Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
PENYAKIT KELENJAR ADRENAL - Cushing’s Syndrome -
OLEH : Woro Harjaningsih

2
Definisi adalah kondisi klinik sebagai akibat dari paparan kronik glukokortikoid menyebabkan kadar glukokortikoid dlm sirkulasi berlebihan. disebut juga sebagai hiperadrenokortikalisme Hiperadrenalkortikalisme Hiperkortisolisme Penyebab paling umum : sekresi berlebih ACTH dari kelenjar hipofisis anterior (Cushing’s disease)
")
3
ETIOLOGI Cushing’s disease : Dapat tjd :
secara spontan cushing’s syndrome spontaneous atau , merupakan penyebab terbesar, kejadian kira2 2 – 4 kasus / juta populasi dan pd wanita 9 X lebih banyak drpd laki-laki sebagai hasil pemberian kronik (jangka panjang) kortikosteroid Cushing’s syndrome iatrogenic
 kortikosteroid Cushing’s syndrome iatrogenic.")
4
Spontaneous cushing’s syndrome / Cushing’s disease bisa tjd akibat :
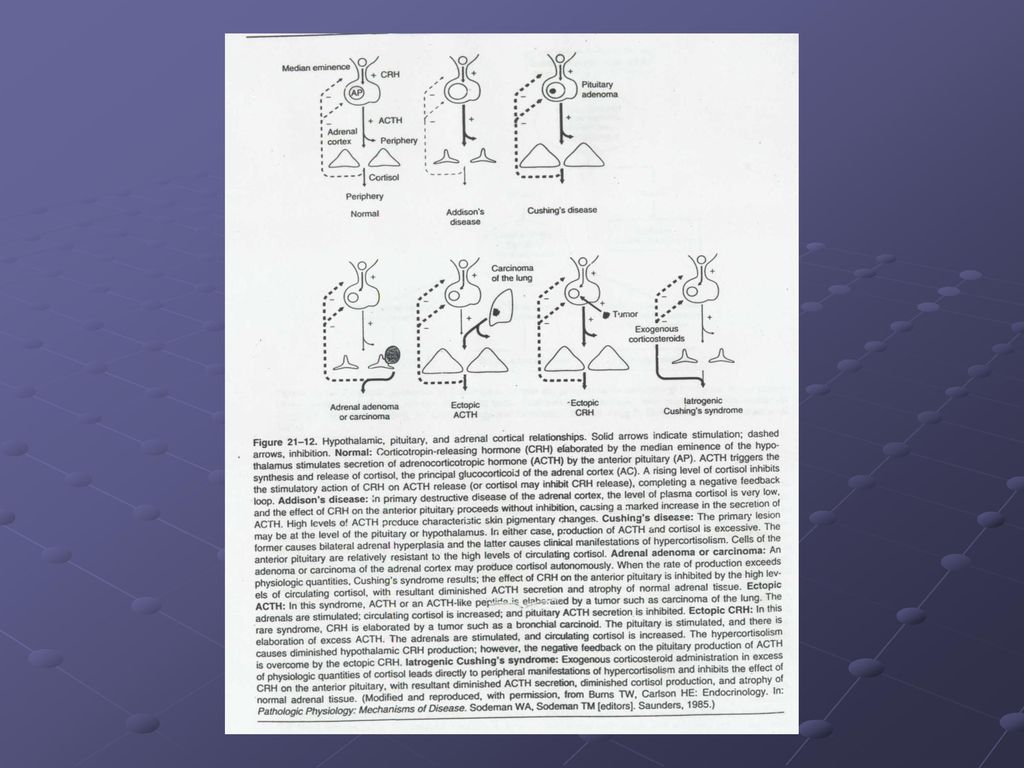
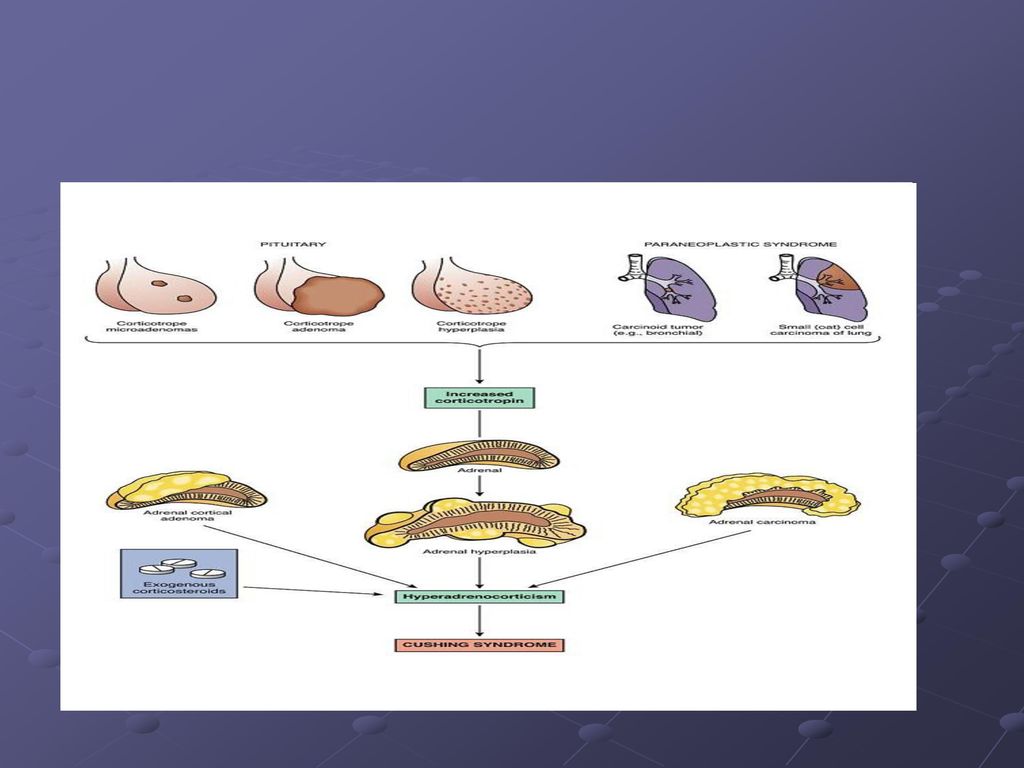
Adenoma hipofisis sekresi berlebih ACTH (> 90%) Hiperplasia difuse / pituitary corticotroph cells yg bertanggung jawab thdp hipersekresi ACTH Hiperplasia kmk krn hipersekresi CRH oleh hipotalamus atau tumor pensekresi CRH (CRH-secreting tumors) Hipersekresi kronik CRH tidak menyebabkan adenoma hipofisis
 Hiperplasia difuse / pituitary corticotroph cells yg bertanggung jawab thdp hipersekresi ACTH. Hiperplasia kmk krn hipersekresi CRH oleh hipotalamus atau tumor pensekresi CRH (CRH-secreting tumors) Hipersekresi kronik CRH tidak menyebabkan adenoma hipofisis.")
5
B. Ectopic ACTH Syndrome
Tumor non hipofisis mensintesis & mensekresikan secara berlebih (hipersekresi) ACTH yg aktif secara biologi atau peptida menyerupai ACTH (ACTH-like peptide) Biasanya karsinoma sel kecil dari paru atau tumor karsinoid dari bronkhial Lebih banyak menyerang laki-laki
 ACTH yg aktif secara biologi atau peptida menyerupai ACTH (ACTH-like peptide) Biasanya karsinoma sel kecil dari paru atau tumor karsinoid dari bronkhial. Lebih banyak menyerang laki-laki.")
6
C. ECTOPIC CRH Syndrome Sangat jarang menyebabkan Cushing’s Syndrome Sebagian besar kasus berhub dg tumor karsinoid bronkhial

7
D. Functioning Adrenocortical Tumors
Baik adrenocortical adenoma dan carcinoma menyebabkan Cushing’s syndrome melalui pengeluaran kortisol secara autonom Adenoma memp vaskuler yang tinggi, dengan area nekrosis, perdarahan, degenerasi kista dan kalsifikasi bisa metastase ke ginjal, retroperitoneum, liver dan paru

8
E. Adrenal Micronodular Hyperplasia
Jarang menyebabkan Cushing’s Syndrome Sekitar separuh kasus timbul secara mendadak pada anak2 dan dewasa muda

9
F. Adrenal Macronodular Hyperplasia
Jarang menyebabkan Cushing’s Syndrome Beberapa pasien dg macronodular hyperplasia tidak menunjukkan gambaran cushingoid tipikal

11
Patofisiologi

12
Patofisiologi Penyebab dapat dibagi 2 kategori :
ACTH-dependent peningkatan kadar kortisol tergantung pada ACTH dan tidak dapat menekan sekresi ACTH dari hipofisis ACTH-independent peningkatan kadar kortisol tidak tergantung ACTH (autonom) dan dapat menekan sekresi ACTH dari hipofisis
 dan dapat menekan sekresi ACTH dari hipofisis.")
14
Klasifikasi ACTH dependent Cushing’s disease Ectopic ACTH syndrome
Ectopic corticotropin-releasing hormone syndrome* ACTH independent Iatrogenic Adrenal adenoma Micronodular hyperplasia* Macronodular hyperplasia* Ket : ACTH : Adrenocorticotropin hormone * : accounts per 1 percent or less of cases (Adapted with permission from Orth DN Cushing’s Syndrome. N Engl. J. Med, 1995 ; 332 : 791 – 803)
")
15
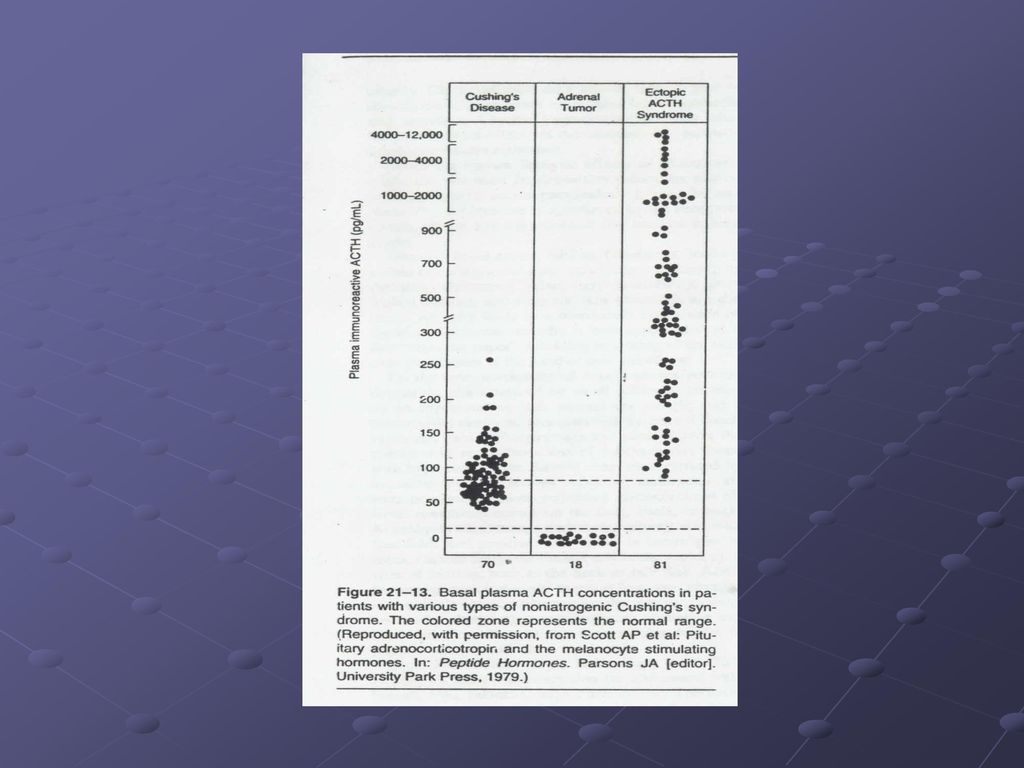
ACTH-dependent Cushing’s syndrome :
~ Cushing’s disease 80% kasus ACTH-dependent ~ Ectopic ACTH hypersecretion 20% ~ Ectopic CRH secretion jarang Dimana kesemuanya ditandai dg hipersekresi ACTH kronik dan peningkatan sekresi kortisol

16
ACTH-independent Cushing’s syndrome :
~ Glucocorticoid-secreting adrenocortical adenoma dan carcinoma ~ Adrenal micronodular dan macronodular hyperplasia Kesemuanya ditandai dg sekresi secara autonom kortisol dan penekanan ACTH hipofisis

17
Adrenal tumor Carcinoma dan adrenal adenoma primer tidak di bawah kendali hipotalamus-hipofisis dan kmd secara autonom mensekresikan lebih kortisol Hiperkortisol menekan produksi ACTH hipofisis menyebabkan atrofi korteks adrenal

19
Manifestasi Klinik

21
FUNGSI KORTISOL Memelihara tekanan darah dan fungsi kardiovaskuler.
Menurunkan respon inflamasi sistem imun. Menyeimbangkan efek insulin dalam memecah glukosa untuk energi. Mengatur metabolisme protein, karbohidrat, dan lemak. Fungsi terpenting : membantu tubuh terhadap respon stress. (kadar kortisol wanita pada kehamilan 3 bln terakhir dan atlit secara normal tinggi). dmk juga pada orang2 dg depresi, alkoholisme, malnutrisi dan gangguan panik.
. dmk juga pada orang2 dg depresi, alkoholisme, malnutrisi dan gangguan panik.")
22
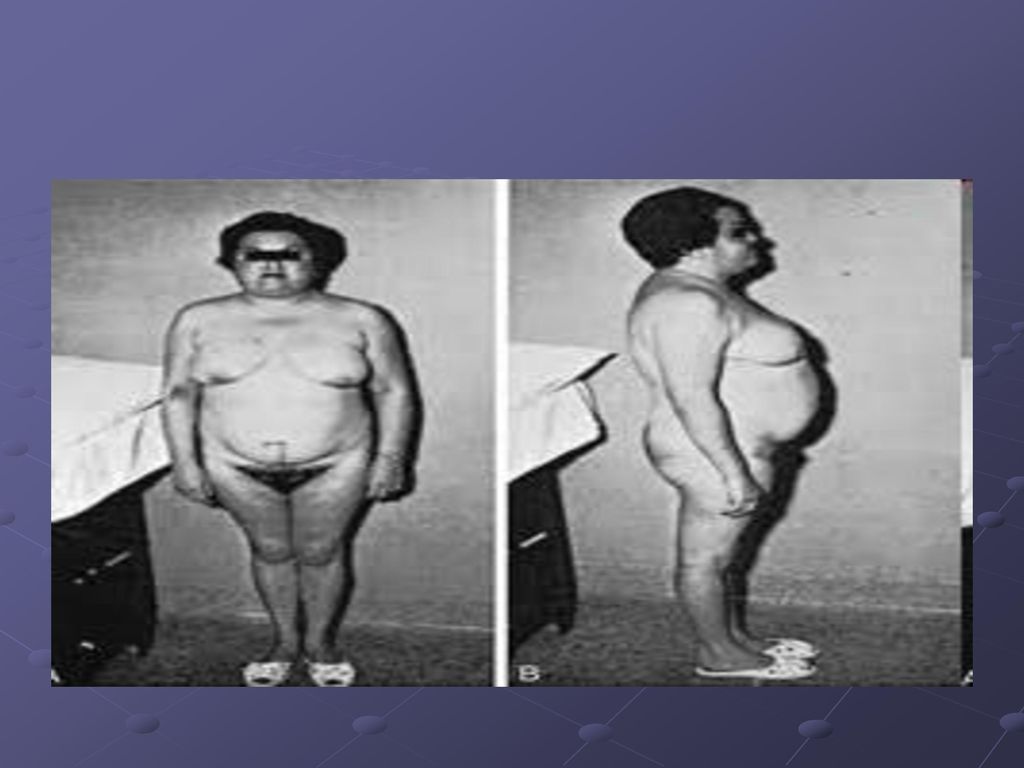
GEJALA Obesitas tubuh bagian atas, muka bulat, peningkatan lemak sekitar leher, lengan dan kaki kurus, pada anak-anak pertumbuhan lambat. Gejala lain : kulit fragile, kurus, memar dan tidak sehat, kulit warna ungu pink pada perut, paha, lengan dan payudara.(striae) Tulang rapuh dan bengkok, patah tulang (fraktur) pada tulang rusuk (iga) dan tulang belakang. Sangat lelah, otot lemah, tek. darah dan kadar gula darah tinggi, irritabilitas, ansietas, depresi. Pertumbuhan rambut pada muka, leher, dada, perut dan paha (pada wanita) Periode menstruasi tidak teratur/ terhenti. Penurunan libido sex pada laki-laki
 Tulang rapuh dan bengkok, patah tulang (fraktur) pada tulang rusuk (iga) dan tulang belakang. Sangat lelah, otot lemah, tek. darah dan kadar gula darah tinggi, irritabilitas, ansietas, depresi. Pertumbuhan rambut pada muka, leher, dada, perut dan paha (pada wanita) Periode menstruasi tidak teratur/ terhenti. Penurunan libido sex pada laki-laki.")
23
Penderita Cushing’s Syndrome

24
Penderita Cushing’s Syndrome anak
25
Gejala Cushing’s Syndrome Striae pada abdomen dan payudara
26
Moonface
27
Moonface
28
Striae pada stomach
29
Striae

30
Pertumbuhan rambut pada dada
31
Striae pada lengan
32
Striae pada siku
33
Buffalohump (punggung menebal)
34
Buffalohump (punggung menebal)
35
Exogenous Cushing Syndromme
37
DIAGNOSIS Berdasarkan tinjauan riwayat medis pasien, pemeriksaan fisik, dan test lab. X ray : utk menentukan lokasi tumor. 24 urin 24 jam bebas kortisol paling spesifik, kadar > 50 – 100 µg / hari utk dewasa cushing’s syndrome Test Supresi Dexametason utk membedakan peningkatan ACTH karena adenoma hipofisis dan tumor ektopik. Test Stimulasi CRH utk membedakan antara adenoma hipofisis dengan sindroma ACTH ektopik atau tumor adrenal penghasil kortisol

38
DIAGNOSIS Visualisasi langsung Kelenjar Endokrin (Imaging Radiologi)
- melihat ukuran dan bentuk kelenjar hipofisis dan adrenal serta menentukan jika ada tumor. - dengan CT ( Computerized Tomography) scan dan MRI (Magnetic Resonance Imaging). Sampling Sinus Petrosal - test terbaik utk membedakan penyebab Cushing’s syndrome antara hipofisis dengan ektopik. Test Dexametason – CRH - membedakan Cushing’s syndrome dengan Pseudo Cushing’s Syndrome secara cepat. - Peningkatan kadar kortisol selama test menunjukkan adanya Cushing’s Syndrome
 scan dan MRI (Magnetic Resonance Imaging). Sampling Sinus Petrosal. - test terbaik utk membedakan penyebab Cushing’s syndrome antara hipofisis dengan ektopik. Test Dexametason – CRH. - membedakan Cushing’s syndrome dengan Pseudo Cushing’s Syndrome secara cepat. - Peningkatan kadar kortisol selama test menunjukkan adanya Cushing’s Syndrome.")
39
Pseudo-Cushing's syndrome is a medical condition in which patients display the signs, symptoms, and abnormal hormone levels seen in Cushing's syndrome. Pseudo-Cushing's syndrome, however, is not caused by a problem with the hypothalamic-pituitary-adrenal axis as Cushing's is. It is an idiopathic condition.

40
Pemeriksaan lab Pseudo Cushing Syndromme
Levels of cortisol and ACTH are both high 24-hour urinary cortisol levels are high Dexamethasone suppression test fails to suppress serum cortisol Loss of diurnal variation in cortisol levels- Loss of Diurnal Variation is seen only in true Cushing's Syndrome or Disease. High mean corpuscular volume and gamma-glutamyl transferase may be clues to alcoholism Polycystic Ovarian Syndrome should be ruled out, since PCOS has similar symptoms.

41
Diagnosis banding=Differential diagnosis
Differentiation from Cushing's is extremely difficult Causes of Cushing's should be excluded with imaging of the lungs, adrenal glands, and pituitary gland - but these often appear normal in Cushing's anyway In the alcoholic patient with pseudo-Cushing's, admission to hospital (and avoidance of alcohol) will result in normal midnight cortisol levels within 5 days, excluding Cushing's[1]
 will result in normal midnight cortisol levels within 5 days, excluding Cushing s[1]")
42
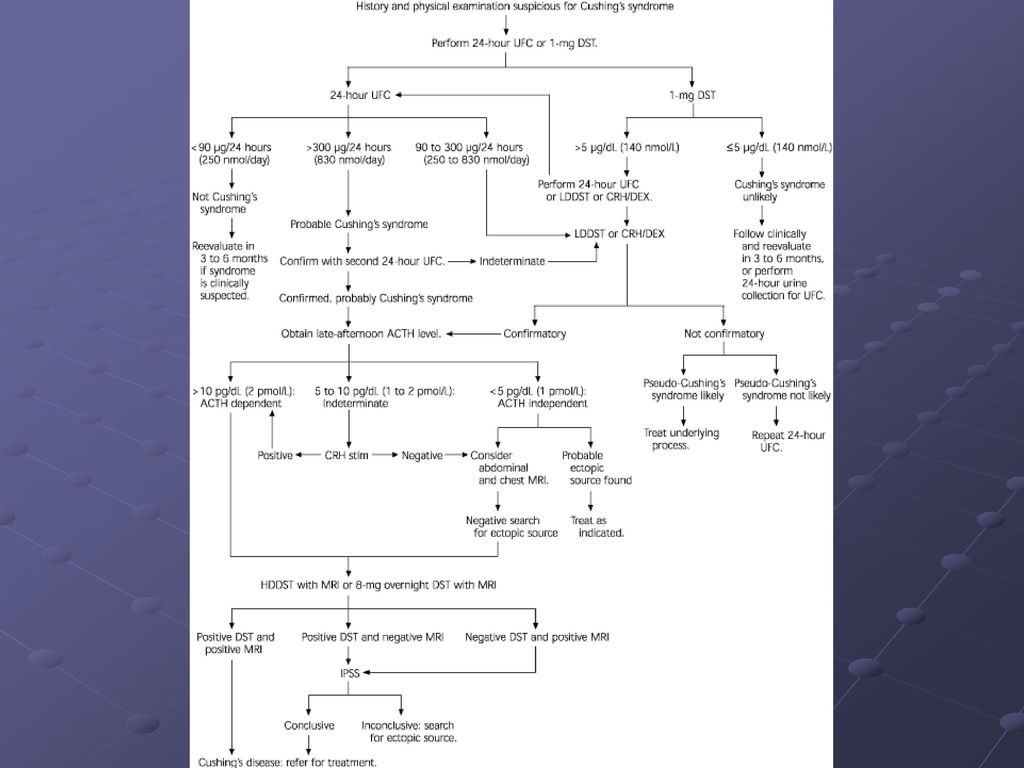
Diagnosa kerja utk menegakkan Cushing’s Syndrome

45
MRI pada adrenal tumor

46
Test utk mendiagnosa Cushing’s syndrome
Normal Hyperplasia Adenoma Carcinoma Plasma Kortisol (μg/dL, AM/PM) 17/8 / / / After low-dose DST After high-dose DST / Normal ACTH (pg/mL) Urine Kortisol (μg/24 h)
 17/8. / / / After low-dose DST. After high-dose DST. / Normal. ACTH (pg/mL) Urine. Kortisol (μg/24 h) ")
47
Sasaran terapi Karena terjadi hiperkortisolisme maka sasaran terapinya adl menurunkan kadar kortisol plasma TERAPI tergantung etiologi / penyebab Terapi farmakologi obat Terapi non farmakologitindakan bedah / operasi dan radiasi

48
TERAPI Treatment Dosing Etiology Non drug Drug Initial Usual Max
Ectopic ACTH syndrome Surgery Chemotherapy Irradiation Metyrapone tabs 250 mg Aminoglutethimide tabs, 250 mg 1 – 1, 5 g/d, divided q4-6 h 0,5-1 g/d, divided 96 bid – qid x 2 weeks 1 – 6 g/d, divided q4-6 h 1 g/d, divided q6 6 g/d 2 g/d Pituitary dependent Cyproheptadine, 2 mg/5 mL syrup or 4 mg tabs Mitotane tabs 500 mg Metyrapone 4 mg bid 1-6 g/d, increased by 1-2 g/d q3-7d See above 24 – 32 mg/d., divided qid 9 – 10 g/d, divided tid – qid 32 mg/d 16 g/d Adrenal adenoma Surgery + postoperative replacement Ketokonazole, tabs 200 mg 200 mg qd - bid 600 – 800 mg/d, divided bid 1200 mg/d Adrenal carcinoma Mitotane

49
Terapi farmakologi Steroid inhibitor Adrenolitik agent mitotan
Neuromodulator agent Antagonis reseptor glukokortikoid

50
Steroid Inhibitor Inhibitor steroid : metyrapone, aminogluthetimide,
ketokonazole Metyrapone dan aminogluthetimide bila tdk kontinu, mempunyai efikasi terbatas → shg digunakan sesudah operasi. Metyrapone : menghambat aktivitas 11 – hydroxylase, sehingga sintesis kortisol terhambat. Setelah terapi akan diikuti dg peningkatan kadar ACTH plasma, karena tjd penurunan mendadak kortisol. ES : mual, muntah, vertigo, sakit kepala, bingung, sakit perut, rash.

51
Ketokonazole Antifungal derival imidazole
Mempunyai efektivitas tinggi menurunkan kortisol Mek kerja : menghambat enzim sit P450 (11 – hydroxylase dan 17- hydroxylase) ES : ginekomastia & penurunan kadar testoterone plasma ES umum : peningkatan transaminase hepatik (reversibel), ginekomastia, gangguan GI
 ES : ginekomastia & penurunan kadar testoterone plasma. ES umum : peningkatan transaminase hepatik (reversibel), ginekomastia, gangguan GI.")
52
Aminoglutethimide Pertama digunakan utk epilepsi, kmd sbg inhibitor sintesis kortisol yg poten Mek. Kerja : menghambat konversi kolesterol mjd pregnenolon. Penurunan kortisol plasma sampai dg 50% ES : sedasi, mual, ataksia, dan skin rash. Interaksi : dg warfarin akan menurunkan efek antikoagulan. Indikasi : penggunaan jangka pendek Cushing’s disease dg sindrom ACTH ektopik, digunakan sbg kombinasi dg metyrapone → efektif pd cushing yg tdk dpt dioperasi.

53
Adrenolytic agent mitotane (orto-para-dichlorodiphenyl dichloroethane)
Menghambat 11-hidroksilasi dari 11-desoksikortisol dan 11-desoksikortikosteron pada korteks. Menurunkan sekresi kortisol plasma, urin, 17-substitued kortisol. Mitotane secara selektif menghambat fs adrenokortikal tanpa menyebabkan destruksi seluler. Karena tjd penurunan besar kortisol, perlu monitoring penurunan kortisol di RS. ES : 80% pasien mengalami lethargi dan somnolen, 40% pasien dg ES CNS lainnya, hiperkolesterolemia.

54
Neuromodulator agent Cyproheptadine Bromocriptine Valproic acid
Octreotide

55
Cyproheptadine Menurunkan sekresi ACTH
Perlu monitoring kadar kortisol pada urin 24 jam bebas kortisol ES : sedasi & hiperfagia Respon Rate (RR) tidak lebih 30%, jadi perlu dipantau kekambuhannya
 tidak lebih 30%, jadi perlu dipantau kekambuhannya.")
56
Antagonis reseptor glukokortikoid
RU-486 (mifepristone) adl antagonis reseptor progesteron dan glukokortikoid menghambat supresi deksametason dan kortisol endogen. Spironolactoneantagonis kompetitif aldosteron, memperbaiki hipertensi & hipokalemia pada Cushing’s syndrome
 adl antagonis reseptor progesteron dan glukokortikoid menghambat supresi deksametason dan. kortisol endogen. Spironolactoneantagonis kompetitif aldosteron, memperbaiki hipertensi & hipokalemia pada Cushing’s syndrome.")
57
Terapi adenoma hipofisis
1. Dg pembedahan →transsphenoidal adenomectomy (tkt keberhasilan 80%), penurunan ACTH sampai 2 tingkat di bwh Normal Jk tjd penurunan drastis →suplai kortisol sintetik (hidrokortison/prednison) Jika pembedahan gagal → radioterapi (> 6 mgu), tkt keberhasilan 40 – 50% pada dws, > 80% pada anak. 2. Kombinasi radiasi dg Mitotane (Lysodren) Mitotane menekan produksi kortisol & menurun kadarnya dlm plasma dan urine, 30 – 40 % pasien berhasil 3. Aminoglutethimide, Metyrapone, Trilostane & Ketokonazole → ada ES
, penurunan ACTH sampai 2 tingkat di bwh Normal. Jk tjd penurunan drastis →suplai kortisol sintetik (hidrokortison/prednison) Jika pembedahan gagal → radioterapi (> 6 mgu), tkt keberhasilan 40 – 50% pada dws, > 80% pada anak. 2. Kombinasi radiasi dg Mitotane (Lysodren) Mitotane menekan produksi kortisol & menurun kadarnya. dlm plasma dan urine, 30 – 40 % pasien berhasil. 3. Aminoglutethimide, Metyrapone, Trilostane & Ketokonazole → ada ES.")
58
Terapi sindroma ACTH ektopik
Prinsip terapi : eliminasi semua jaringan kanker penghasil ACTH (misal sel kanker paru) Pembedahan Radioterapi Kemoterapi Imunoterapi Kombinasi →tgt tipe dan luas kanker
 Pembedahan. Radioterapi. Kemoterapi. Imunoterapi. Kombinasi →tgt tipe dan luas kanker.")
59
Tumor adrenal Dg : Pembedahan adrenolectomy Pada Primary Pigmented Micronodular Adrenal Disease dan Carney’s Complex dg pembedahan kel. Adrenal.

60
Learn How to Treat Cushing's Syndrome
1Cushing's syndrome may be caused in different ways and categorized accordingly. Long-term use of steroids (such as prednisone) or adrenal abnormalities can cause the disease to surface. However, pituitary adenomas (benign tumors) are to blame in most cases, and this condition is referred to as Cushing's disease. In other cases, ectopic ACTH syndrome is at work, which means malignant tumors have formed on the pituitary, causing a domino reaction of ACTH and cortisol release. 2The exact reason your body is producing too much cortisol will determine how to treat the disease. Conventional treatments include radiation, chemotherapy, administration of cortisol-inhibiting drugs and/or surgery. 3Pituitary adenomas are usually treated by a surgical procedure called a transsphenoidal adenomectomy, which has a better than 80 percent success rate. The pituitary gland is accessed through the nose via a thin tube containing a microscope, and tiny instruments are used to remove the tumor.
 or adrenal abnormalities can cause the disease to surface. However, pituitary adenomas (benign tumors) are to blame in most cases, and this condition is referred to as Cushing s disease. In other cases, ectopic ACTH syndrome is at work, which means malignant tumors have formed on the pituitary, causing a domino reaction of ACTH and cortisol release. 2The exact reason your body is producing too much cortisol will determine how to treat the disease. Conventional treatments include radiation, chemotherapy, administration of cortisol-inhibiting drugs and/or surgery. 3Pituitary adenomas are usually treated by a surgical procedure called a transsphenoidal adenomectomy, which has a better than 80 percent success rate. The pituitary gland is accessed through the nose via a thin tube containing a microscope, and tiny instruments are used to remove the tumor.")
61
Cont’d 4Be aware that surgery on the pituitary may cause ACTH levels to fall below normal, which is typical. Therefore, it may become necessary to follow up with administration of a synthetic form of cortisol, such as hydrocortisone or prednisone. 5Expect that radiotherapy or a combination of radiation therapy and medication may be necessary if you're not a good candidate for surgery. While radiation works to shrink tumors, drugs such as mitotane (Lysodren) help to inhibit cortisol production. 6Know that there are several medications used to control cortisone secretion, including mitotane, aminoglutethimide, metyrapone, trilostane and ketoconazole. Read more: How to Treat Cushing's Syndrome | eHow.com
 help to inhibit cortisol production. 6Know that there are several medications used to control cortisone secretion, including mitotane, aminoglutethimide, metyrapone, trilostane and ketoconazole. Read more: How to Treat Cushing s Syndrome | eHow.com")
62
Monitoring terapi Kadar kortisol serum pada pemeriksaan urin 24 jam bebas kortisol Perbaikan gejala & manifestasi klinik Cushing’syndrome Risiko kekambuhan terutama utk obat2 dg RR yg rendah

63
Penderita Cushing’s sebelum pembedahan

64
Penderita Cushing’s sesudah pembedahan

65
Sesudah pembedahan & sebelum pembedahan
66
Adrenocortical carcinoma in infant

67
The patient is a Caucasian female born at term with a birth weight of 3.06 kg; pregnancy and delivery were uncomplicated. At six months of age, she was referred to pediatric endocrine clinic due to features of Cushing syndrome. She had a three month history of progressive Cushingoid facies, acne and irritability. Her linear growth apparently had been arrested between three and six months of age, although she gained weight at an accelerated rate. Prior to referral, laboratory evaluation by her primary care physician revealed serum cortisol of 240 mcg/dl (normal, 4.5–22.7 mcg/dl); total testosterone of 185 ng/dl (normal, 6–77ng/dl), and DHEA-S of 401 mcg/dl (normal, 16–96 mcg/dl). Serum ACTH was less than 5 pg/ml (normal, 10–60 pg/ml).
; total testosterone of 185 ng/dl (normal, 6–77ng/dl), and DHEA-S of 401 mcg/dl (normal, 16–96 mcg/dl). Serum ACTH was less than 5 pg/ml (normal, 10–60 pg/ml)..")
68
Her weight at initial evaluation in our clinic at six months of age was 7.52 kg (60–75th percentile) and length was 59.1 cm (< 5th percentile). Blood pressure was 110/70 mmHg. Physical examination showed Cushingoid facies, buffalo hump, facial acne, and poor muscle tone (Figure 2). There were no signs of virilization. Family history was noncontributory. Physical examination of the patient revealed features of Cushing Syndrome including round facies, acne, plethora, central obesity, and poor muscle tone; she lacked clitoromegaly, hirsutism or other signs of virilization. An MRI of the abdomen showed a heterogeneous right adrenal mass measuring 3.6×5.4×3.8 cm; this mass was found to extend as a tumor thrombus into the inferior vena cava. The tumor thrombus appeared to extend to approximately 2 cm from the right atrium. There were no metastases seen in the liver or lungs on MRI. A Doppler ultrasound showed minimal, but present flow around the IVC tumor thrombus which measured 2.5×0.9×1 cm. Laboratory evaluation showed serum cortisol 70.8 mcg/dl (normal, 4.5–22.7 mcg/dl); aldosterone 4.2 ng/dl (normal 6.5–86.0 ng/dl); testosterone 59 ng/dl (normal, 6–77 ng/dl); ACTH <5 (normal, 10–60 pg/ml).
; aldosterone 4.2 ng/dl (normal 6.5–86.0 ng/dl); testosterone 59 ng/dl (normal, 6–77 ng/dl); ACTH <5 (normal, 10–60 pg/ml).")
69
Terima kasih

Presentasi serupa











>")




>")



