Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
Manajemen Gangguan Pertukaran Gas

2
Gangguan pertukaran gas adalah kelebihan dan kekurangan oksigen dan/ atau eliminasi karbondioksida di membrane kapiler-alveolar. (Zul Dahlan, 2000)
.")
3
PROSES PERTUKARAN GAS Internal Mitokhondria Inspirasi Ventilasi
Ekspirasi Eksternal Difusi Oksigen Asidosis Transportasi CO2 Alkalosis

4
Gambar Paru-paru

6
Managemen Gangguan Pertukaran Gas

11
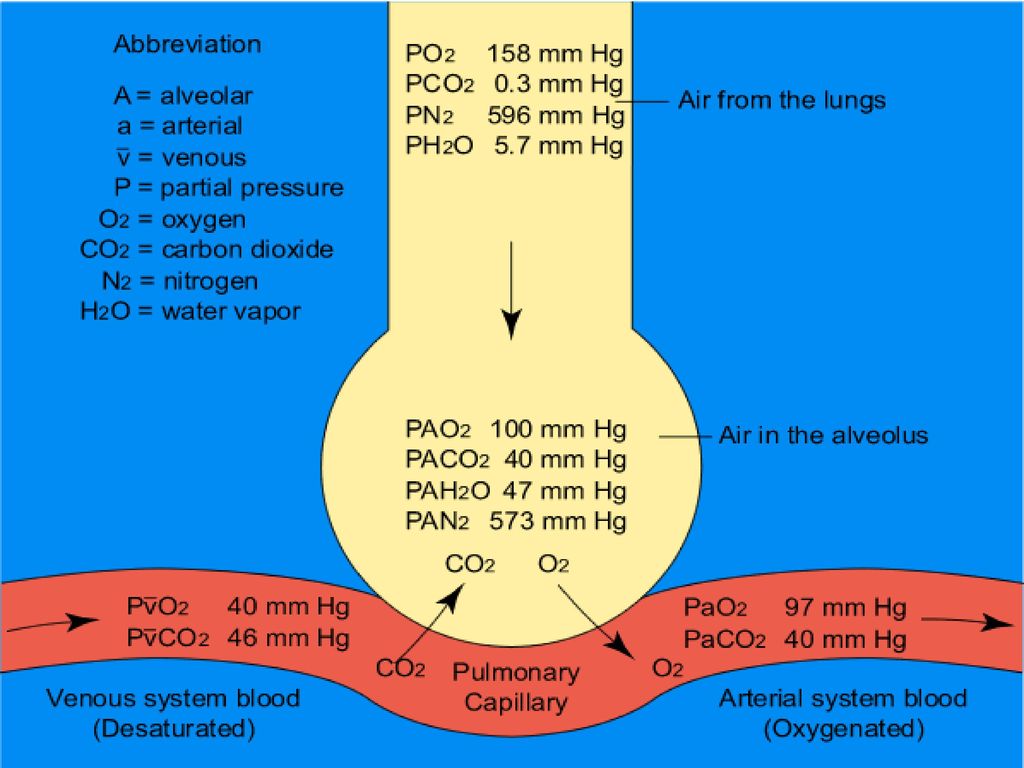
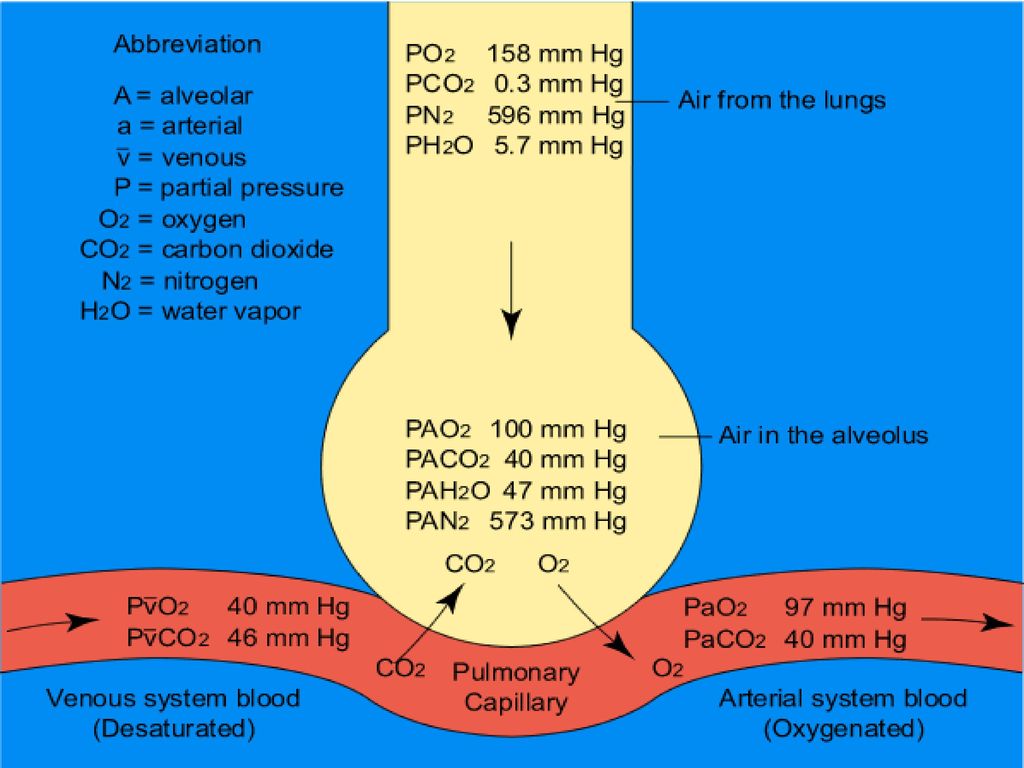
Pertukaran Gas di Paru paru
PO2 in alveoli ~ 100 mm Hg PO2 in pulmonary capillaries ~ 40 mm Hg Result: O2 moves into pulmonary capillaries PCO2 in pulmonary capillaries ~ 46 mm Hg Average arterial blood gases equal PO2 100 mm Hg PCO2 40 mm Hg Exchange of O2 for CO2 occurs by diffusion Structure of gas exchange organs facilitates diffusion

12
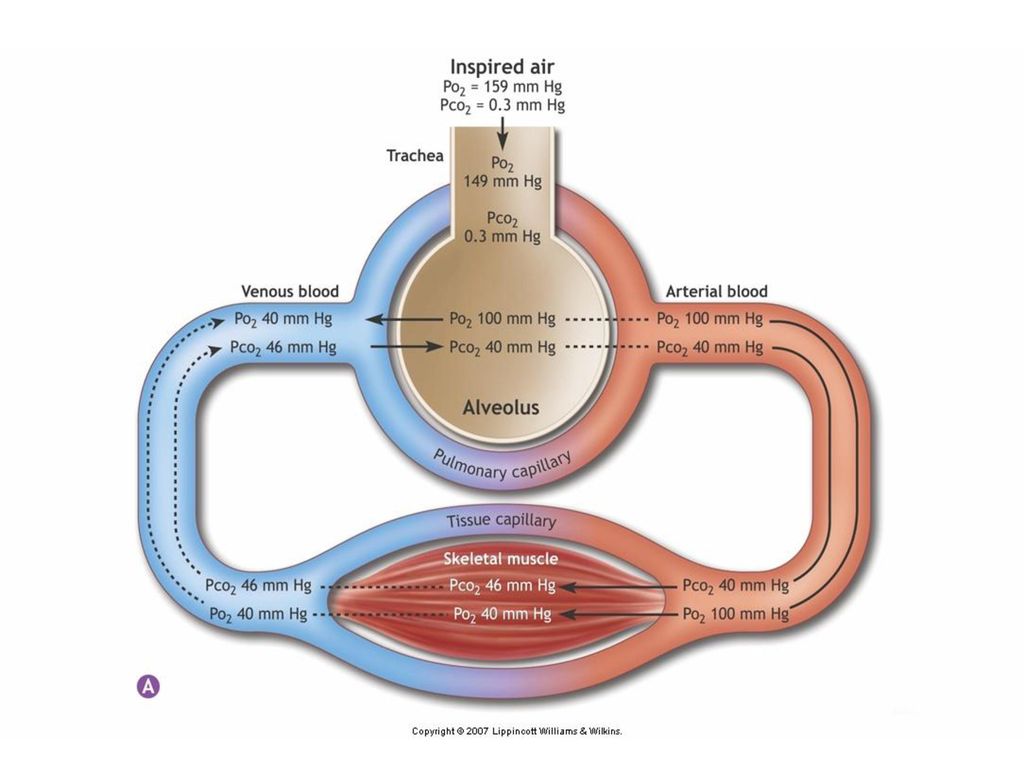
Transpor Gas Ventilation of alveoli
O2 diffusion from alveoli to hemoglobin in RBC’s Equilibrium pO2 = 100 mmHg Diffusion from hemoglobin to body tissues Equilibrium pO2 = 40 mmHg CO2 diffusion from body tissues to hemoglobin Equilibrium pCO2 = 45 mmHg Diffusion from hemoglobin in RBC’s to alveoli Equilibrium pCO2 = 40 mmHg Ventilation of alveoli

13
Hemoglobin Hemoglobin Oxygen-hemoglobin dissociation curve
Exercise lowers pO2 and pH in muscles, higher temperature Hb releases more O2 at low pO2 , low pH, and high temperature Hemoglobin Oxygen-hemoglobin dissociation curve Hb binds O2 at high pO2 Hb releases O2 at low pO2

14
O2 and CO2 Movement Copyright © 2008 Pearson Education, Inc., publishing as Benjamin Cummings.

15
Tekanan Parsial O2 and CO2

16
Tekanan Parsial O2 and CO2
Copyright © 2008 Pearson Education, Inc., publishing as Benjamin Cummings.

17
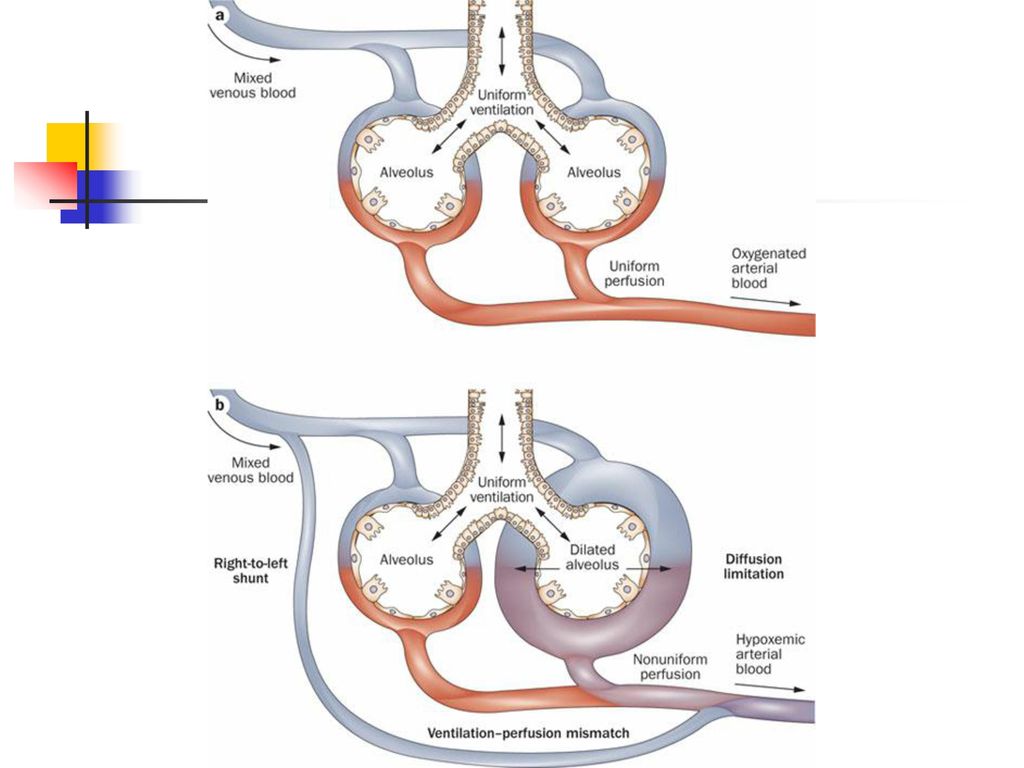
Gas transfer capacity may be impaired by:
Thickening of membrane The thicker the membrane, the slower the rate of diffusion. E.g., edema in the interstitial space increases the distance gasses must diffuse Reduction in surface area If surface area decreases, the rate of diffusion will decrease. E.g., emphysema causes dissolution of alveolar walls

18
Gas transfer capacity may be impaired by:
Diffusion coefficient The diffusion coefficient is proportional to the solubility The greater the diffusion coefficient, the greater the rate of diffusion So, a small molecule that is highly soluble diffuses fast (e.g., CO2). CO2 diffuses ~ 20 x more rapidly than O2 Difference in partial pressure gases will diffuse from areas of high partial pressure to areas of lower partial pressure
. CO2 diffuses ~ 20 x more rapidly than O2. Difference in partial pressure. gases will diffuse from areas of high partial pressure to areas of lower partial pressure.")
19
Copyright © 2008 Pearson Education, Inc
Copyright © 2008 Pearson Education, Inc., publishing as Benjamin Cummings.

20
Assessment Client history Major signs and symptoms Cough Dyspnea
Type, duration, length Sputum production Color, consistency, amount Dyspnea Rate of perception ADLs Paroxysmal nocturnal dyspnea Orthopnea Chest pain, wheezing, clubbing of finger/nails, hemoptysis, cyanosis

21
Risk Factors Smoking Personal / family history Occupation Allergens
Recreational exposure

22
Gerontologic Considerations (1)
Decreased strength of respiratory muscles Decreased elasticity Increased respiratory dead space Decreased number of cilia Decreased cough and gag reflex Increased collagen of alveolar walls

23
Gerontologic Considerations (2)
Vital capacity and respiratory muscle strength peak between and then decrease Age 40 and older – surface area in alveoli is reduced Age 50 – alveoli loses elasticity Loss of chest wall mobility>decrease in vital capacity Amount of respiratory dead space increases with age Decreased diffusion capacity with age – lower oxygen level in arterial circulation

24
Common Management Position Environmental control Activity dan rest
Oral Hygiene Adequate hydration Infection prevention and control Psychosocial support

25
Respiratory Pharmacologic agent
Antimicrobials (Antibiotik) Bronchodilators -adrenergics, seperti : albuterol (ventolin) Theophyline, seperti aminophyline Adrenal Glucocorticoids (Prednison) Antitusive Mucolitycs Antiallergenics Vasoconstristor dan Decongestan
 Bronchodilators. -adrenergics, seperti : albuterol (ventolin) Theophyline, seperti aminophyline. Adrenal Glucocorticoids (Prednison) Antitusive. Mucolitycs. Antiallergenics. Vasoconstristor dan Decongestan.")
26
Respiratory Assessment
Health History Risk factors for respiratory disease-genetics, smoking, allergens, occupational and recreational exposure Dyspnea, orthopnea Cough, ?productive Chest pain Cyanosis Lung sounds Clubbing—indicates chronicity

27
Diagnostic Evaluation (1)
PFTs-assess respiratory function, screening, assess response to therapy FVC—vital capacity performed with a maximally forced expiratory effort Forced expiratory volume—FEV1—volume of air exhaled in the specified time during the performance of forced vital capacity. FEV1 is volume exhaled in one second. FEV1/FVC%--ratio of timed forced exp. volume to forced vital capacity

28
Diagnostic Evaluation (2)
ABGs: 1. pH 2. evaluate the PaCO2 and HCO3- 3. Look to see if compensation has occurred. If CO2 is >40, respiratory acidosis; If HCO3- <24, metabolic acidosis; next look at value other than primary disorder, if moving in same direction as primary value compensation is underway.

29
Diagnostic Evaluation (3)
Pulse oximetry—not reliable in severe anemia, high CO levels, or in shock CO2 monitoring—tells us ventilation to lungs is occurring, that CO2 is being transported to lungs, exp. CO2 indicates adequate ventilation Cultures Imaging—chest xray, CT, MRI, lung scans (inject isotope, inhale radioactive gas), PET Bronchoscopy Thoracentesis others
, PET. Bronchoscopy. Thoracentesis. others.")
30
Respiratory Care Modalities
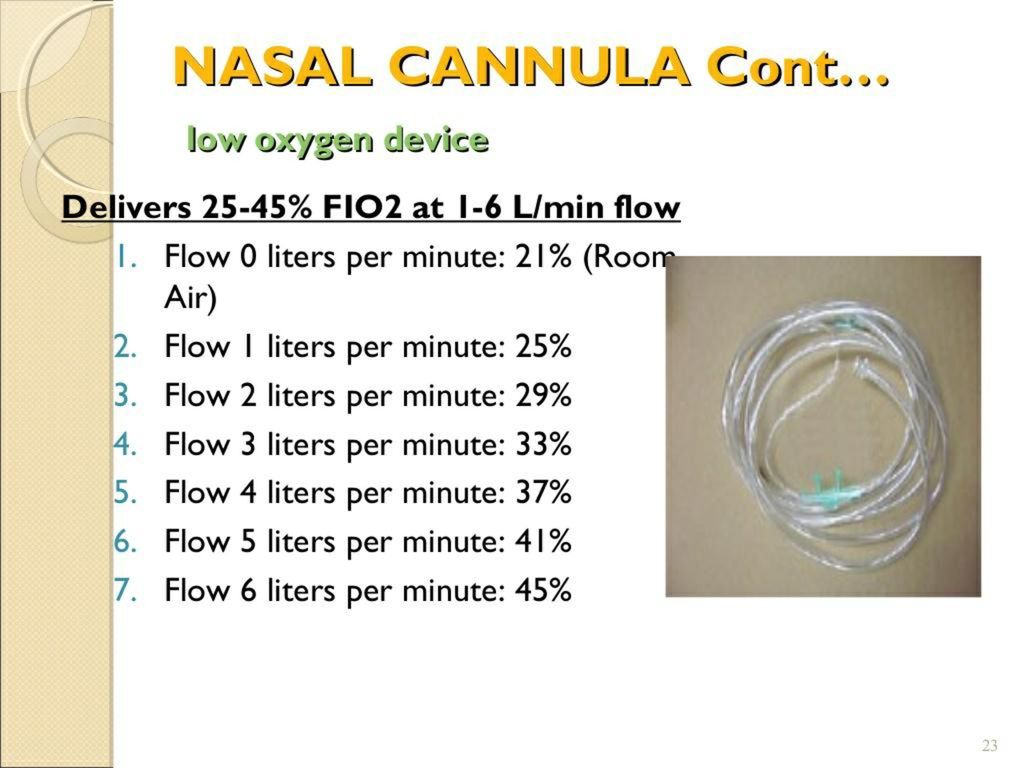
Nasal cannula—up to 6L/min. Delivers up to 42% oxygen Simple mask—flow rate 6-8L/min. Delivers 40-60% oxygen. Partial rebreather mask—flow rate is 8-11L/min. Delivers 50-75% oxygen. Nonrebreather mask—flow at 12 L/min. Delivers % oxygen. Venturi mask—4-6 L/min, 6-8 L/min. Deliver respective oxygen concentration of 24, 26, 28 or 30, 35, 40% oxygen. Most accurate delivery.

34
Tracheostomy (1) Surgical procedure in which an opening is made into the trachea Tracheostomy tube Temporary or permanent Used to bypass an upper airway obstruction, allow removal of tracheobronchial secretions, permit long term use of mechanical ventilation, to prevent aspiration in unconscious patient or to replace endotracheal tube

35
Tracheostomy (2) Complications of tracheostomy:
Bleeding, pneumothorax, air embolism, aspiration, subcutaneous or mediastinal emphysema, recurrent laryngeal nerve damage Airway obstruction from accumulation of secretions ,tracheoesophageal fistula, tracheal ischemia

36
Tracheostomy (3) Nursing care of the patient with tracheostomy:
Initially, semi-fowler’s position to facilitate ventilation, promote drainage, minimize edema, and prevent strain on the sutures Allow method of communication Ensure humidity to trach Suction secretions as needed Manage cuff—usually keep pressure less than 25 mm Hg but more than 15 mm Hg to prevent aspiration

37
Endotracheal Intubation
Pass ETT via nose or mouth into trachea Method of choice in emergency situation Passed with aid of a laryngoscope ETT generally has a cuff, ensure that cuff pressure is between mm Hg. Use warmed, humidified oxygen Should not be used for more than 3 week

38
Preventing Complications Associated with Endotracheal and Tracheostomy Tubes
Administer adequate warmed humidity Maintain cuff pressure at appropriate level Suction as needed Maintain skin integrity Auscultate lung sounds—ETT can lodge in right mainstem bronchus Monitor for s/s of infection Monitor for cyanosis Maintain hydration of patient Use sterile technique when suctioning and performing trach care Monitor O2 sat

39
Mechanical Ventilation
Used to control patient’s respirations, to oxygenate when patient’s ventilatory efforts are inadequate, to rest respiratory muscles Can be positive pressure or negative pressure Key for the nurse is assess patient—not the ventilator

40
Indications for Mechanical Ventilation
PaO2 <50 mm Hg with FiO2 >0.60 PaO2 >50 mm Hg with pH <7.25 Vital capacity < 2 times tidal volume Negative inspiratory force < 25 cm H20 Respiratory rate > 35 bpm ( *vital capacity is dependent on age, gender, weight and body build. Usually is twice tidal volume. If < 10mL/kg, will need respiratory assist)
")
41
Thoracic Surgeries (1) Pneumonectomy Lobectomy Segmental resection
Lung volume reduction, etc Manage potential complication: Monitor respiratory status Vitals For dysrhythmias For bleeding, atelectasis and infection Monitor chest tube drainage, for leaks, for tube kinks, for excessive drainage

42
Thoracic Surgeries (2) Care of patient after thoracotomy:
Maintain airway clearance Positioning-lobectomy turn either side,pneumonectomy turn on affected side, segmental resection varies per doctor Chest tube drainage/care Relieve pain Promote mobility Maintain fluid volume and nutrition

43
Position of Postural Drainage

44
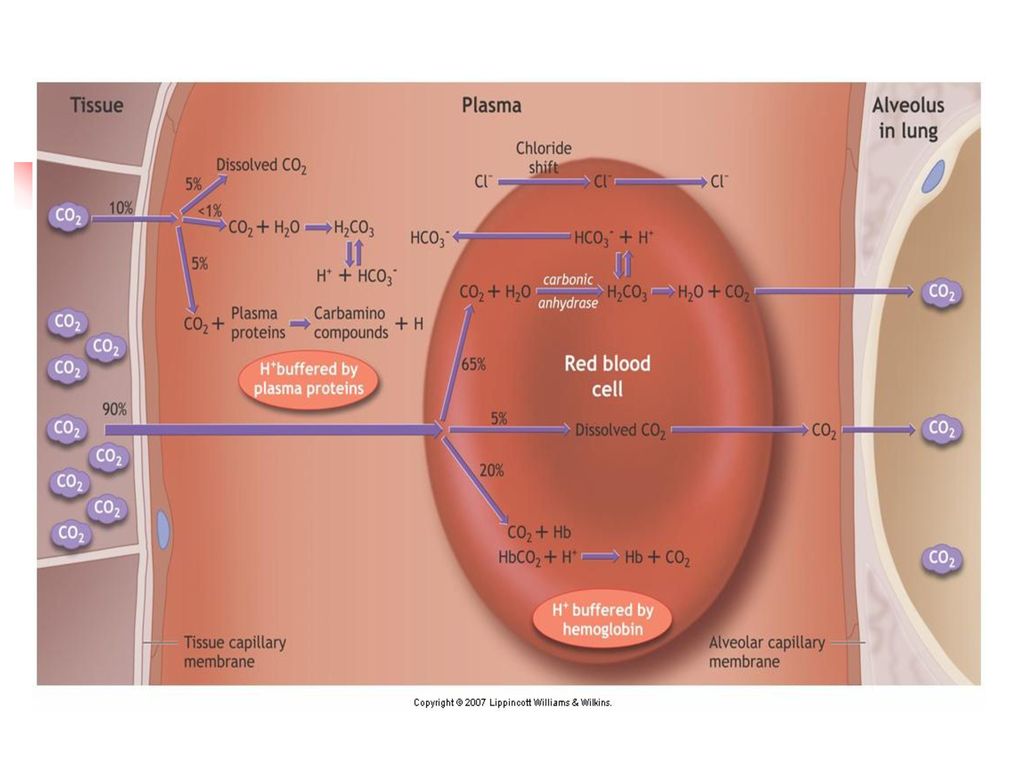
Keseimbangan Asam Basa
CO2 + H2O H2CO3 H+ + HCO3- Asidosis : Hipoventilasi, Retensi CO2 Alkalosis : Hiperventilasi, Ekskresi CO2

45
Kendali Pernafasan Faktor Lokal : Kontrol Medulla Oblongata :
Kontrol Pons : transisi insp – eks Refleks Hering-Breur : Masukkan Korteks : Kendali Bio Kimiawi : Efek Latihan Jasmani : Efek Altitude/Ketinggian

46
Tindakan Umum Posisi Kontrol Lingkungan Aktifitas dan Istirahat.
Oral Hygiene. Hidrasi Adekuat Pencegahan dan Kontrol Infeksi Support Psikososial

47
Respiratory Pharmacologic agent
Antimicrobials (Antibiotik) Bronchodilators -adrenergics, seperti : albuterol (ventolin) Theophyline, seperti aminophyline Adrenal Glucocorticoids (Prednison) Antitusive Mucolitycs Antiallergenics Vasoconstristor dan Decongestan
 Bronchodilators. -adrenergics, seperti : albuterol (ventolin) Theophyline, seperti aminophyline. Adrenal Glucocorticoids (Prednison) Antitusive. Mucolitycs. Antiallergenics. Vasoconstristor dan Decongestan.")
48
Terapi Respirasi Batuk Efektif dan Nafas Dalam
Fungsi : meningkatkan “Normal Cleansing Mechanism”. Batuk yang tidak efektif : Kolaps saluran nafas Ruptur dinding alveoli pneumothoraks

49
Terapi………… Fisioterapi dada : Clapping Vibrasi Postural Drainage

50
Postural Drainage Prinsip : gravitasi ke dalam bronkus mayor dan trakea. Tujuan : Menggerakkan sekresi yang terakumulasi Mencegah akumulasi sekresi pada klien yang tidak sadar atau yang diberikan ventilasi mekanis. dilakukan sebanyak 2-3 kali perhari, Waktu terbaik : sebelum sarapan, sebelum makan siang, sore hari atau sebelum tidur.

51
Postural……….. kategori posisi, yaitu :
Posisi yang mendrainase segmen atas atau lobus atas paru. Posisi yang mendrainase segmen tengah paru (hanya pada paru kanan). Posisi yang mendrainase segmen basal paru atau lobus bawah.
. Posisi yang mendrainase segmen basal paru atau lobus bawah.")
52
Posisi Postural Drainage

53
Oksigen Diberikan ketika hipoksemia timbul atau dicurigai akan timbul dimana dengan hipoksemia tertanggulangi maka hipoxia akan dapat dicegah. indikasi : Menurunnya Arterial Blood Oxygen. Meningkatnya kerja nafas Kebutuhan untuk menurunkan kerja myocardial.

54
Komplikasi Oksigen Oxygen-induced Hypoventilation Oxygen Toxicity.
Atelektasis Occular Damage.

55
Alat Pemberian O2 Alat-alat oksigen aliran rendah : kanula nasal, masker sederhana, rebreather dan Non-rebreather. Alat-alat oksigen aliran tinggi adalah : masker venturi, masker aerosol, collar trakeostomi, T-Piece, sungkup.

Presentasi serupa