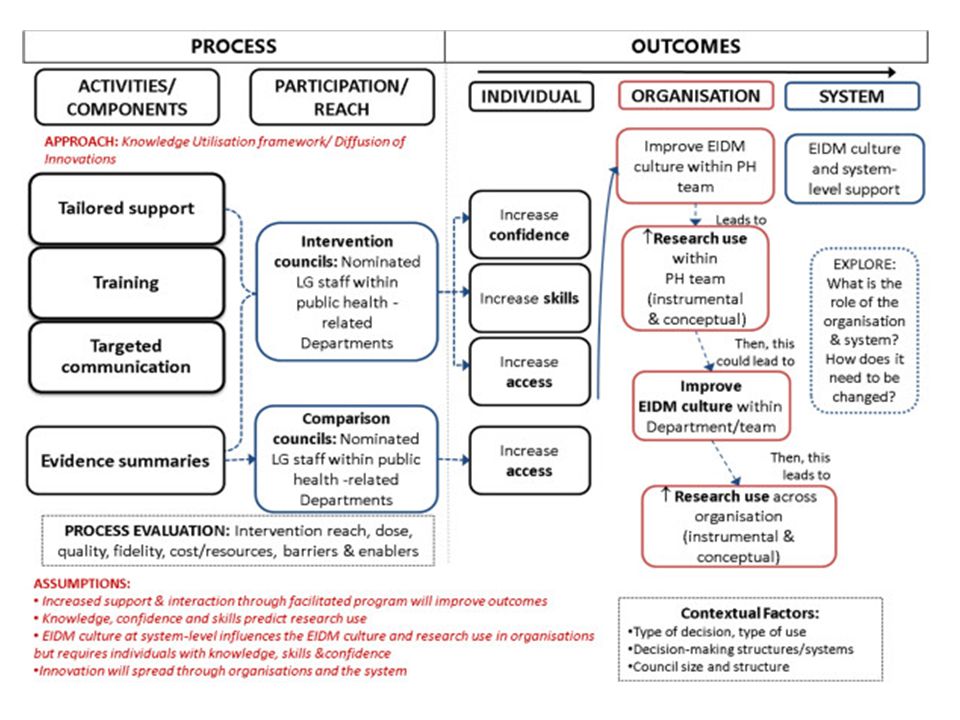
Berbagai intervensi harus dirancang dan dilaksanakan oleh anggota organisasi RSUD supaya berhasil mengelola keuangan dan meningkatkan mutu dan cakupan pelayanan kesehatan. Untuk itu mereka perlu dilatih menggunakan informasi tentang intervensi- intervensi yang terbukti berdayaguna. Team konsultan PKMK dapat memengikuti Logic Model for Knowledge Translation for local Governments dari Amstrong, R., dkk. (2013) berikut, yang digunakan ketika mendampingi suatu PemDa di Australia dalam membuat keputusan tentang berbagai intervensi kesehatan masyarakat:
 berikut, yang digunakan ketika mendampingi suatu PemDa di Australia dalam membuat keputusan tentang berbagai intervensi kesehatan masyarakat:.")
Presentasi serupa


>")





 dan Pembelajaran Konvensional.>")










