Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
DIAH PUSPITA RINI, dr., SpPK
TROMBOSIT / PLATELET DIAH PUSPITA RINI, dr., SpPK

2
Hematopoietic stem cell
FISIOLOGI Hematopoietic stem cell Megakaryoblast Megakaryocyte Fragmentation of cytoplasm Platelets

3
FISIOLOGI Trombosit merupakan fragmen sitoplasma megakariosit
Umur dalam sirkulasi darah 8 – 10 hari + 15% terpakai tiap hari Jumlah normal dlm sirkulasi /ml + 1/3 total massa trombosit terdapat dalam lien Berada dalam sirkulasi dalam keadaan “inaktif”

4
TROMBOPOIETIN Mengatur produksi trombosit
Mengatur jumlah dan kecepatan produksi trombosit Diproduksi di : - Liver - Ginjal

5
STRUKTUR TROMBOSIT MEMBRAN SEL MIKROTUBULUS SITOPLASMA

6
1. MEMBRAN SEL LIPID KARBOHIDRAT PROTEIN dan GLIKOPROTEIN
fosfolipid, kolesterol dan glikolipid KARBOHIDRAT PROTEIN dan GLIKOPROTEIN glikoprotein dan fosfolipid secara fungsional penting

7
GLIKOPROTEIN Mencegah trombosit melekat pada endotelium intak
Merupakan reseptor terhadap: ADP Trombin Fibrinogen Faktor Von Willebrand

8
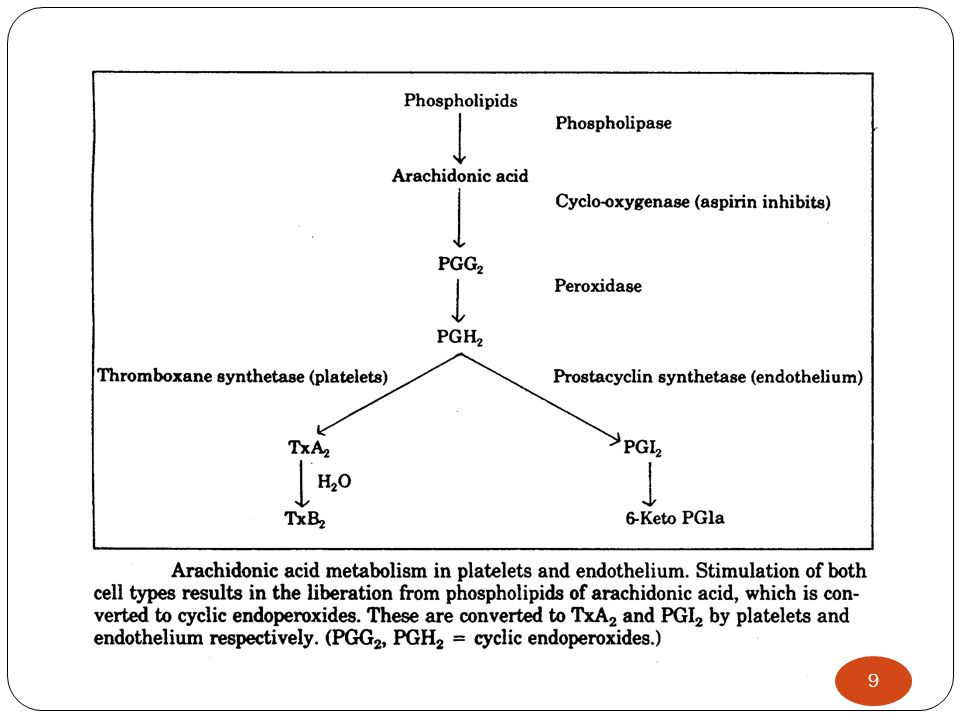
FOSFOLIPID - Mengaktivasi sistem koagulasi intrinsik
- Mengandung asam arakidonat (ArA) merupakan bahan baku untuk : -endoperoksidase siklik -tromboksan A2 (TxA2) merupakan Agonis agregasi trombosit
 merupakan bahan baku untuk : -endoperoksidase siklik. -tromboksan A2 (TxA2) merupakan Agonis agregasi trombosit.")
10
2. Mikrotubulus Terdiri dari protein polimer yang disebut tubulin
Tubulus membentuk dinding penyangga pada trombosit yang inaktif, untuk mempertahankan bentuk diskoid.

12
3. SITOPLASMA PROTEIN HORMON BAHAN LAIN Adrenalin
aktin, miosin,tromboastenin → kontraksi Fibrin-stabilizing factor Platelet derived growth factor (PDGF) HORMON Adrenalin Serotonin vascular and local tissue reactions Histamin BAHAN LAIN Calcium ions Mg- ions. Adenosine triphosphate (ATP) Adenosine diphosphate (ADP)
 HORMON. Adrenalin. Serotonin vascular and local tissue reactions. Histamin. BAHAN LAIN. Calcium ions. Mg- ions. Adenosine triphosphate (ATP) Adenosine diphosphate (ADP)")
13
FAAL HEMOSTASIS 1. Faal Koagulasi: berakhir dengan pembentukan fibrin stabil 2. Faal Fibrinolisis: berakhir dengan pembentukan plasmin

14
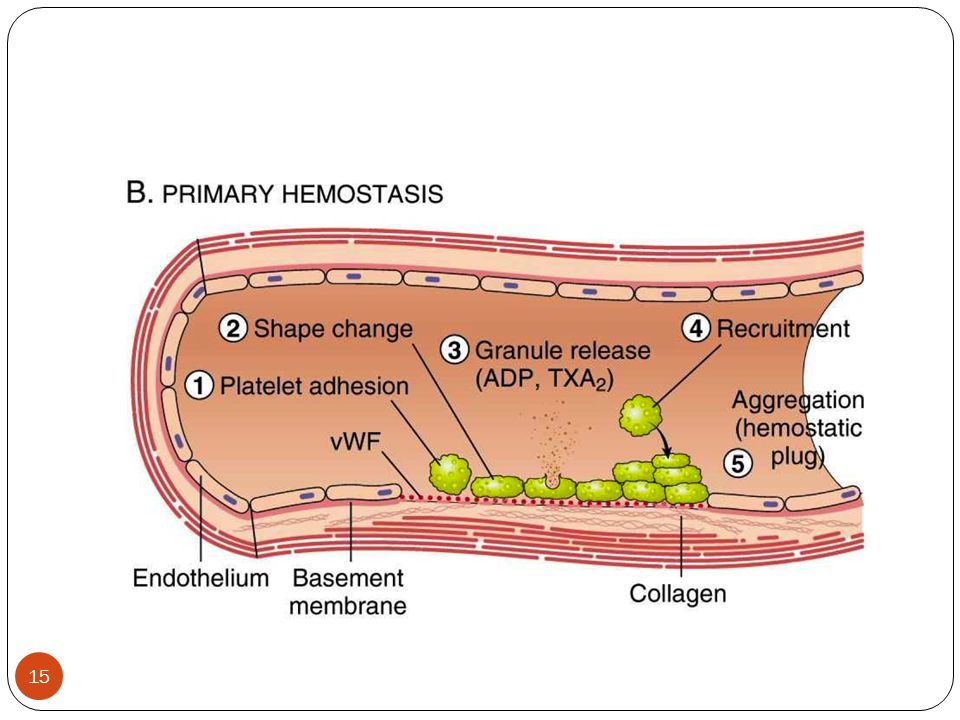
HEMOSTASIS PRIMER SEKUNDER FIBRINOLISIS
pembentukan sumbat trombosit/ “primary platelet plug” SEKUNDER pembentukan stable hemostatic plug (platelet+fibrin plug) FIBRINOLISIS
 FIBRINOLISIS.")
16
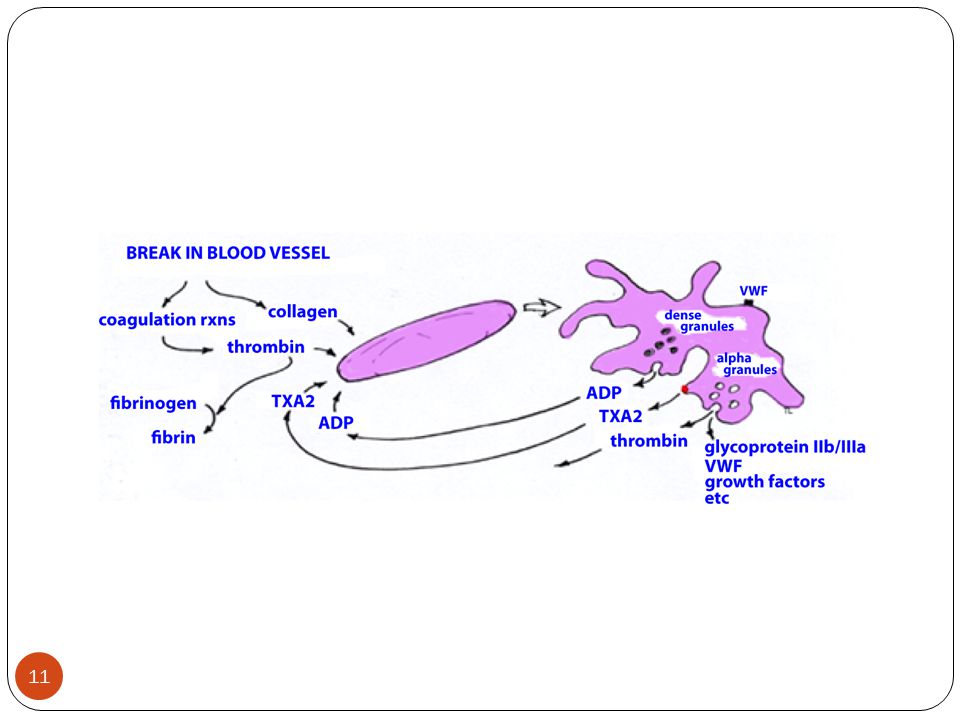
FUNGSI TROMBOSIT Membentuk sumbat trombosit/platelet plug sebagai respon terhadap kerusakan pembuluh darah Melalui mekanisme: 1. ADHESI 2. AKTIVASI 3. AGREGASI

17
ADHESI Trombosit menempel di kolagen subendotel
Proses ini bergantung pada: - faktor Von Willebrand - glikoprotein

18
AKTIVASI & AGREGASI Granula Sitoplasmik serotonin ADP dan
Thromboksan A2 Granula Sitoplasmik SEROTONIN → Vasokonstriktor ADP → menarik trombosit lain ke area luka TROMBOKSAN A2 → menyebabkan agregasi trombosit, degranulasi dan vasokonstriksi

19
endoperoksidase siklik, TxA2 & Trombin :
merangsang pelepasan ADP dari granula trombosit TxA2 , Trombin & ADP : aktivasi GP IIb – IIIa menjadi reseptor fibrinogen (FI) FI melekat pada GP IIb – IIIa trombosit yang berdekatan agregasi trombosit
 FI melekat pada GP IIb – IIIa trombosit yang. berdekatan agregasi trombosit.")
20
AGREGASI TROMBOSIT troMbosit trombosit trombosit trombosit trombosit
FI AGREGASI TROMBOSIT

21
KLINIS Adhesi dan agregasi trombosit berperan dalam penghentian primer terhadap pendarahan disebut “ PRIMARY HEMOSTASIS “ Defek Hemostasis Primer: Kelainan jumlah atau fungsi trombosit → perdarahan mukokutaneous : epistaxis, ecchymosis, perdarahan genitourinary atau perdarahan gingival

22
Disorders of platelets Disorders in the number of platelets
Functional Disorders (Qualitative)
")
23
A. GANGGUAN JUMLAH B. GANGGUAN FUNGSI 1. TROMBOSITOSIS
- trombositosis primer (Trombositosis esensial) - trombositosis sekunder (Trombositosis reaktif) 2. TROMBOSITOPENIA - penurunan produksi - peningkatan destruksi - gangguan distribusi B. GANGGUAN FUNGSI - gangguan adesi - gangguan agregasi
 - trombositosis sekunder (Trombositosis reaktif) 2. TROMBOSITOPENIA. - penurunan produksi. - peningkatan destruksi. - gangguan distribusi. B. GANGGUAN FUNGSI. - gangguan adesi. - gangguan agregasi.")
24
Trombositopenia

25
Trombositopenia : jumlah < 150.000/mm3
Penyebab : Penurunan produksi Peningkatan destruksi gangguan distribusi (sequestrasi) Bila tidak ada gangguan fungsi trombosit, ∑ – / ml → gejala klinik (-) Jumlah trombosit – / ml - pendarahan spontan ringan - pendarahan pasca operasi Jumlah trombosit /ml - pendarahan spontan, serius
 Bila tidak ada gangguan fungsi trombosit, ∑ – / ml. → gejala klinik (-) Jumlah trombosit – / ml. - pendarahan spontan ringan. - pendarahan pasca operasi. Jumlah trombosit /ml. - pendarahan spontan, serius.")
26
Thrombositopenia

27
Tipe trombositopenia Infection-Induced Thrombocytopenia
Drug-Induced Thrombocytopenia Heparin-Induced Thrombocytopenia Immune Thrombocytopenic Purpura (ITP) Inherited Thrombocytopenia Thrombotic Thrombocytopenic Purpura Hemolytic Uremic Syndrome
 Inherited Thrombocytopenia. Thrombotic Thrombocytopenic Purpura. Hemolytic Uremic Syndrome.")
28
TROMBOSITOPENIA Peningkatan Destruksi Trombosit
1. (Auto)immune Thrombocytopenic Purpura 2. Gangguan imunologis lain - pengaruh obat-obatan - SLE - penyakit limfoproliferatif - infeksi HIV 1 - pasca transfusi
immune Thrombocytopenic Purpura. 2. Gangguan imunologis lain. - pengaruh obat-obatan. - SLE. - penyakit limfoproliferatif. - infeksi HIV 1. - pasca transfusi.")
29
3. Non-imunologis - DIC - Septikemia bakterial - TTP + HUS - pengaruh etanol - pendarahan berat - toksemia - penyakit heriditer

30
TROMBOSITOPENIA … B. Gangguan Produksi - hipoplasia / aplasia sutul - invasi sel ganas ke sutul - sindroma dismielopoitik Gangguan Distribusi - hipersplenisme → pooling trombosit D. Akibat pengenceran (dilutional loss) akibat transfusi masif
 akibat transfusi masif.")
31
IDIOPATHIC THROMBOCYTOPENIC PURPURA (ITP)
Trombosit + autoantibodi Pembagian ITP: AKUT: sering pada anak, setelah inf.virus, sebagian besar sembuh spontan KRONIK: ♀ th, hilang timbul, jarang sembuh spontan PATOGENESIS: Trombosit dilapisi antibodi (IgG) Antibodi: Gp IIb – IIIa atau Ib → difagosit di RES → trombositopenia → kompensasi: peningkatan megakariosit di sutul
 Antibodi: Gp IIb – IIIa atau Ib → difagosit di RES → trombositopenia → kompensasi: peningkatan megakariosit di sutul.")
32
Gejala Klinik: Onset pelan: perdarahan kulit/mukosa, menorrhagia, perdarahan gusi, epistaksis Splenomegali pada 10% kasus Gambaran lab: Darah tepi: paling sering trombosit – Sumsum tulang: jumlah megakariosit meningkat disertai inti banyak (multinuclearity), lobulasi Imunologi: adanya antiplatelet IgG, lebih spesifik antibodi Gp IIb –IIIa atau Gp Ib
, lobulasi. Imunologi: adanya antiplatelet IgG, lebih spesifik antibodi Gp IIb –IIIa atau Gp Ib.")
33
The Classic Pentad of TTP
THROMBOTIC THROMBOCYTOPENIC PURPURA ( TTP ) dan HEMOLYTIC UREMIC SYNDROME ( HUS ) Sindroma akut dgn sistem organ multipel yang abnormal, anemia hemolitik mikroangiopati, trombositopenia The Classic Pentad of TTP Microangiopathic hemolytic anemia Thrombocytopenia Disfungsi organ: renal, CNS, others Neurologic abnormalities that can be fluctuating Fever
 dan HEMOLYTIC UREMIC SYNDROME ( HUS ) Sindroma akut dgn sistem organ multipel yang abnormal, anemia hemolitik mikroangiopati, trombositopenia. The Classic Pentad of TTP. Microangiopathic hemolytic anemia. Thrombocytopenia. Disfungsi organ: renal, CNS, others. Neurologic abnormalities that can be fluctuating. Fever.")
34
Patogenesis TTP Aktivitas yang menurun/ adanya inhibitor ADAMTS13 (A Disintegrin-like And Metalloprotease with ThromboSpondin type 1 motif 13) Suatu protease yang fungsinya memecah ULVWf (Unusually Large Von Willebrand factor) di sirkulasi
 di sirkulasi.")
35
Sadler, J. E. Hematology 2006;2006:415-420
Figure 5. Pathogenesis of idiopathic thrombotic thrombocytopenic purpura (TTP) caused by ADAMTS13 deficiency Figure 1. Pathogenesis of idiopathic thrombotic thrombocytopenic purpura (TTP) caused by ADAMTS13 deficiency Multimeric von Willebrand factor (VWF) adheres to endothelial cells or to connective tissue exposed in the vessel wall. Platelets adhere to the VWF through platelet membrane glycoprotein GPIb. In flowing blood, VWF in the platelet-rich thrombus is stretched and cleaved by the metalloprotease ADAMTS13, limiting thrombus growth. If ADAMTS13 is absent, VWF-dependent platelet accumulation continues, eventually causing microvascular thrombosis and TTP. Sadler, J. E. Hematology 2006;2006: Copyright ©2006 American Society of Hematology. Copyright restrictions may apply.
 caused by ADAMTS13 deficiency. Figure 1. Pathogenesis of idiopathic thrombotic thrombocytopenic purpura (TTP) caused by ADAMTS13 deficiency. Multimeric von Willebrand factor (VWF) adheres to endothelial cells or to connective tissue exposed in the vessel wall. Platelets adhere to the VWF through platelet membrane glycoprotein GPIb. In flowing blood, VWF in the platelet-rich thrombus is stretched and cleaved by the metalloprotease ADAMTS13, limiting thrombus growth. If ADAMTS13 is absent, VWF-dependent platelet accumulation continues, eventually causing microvascular thrombosis and TTP. Sadler, J. E. Hematology 2006;2006: Copyright ©2006 American Society of Hematology. Copyright restrictions may apply.")
36
HEMOLYTIC UREMIC SYNDROME
Lebih sering pada anak Klinis: anemia hemolitik mikroangiopatik trombositopenia gagal ginjal akut (uremia) Etiologi: E.coli 0157:H7 (Shiga like toxin) atau bakteri lain yang memproduksi eksotoksin Self limited, tanpa plasma exchange
 Etiologi: E.coli 0157:H7 (Shiga like toxin) atau bakteri lain yang memproduksi eksotoksin. Self limited, tanpa plasma exchange.")
37
Adapted from Veyradier, A, et al. Blood 2001; 98:1765.
TTP HUS NUMBER OF SUBJECTS 66 45 Hemolytic Anemia 100 Thrombocytopenia 94 60 Neurologic changes 90 15 Acute Renal Failure 2 98 Fever 50 21 Adapted from Veyradier, A, et al. Blood 2001; 98:1765.

38
TTP and HUS: different entities
Several (E.Coli 0157:H7) Causative agent None identified Epidemics No Yes GI prodrome Uncommon Often Children affected Rare Often Relapses Common Rare Renal impairment Usually mild Often severe Severe thrombocytopenia Often Rare Incr UL-VWF multimers Yes No Antibodies to metalloproteinase Yes No BUT: TTP cannot be reliably distinguished from HUS at time of presentation in many cases
 Causative agent. None identified. Epidemics. No. Yes. GI prodrome. Uncommon. Often. Children affected. Rare. Often. Relapses. Common. Rare. Renal impairment. Usually mild. Often severe. Severe thrombocytopenia. Often. Rare. Incr UL-VWF multimers. Yes. No. Antibodies to metalloproteinase. Yes. No. BUT: TTP cannot be reliably distinguished from HUS at time of presentation in many cases.")
39
Diagnosis Fragmentosit/schistosit pada hapusan darah tepi
Trombositopenia Fragmentosit/schistosit pada hapusan darah tepi LDH (laktat dehodrogenase) Haptoglobin menurun ADAMTS13 (pada TTP) Rule out other cause of microangiopathy: pregnancy, cancer, DIC
 Haptoglobin menurun. ADAMTS13 (pada TTP) Rule out other cause of microangiopathy: pregnancy, cancer, DIC.")
40
Gambaran hapusan darah tepi pada penderita HUS.
Banyak terdapat Schistocytes (Marler Clark, 2006)
")
41
TROMBOSITOPENIA HERIDITER
Wiskott-Aldrich syndrome - trombositopenia berat - ukuran trombosit kecil-kecil - respon baik terhadap splenektomi - sifat x-Linked resesif 2. Bernard-Soulier syndrome - autosomal resesif - “giant” trombosyte (+) - defisiensi GP Ib → gangguan fungsi May-Hegglin anomaly - autosomal dominant - giant thrombocyte (+) - dohle bodies (+)
 - defisiensi GP Ib → gangguan fungsi. May-Hegglin anomaly. - autosomal dominant. - giant thrombocyte (+) - dohle bodies (+)")
42
-Elevated Liver enzyme, -Low Platelet count.
TROMBOSITOPENIA PADA TOKSEMIA . 15 – 20 % TOXAEMIA GRAVIDARUM . sering disertai dengan - anemia hemolitik mikroangiopatik - peningkatan enzim-enzim hati disebut : HELLP Syndrome -Hemolysis -Elevated Liver enzyme, -Low Platelet count.

43
Differential diagnosis of thrombocytopenia
Differential diagnosis of thrombocytopenia. Evaluation of thrombocytopenia is best organized according to the apparent defect in platelet production, distribution, or destruction.

44
Algorithm for thrombcytopenia evaluation

45
Increased Platelet Destruction
Thrombositosis Increased Platelet Destruction The hallmark of increased platelet destruction is increased marrow megakaryocytes or, when available, high reticulated platelet count. Platelet destruction results from various immune conditions, including the following: Immune thrombocytopenic purpura (ITP) Thrombotic microangiopathies Post-transfusion purpura (PTP) Heparin-induced thrombocytopenia (HIT) Disseminated intravascular coagulation (DIC)
 Thrombotic microangiopathies. Post-transfusion purpura (PTP) Heparin-induced thrombocytopenia (HIT) Disseminated intravascular coagulation (DIC)")
46
TROMBOSITOSIS PRIMER Trombositosis (trombositemia) esensial
merupakan bagian penyakit mieloproliferatif Kriteria diagnosis: - tidak ada bukti penyebab trombositosis reaktif - jumlah trombo > /ml pd 2 x pemeriksaan - splenomegali (50-65% kasus) - Hb, PCV, massa eritrosit normal - cadangan besi dalam Sutul cukup - Philadelphia Kromosom + - fibrosis Sutul + /minimal
 - Hb, PCV, massa eritrosit normal. - cadangan besi dalam Sutul cukup. - Philadelphia Kromosom + - fibrosis Sutul + /minimal.")
47
TROMBOSITOSIS PRIMER w Hematologi :
jumlah trombo > /ml ( sering > 1 juta/uL) pada 2 x pemeriksaan Hb, PCV, massa eritrosit normal lekositosis > /mL (25-40%) gangguan agregasi trombosit dengan agonis :adrenalin, ADP, trombin sutul hiperseluler : Megakaryosit Fibrosis minimal / +
 pada 2 x pemeriksaan. Hb, PCV, massa eritrosit normal. lekositosis > /mL (25-40%) gangguan agregasi trombosit dengan agonis :adrenalin, ADP, trombin. sutul hiperseluler : Megakaryosit. Fibrosis minimal / +")
48
PENYEBAB TROMBOSITOSIS REAKTIF
post Splenektomi defisiensi besi khronik penyakit neoplastik infeksi / inflamasi khronik pasca operasi penyakit mieloproliferatif lain (Polisitemia vera, CML)
")
49
Hapusan darah tepi trombositosis

50
Increased Platelet Destruction
Kelainan Fungsi Trombosit Increased Platelet Destruction The hallmark of increased platelet destruction is increased marrow megakaryocytes or, when available, high reticulated platelet count. Platelet destruction results from various immune conditions, including the following: Immune thrombocytopenic purpura (ITP) Thrombotic microangiopathies Post-transfusion purpura (PTP) Heparin-induced thrombocytopenia (HIT) Disseminated intravascular coagulation (DIC)
 Thrombotic microangiopathies. Post-transfusion purpura (PTP) Heparin-induced thrombocytopenia (HIT) Disseminated intravascular coagulation (DIC)")
51
Congenital disorders of platelet function
Von Willebrand Disease Glanzmann’s Thrombasthenia Bernard-soulier Syndrome

52
GANGGUAN FUNGSI TROMBOSIT
I. KONGENITAL - riwayat pendarahan muko-kutaneus: epistaksis, menoragia, pendarahan gusi dll - jumlah dan ukuran trombosit : normal - tes penyaring koagulasi plasma : normal contoh : - Bernard – Soulier Syndrom: Gp.Ib (-) - von Willebrand’s disease : vWf (-) - tromboastenia Glanzman : Gp IIb-IIIa (-)
 - von Willebrand’s disease : vWf (-) - tromboastenia Glanzman : Gp IIb-IIIa (-)")
53
Gp IIb-IIIa complex on platelet surface

54
Gp Ib receptor on platelets

55
* pada Mielofibrosis : kelainan membran & granula trombosit
DAPATAN 1. Penyakit mieloproliferatif * kecenderungan pendarahan ada hubungan dengan trombositosis gbila jumlah trombosit di i g pendarahani * pada Mielofibrosis : kelainan membran & granula trombosit * Agregasi abnormal terhadap epinefrin, ADP & kolagen 2. Uremia * gangguan agregasi terhadap epinefrin, ADP & kolagen

56
3. Pintas jantung – paru (cardiopulmonary bypass)
* menyebabkan trombositopenia dan kerusakan granula-granula trombosit. 4. Obat-obatan * asetosal ,NSAID dosis kecil gangguan sintesis endoperoksidase

57
PLATELET Function TESTS
Capillary Resistance Test - test of Hess - tourniquet test - Rumple-Leede’s test Bleeding Time - with & without aspirin Clot Retraction Platelet Adhesion Platelet Aggregation Antiplatelet Antibody

58
END OF TODAY LECTURE

59
REFERENCE al, F. e. (2008). Harrison's Principles of Internal Medicine, 17th Edition. USA: The McGraw-Hill Companies, Inc Clark M, LLP, PS. About Hemolytic Uremic Syndrome (HUS). Columbia : Outbreak, Inc; 2005 p 1-4. Hematology TTP and ADAMTS13: When is testing appropriate? Mannucci et al Hematology 2006.Thrombocytopenic Purpura:A moving Target. Sadler Kumar, V., Abbas, A. K., Fausto, N., & Mitchell, R. N. (2007). Robbin's Basic Pathology 8th Edition.Philadelphia, PA: Saunders Elsevier Veyradier, A, et al. Specific von Willebrand factor-cleaving protease in thrombotic microangiopathies: a study of 111 cases. Blood 2001; 98:1765.
. Columbia : Outbreak, Inc; 2005 p 1-4. Hematology TTP and ADAMTS13: When is testing appropriate Mannucci et al. Hematology 2006.Thrombocytopenic Purpura:A moving Target. Sadler. Kumar, V., Abbas, A. K., Fausto, N., & Mitchell, R. N. (2007). Robbin s Basic Pathology 8th Edition.Philadelphia, PA: Saunders Elsevier. Veyradier, A, et al. Specific von Willebrand factor-cleaving protease in thrombotic microangiopathies: a study of 111 cases. Blood 2001; 98:1765.")
Presentasi serupa










, mencakup.>")








