Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
BY. NUR ASNAH SITOHANG,S.Kep.Ns.M.Kep BY. NUR ASNAH SITOHANG,S.Kep.Ns.M.Kep

2
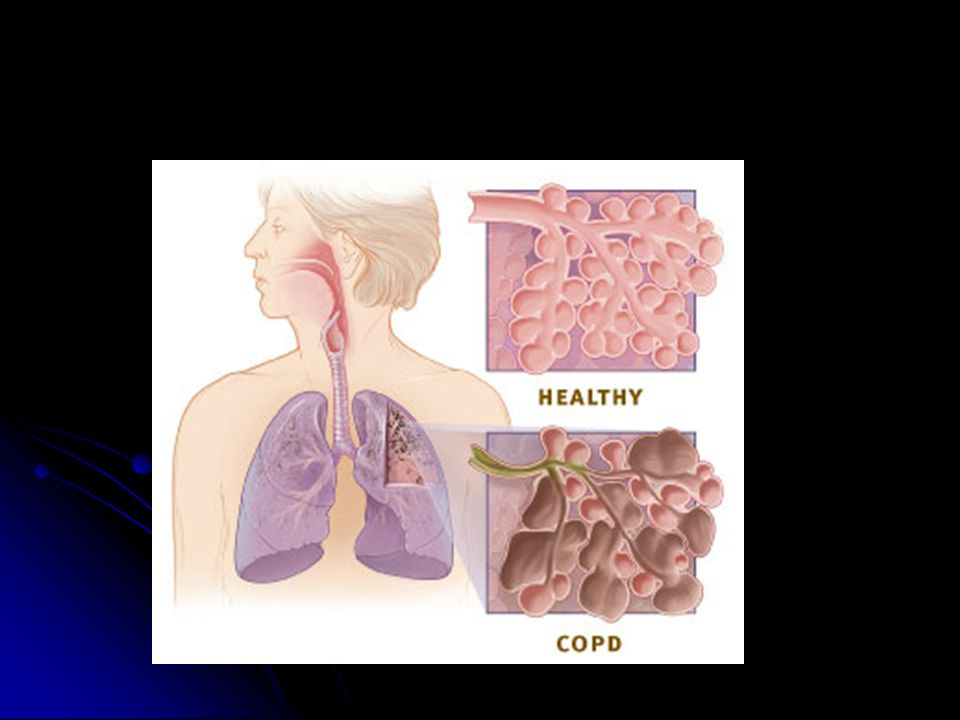
DEFENISI is a progressive disease that makes it hard to breathe. "Progressive" means the disease gets worse over time. is a progressive disease that makes it hard to breathe. "Progressive" means the disease gets worse over time.

3
To understand COPD, it helps to understand how the lungs work. The air that you breathe goes down your windpipe into tubes in your lungs called bronchial tubes, or airways. To understand COPD, it helps to understand how the lungs work. The air that you breathe goes down your windpipe into tubes in your lungs called bronchial tubes, or airways.how the lungs workhow the lungs work The airways are shaped like an upside-down tree with many branches. At the end of the branches are tiny air sacs called alveoli The airways are shaped like an upside-down tree with many branches. At the end of the branches are tiny air sacs called alveoli

4
The airways and air sacs are elastic. When you breathe in, each air sac fills up with air like a small balloon. When you breathe out, the air sac deflates and the air goes out. The airways and air sacs are elastic. When you breathe in, each air sac fills up with air like a small balloon. When you breathe out, the air sac deflates and the air goes out.

5
In COPD, less air flows in and out of the airways because of one or more of the following: In COPD, less air flows in and out of the airways because of one or more of the following: The airways and air sacs lose their elastic quality. The airways and air sacs lose their elastic quality. The walls between many of the air sacs are destroyed. The walls between many of the air sacs are destroyed. The walls of the airways become thick and inflamed (swollen). The walls of the airways become thick and inflamed (swollen). The airways make more mucus than usual, which tends to clog the airways. The airways make more mucus than usual, which tends to clog the airways.
. The walls of the airways become thick and inflamed (swollen). The airways make more mucus than usual, which tends to clog the airways. The airways make more mucus than usual, which tends to clog the airways..")
9
In the United States, the term "COPD" includes two main conditions—emphysema and chronic obstructive bronchitis. In the United States, the term "COPD" includes two main conditions—emphysema and chronic obstructive bronchitis.emphysema In emphysema, the walls between many of the air sacs are damaged, causing them to lose their shape and become floppy. This damage also can destroy the walls of the air sacs, leading to fewer and larger air sacs instead of many tiny ones. In emphysema, the walls between many of the air sacs are damaged, causing them to lose their shape and become floppy. This damage also can destroy the walls of the air sacs, leading to fewer and larger air sacs instead of many tiny ones.

10
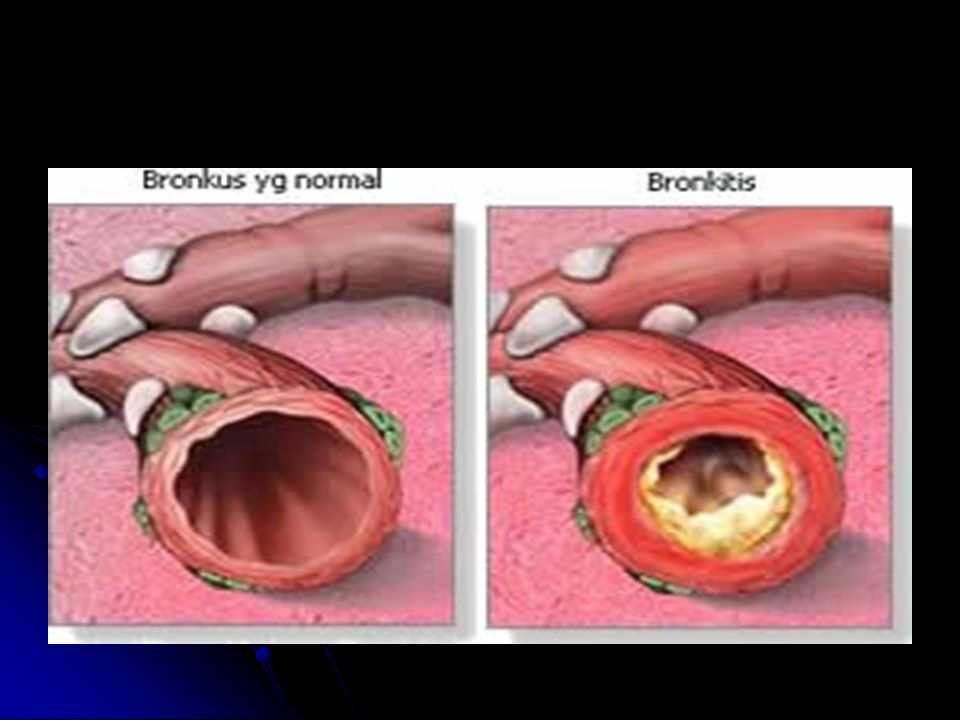
In chronic obstructive bronchitis, the lining of the airways is constantly irritated and inflamed. This causes the lining to thicken. Lots of thick mucus forms in the airways, making it hard to breathe. In chronic obstructive bronchitis, the lining of the airways is constantly irritated and inflamed. This causes the lining to thicken. Lots of thick mucus forms in the airways, making it hard to breathe. Most people who have COPD have both emphysema and chronic obstructive bronchitis. Thus, the general term "COPD" is more accurate. Most people who have COPD have both emphysema and chronic obstructive bronchitis. Thus, the general term "COPD" is more accurate.

11
COPD is a major cause of disability, and it's the fourth leading cause of death in the United States. More than 12 million people are currently diagnosed with COPD. An additional 12 million likely have the disease and don't even know it. COPD is a major cause of disability, and it's the fourth leading cause of death in the United States. More than 12 million people are currently diagnosed with COPD. An additional 12 million likely have the disease and don't even know it. COPD develops slowly. Symptoms often worsen over time and can limit your ability to do routine activities. Severe COPD may prevent you from doing even basic activities like walking, cooking, or taking care of yourself. COPD develops slowly. Symptoms often worsen over time and can limit your ability to do routine activities. Severe COPD may prevent you from doing even basic activities like walking, cooking, or taking care of yourself.

12
Most of the time, COPD is diagnosed in middle-aged or older people. The disease isn't passed from person to person—you can't catch it from someone else. Most of the time, COPD is diagnosed in middle-aged or older people. The disease isn't passed from person to person—you can't catch it from someone else.

13
Other Names for COPD Chronic obstructive airway disease Chronic obstructive airway disease Chronic obstructive bronchitis Chronic obstructive bronchitis Chronic obstructive lung disease Chronic obstructive lung disease Emphysema Emphysema Emphysema

15
What Causes COPD? Most cases of COPD develop after long-term exposure to lung irritants that damage the lungs and the airways. Most cases of COPD develop after long-term exposure to lung irritants that damage the lungs and the airways. In the United States, the most common irritant that causes COPD is cigarette smoke. Pipe, cigar, and other types of tobacco smoke also can cause COPD, especially if the smoke is inhaled. Secondhand smoke—that is, smoke in the air from other people smoking—also can irritate the lungs and contribute to COPD. In the United States, the most common irritant that causes COPD is cigarette smoke. Pipe, cigar, and other types of tobacco smoke also can cause COPD, especially if the smoke is inhaled. Secondhand smoke—that is, smoke in the air from other people smoking—also can irritate the lungs and contribute to COPD. Breathing in air pollution and chemical fumes or dust from the environment or workplace also can contribute to COPD. Breathing in air pollution and chemical fumes or dust from the environment or workplace also can contribute to COPD.

16
In rare cases, a genetic condition called alpha-1 antitrypsin deficiency may play a role in causing COPD. People who have this condition have low levels of alpha-1 antitrypsin (AAT)—a protein made in the liver. In rare cases, a genetic condition called alpha-1 antitrypsin deficiency may play a role in causing COPD. People who have this condition have low levels of alpha-1 antitrypsin (AAT)—a protein made in the liver.alpha-1 antitrypsin deficiencyalpha-1 antitrypsin deficiency Having a low level of the AAT protein can lead to lung damage and COPD if you're exposed to smoke or other lung irritants. If you have this condition and smoke, COPD can worsen very quickly Having a low level of the AAT protein can lead to lung damage and COPD if you're exposed to smoke or other lung irritants. If you have this condition and smoke, COPD can worsen very quickly
—a protein made in the liver. In rare cases, a genetic condition called alpha-1 antitrypsin deficiency may play a role in causing COPD. People who have this condition have low levels of alpha-1 antitrypsin (AAT)—a protein made in the liver.alpha-1 antitrypsin deficiencyalpha-1 antitrypsin deficiency Having a low level of the AAT protein can lead to lung damage and COPD if you re exposed to smoke or other lung irritants. If you have this condition and smoke, COPD can worsen very quickly Having a low level of the AAT protein can lead to lung damage and COPD if you re exposed to smoke or other lung irritants. If you have this condition and smoke, COPD can worsen very quickly.")
17
Who Is At Risk for COPD? The main risk factor for COPD is smoking The main risk factor for COPD is smoking People who have a family history of COPD are more likely to get the disease if they smoke. People who have a family history of COPD are more likely to get the disease if they smoke. Long-term exposure to other lung irritants also is a risk factor for COPD Long-term exposure to other lung irritants also is a risk factor for COPD a genetic condition a genetic condition

18
What Are the Signs and Symptoms of COPD? The signs and symptoms of COPD include: The signs and symptoms of COPD include: An ongoing cough or a cough that produces large amounts of mucus (often called "smoker's cough") An ongoing cough or a cough that produces large amounts of mucus (often called "smoker's cough") Shortness of breath, especially with physical activity Shortness of breath, especially with physical activity Wheezing (a whistling or squeaky sound when you breathe) Wheezing (a whistling or squeaky sound when you breathe) Chest tightness Chest tightness
 An ongoing cough or a cough that produces large amounts of mucus (often called smoker s cough ) Shortness of breath, especially with physical activity Shortness of breath, especially with physical activity Wheezing (a whistling or squeaky sound when you breathe) Wheezing (a whistling or squeaky sound when you breathe) Chest tightness Chest tightness.")
19
How Is COPD Diagnosed? Lung Function Test :spirometry Lung Function Test :spirometry

20
A chest x ray or chest computed tomography (CT) scan A chest x ray or chest computed tomography (CT) scanchest x raychest computed tomography (CT) scanchest x raychest computed tomography (CT) scan
 scan A chest x ray or chest computed tomography (CT) scanchest x raychest computed tomography (CT) scanchest x raychest computed tomography (CT) scan")
21
Arterial blood gases : should be performed in all patients with an FEV1 less than 40% predicted or when clinical signs of respiratory failure/ rigth –sided heart failure are present Arterial blood gases : should be performed in all patients with an FEV1 less than 40% predicted or when clinical signs of respiratory failure/ rigth –sided heart failure are present

22
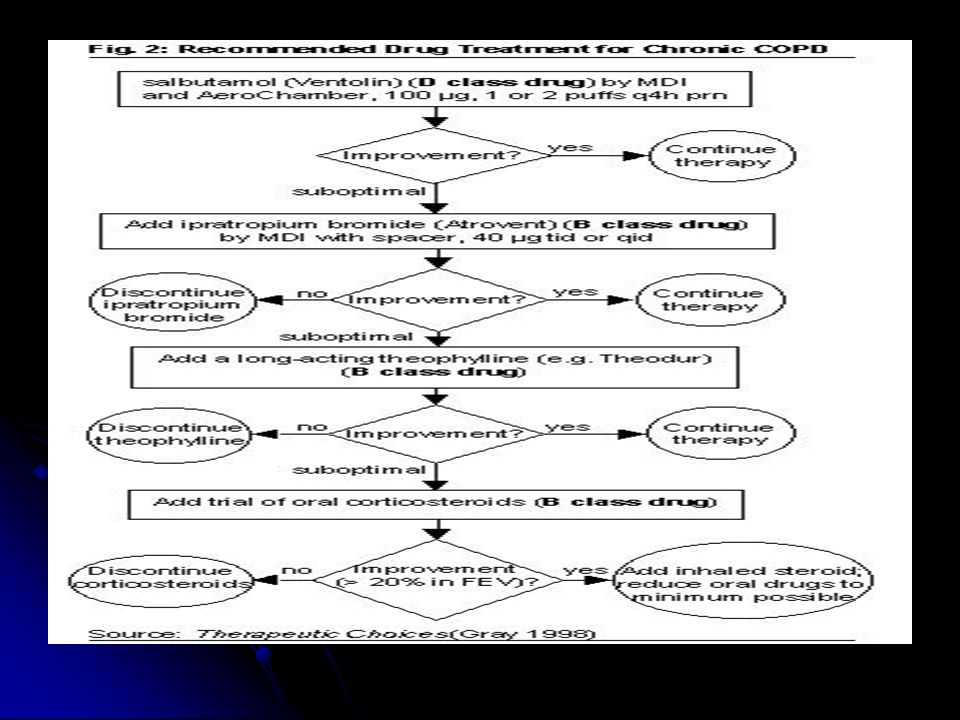
How Is COPD Treated? Quitting smoking Quitting smoking Other treatments for COPD may include medicines, vaccines, pulmonary rehabilitation (rehab), oxygen therapy, surgery, and managing complications. Other treatments for COPD may include medicines, vaccines, pulmonary rehabilitation (rehab), oxygen therapy, surgery, and managing complications.
, oxygen therapy, surgery, and managing complications. Other treatments for COPD may include medicines, vaccines, pulmonary rehabilitation (rehab), oxygen therapy, surgery, and managing complications..")
24
The goals of COPD treatment Relieve your symptoms Relieve your symptoms Slow the progress of the disease Slow the progress of the disease Improve your exercise tolerance (your ability to stay active) Improve your exercise tolerance (your ability to stay active) Prevent and treat complications Prevent and treat complications Improve your overall health Improve your overall health
 Improve your exercise tolerance (your ability to stay active) Prevent and treat complications Prevent and treat complications Improve your overall health Improve your overall health")
25
Stage of COPD and their treatment Stagecharacteristics Recommended treatment all o avoidance of risk factor o influenza factor 0: at risk chronic symptoms chronic symptoms Exposure to risk factor Exposure to risk factor Normal spyrometry Normal spyrometry Short acting bronchodilator when needed

26
1.Mild COPD - FEV1/FVC <70% - FEV,>80% predicted - With or without symptom -short acting bronchodilator when needed 2. Moderate COPD II A - FEV1/FVC <70% - FEV,<80% predicted - With or without symptom Regular treatmen with one/more bronchodilator - Rehabilitation - Inhaled glucocorticoster oid if significant symptom & lung function respon

27
IIB - FEV1/FVC <70% - 30% FEV,<50% predicted - With or without symptom -Regular treatmen with one/more bronchodilator - Rehabilitation - Inhaled glucocorticoster oid if significant symptom & lung function respon/if repeated exacerbation

28
III. Severe COPD - FEV1/FVC <70% - 30% FEV,predicted or presence of respiratory failure or right heart filure - Idem stage II + ; - treatment of complications - rehabilitation - long term O2 therapy if respiratory failure - consider surgical treatment

29
The 2001 GOLD gudelines for diagnosis,management & prevention COPD Nonpharmacological therapy : Nonpharmacological therapy : 1. Exercise training 2. Nutritional counseling 3. Education

30
Pharmacilogical therapy ; Pharmacilogical therapy ; 1. Bronchodilators 2. Glucocorticoids 3. Other pharmacological agents 4. O2 therapy 5. Surgical therapy

31
How Can COPD Be Prevented? you can take steps to prevent complications and slow the progress of the disease. you can take steps to prevent complications and slow the progress of the disease.

32
Living With COPD Avoid lung irritants Avoid lung irritants Get ongoing care Get ongoing care Manage the disease and its symptoms Manage the disease and its symptoms Prepare for emergencies Prepare for emergencies

33
Pengkajian Sudah berapa lama pasien mengalami kesulitan pernapasan? Sudah berapa lama pasien mengalami kesulitan pernapasan? Apakah aktivitas meningkatkan dispnea? Apakah aktivitas meningkatkan dispnea? Berapa jauh batasan pasien terhadap toleransi aktivitas? Berapa jauh batasan pasien terhadap toleransi aktivitas? Kapan pasien mengeluh paling letih dan sesak napas? Kapan pasien mengeluh paling letih dan sesak napas?

34
Apakah kebiasaan makan dan tidur terpengaruh? Apakah kebiasaan makan dan tidur terpengaruh? Riwayat merokok? Riwayat merokok? Obat yang dipakai setiap hari? Obat yang dipakai setiap hari? Obat yang dipakai pada serangan akut? Obat yang dipakai pada serangan akut? Apa yang diketahui pasien tentang kondisi dan penyakitnya? Apa yang diketahui pasien tentang kondisi dan penyakitnya?

35
Data tambahan yang dikumpulkan melalui observasi dan pemeriksaan Frekuensi nadi dan pernapasan pasien? Frekuensi nadi dan pernapasan pasien? Apakah pernapasan sama tanpa upaya? Apakah pernapasan sama tanpa upaya? Apakah ada kontraksi otot-otot abdomen selama inspirasi? Apakah ada kontraksi otot-otot abdomen selama inspirasi? Apakah ada penggunaan otot-otot aksesori pernapasan selama pernapasan? Apakah ada penggunaan otot-otot aksesori pernapasan selama pernapasan? Barrel chest? Barrel chest? Apakah tampak sianosis? Apakah tampak sianosis?

36
Apakah ada batuk? Apakah ada batuk? Apakah ada edema perifer? Apakah ada edema perifer? Apakah vena leher tampak membesar? Apakah vena leher tampak membesar? Apa warna, jumlah dan konsistensi sputum pasien? Apa warna, jumlah dan konsistensi sputum pasien? Bagaimana status sensorium pasien? Bagaimana status sensorium pasien? Apakah terdapat peningkatan stupor? Kegelisahan? Apakah terdapat peningkatan stupor? Kegelisahan?

37
Palpasi: Palpasi: Palpasi pengurangan pengembangan dada? Palpasi pengurangan pengembangan dada? Adakah fremitus taktil menurun? Adakah fremitus taktil menurun? Perkusi: Perkusi: Adakah hiperesonansi pada perkusi? Adakah hiperesonansi pada perkusi? Diafragma bergerak hanya sedikit? Diafragma bergerak hanya sedikit?

38
Auskultasi: Auskultasi: Adakah suara wheezing yang nyaring? Adakah suara wheezing yang nyaring? Adakah suara ronkhi? Adakah suara ronkhi? Vokal fremitus nomal atau menurun Vokal fremitus nomal atau menurun

39
Diagnosa Keperawatan Bersihan jalan napas tidak efektif berhubungan dengan bronkokontriksi, peningkatan produksi sputum, batuk tidak efektif, kelelahan/berkurangnya tenaga dan infeksi bronkopulmonal. Bersihan jalan napas tidak efektif berhubungan dengan bronkokontriksi, peningkatan produksi sputum, batuk tidak efektif, kelelahan/berkurangnya tenaga dan infeksi bronkopulmonal. Pola napas tidak efektif berhubungan dengan napas pendek, mucus, bronkokontriksi dan iritan jalan napas. Pola napas tidak efektif berhubungan dengan napas pendek, mucus, bronkokontriksi dan iritan jalan napas. Gangguan pertukaran gas berhubungan dengan ketidaksamaan ventilasi perfusi Gangguan pertukaran gas berhubungan dengan ketidaksamaan ventilasi perfusi Intoleransi aktivitas berhubungan dengan ketidakseimbangan antara suplai dengan kebutuhan oksigen. Intoleransi aktivitas berhubungan dengan ketidakseimbangan antara suplai dengan kebutuhan oksigen.

40
Risiko perubahan nutrisi kurang dari kebutuhan tubuh berhubungan dengan anoreksia. Risiko perubahan nutrisi kurang dari kebutuhan tubuh berhubungan dengan anoreksia. Ganggua pola tidur berhubungan dengan ketidaknyamanan, pengaturan posisi. Ganggua pola tidur berhubungan dengan ketidaknyamanan, pengaturan posisi. Kurang perawatan diri berhubungan dengan keletihan sekunder akibat peningkatan upaya pernapasan dan insufisiensi ventilasi dan oksigenasi. Kurang perawatan diri berhubungan dengan keletihan sekunder akibat peningkatan upaya pernapasan dan insufisiensi ventilasi dan oksigenasi. Ansietas berhubungan dengan ancaman terhadap konsep diri, ancaman terhadap kematian, keperluan yang tidak terpenuhi. Ansietas berhubungan dengan ancaman terhadap konsep diri, ancaman terhadap kematian, keperluan yang tidak terpenuhi.

41
individu tidak efektif berhubungan dengan kurang sosialisasi, ansietas, depresi, tingkat aktivitas rendah dan ketidakmampuan untuk bekerja. individu tidak efektif berhubungan dengan kurang sosialisasi, ansietas, depresi, tingkat aktivitas rendah dan ketidakmampuan untuk bekerja. Kurang pengetahuan berhubungan dengan kurangnya informasi, tidak mengetahui sumber informasi. Kurang pengetahuan berhubungan dengan kurangnya informasi, tidak mengetahui sumber informasi.

42
Masalah kolaboratif/Potensial komplikasi yang dapat terjadi Gagal/insufisiensi pernapasan Gagal/insufisiensi pernapasan Hipoksemia Hipoksemia Atelektasis Atelektasis Pneumonia Pneumonia Pneumotoraks Pneumotoraks Hipertensi paru Hipertensi paru Gagal jantung kanan Gagal jantung kanan

Presentasi serupa





 the RIGHT one for me?” “Should I BUY this? Or SELL that?” “Should I INVEST in.>")


 setelah 2 jam EfekKadar COHb di dalam darah ( %) 0 - 10Tanpa gangguan0-2 10-50Tampak kelelahan2-10 50-100Sedikit sakit.>")











 Hidsal Jamil(135020100111028) Padel Aji Pamungkas(135020100111042)>")

