Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
ADVANCED CARDIAC LIFE SUPPORT

4
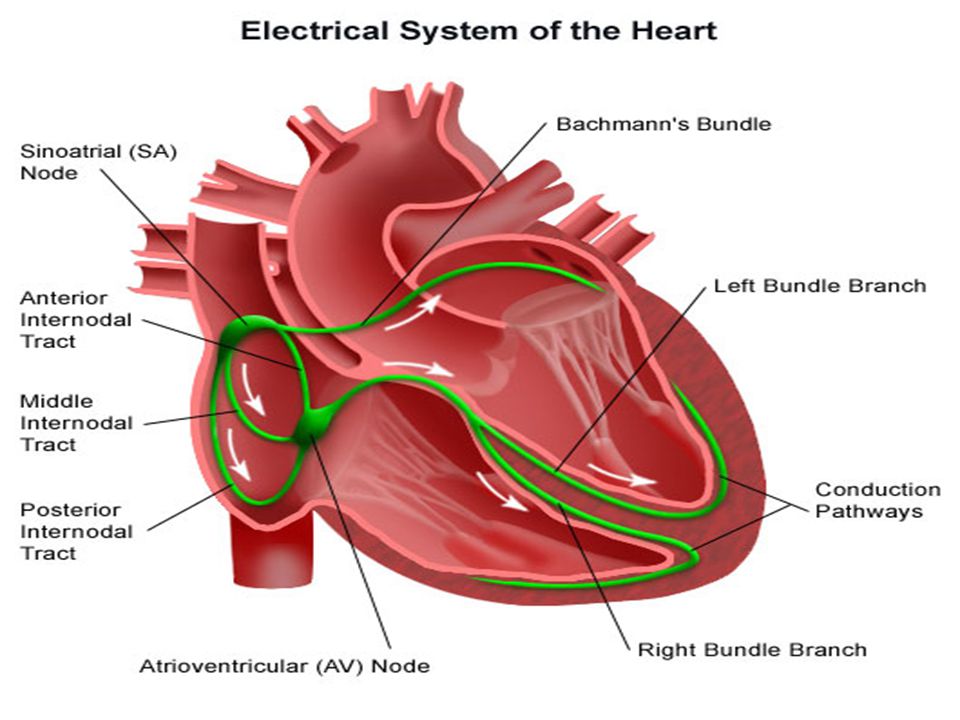
SA NODE: IRAMA SINUS AV NODE: IRAMA JUNCTIONAL SERABUT PURKINJE: IRAMA IDIOVENTRIKULAR

5
90 % pasien henti jantung dengan ventrikel fibrilasi dan ventrikel takikardi tanpa nadi
Indonesia Raya ACLS: cek nadi, cek napas, cek Bp. (dilakukan setiap dua menit, atau perubahan EKG)
")
6
UNORGANIZED RHYTM Ventrikel fibrilasi (coarse, fine) Asystole
JANGAN CEK NADI

7
ALGORITME NADI NEGATIVE (-) NADI POSITIVE (-)
 NADI POSITIVE (-)")
8
NADI NEGATIVE VENTRIKEL FIBRILASI DAN VENTRIKEL TAKIKARDI TANPA NADI (-) PEA Sinus rhytm Sinus bradicardi Sinus takikardi Junctional rthym IVR AVB etc

9
ASYSTOLE Flat

10
NADI POSITIVE BRADIKARDI
SINUS BRADIKARDI JUNCTIONAL RHYTM IVR AVB

11
TAKIKARDI SVT VT MAT JT Af AF

12
Electrocardiographic Paper
The electrocardiogram (ECG) strip is printed on graph paper, with each small block measuring 1 mm in height and width. ECG recorders and monitors are standardized at a speed of 25 mm/sec. Time is measured on the horizontal axis. At this speed, each small block represents 0.04 second. Five small blocks make up one large block = 0.20 second.
 strip is printed on graph paper, with each small block measuring 1 mm in height and width. ECG recorders and monitors are standardized at a speed of 25 mm/sec. Time is measured on the horizontal axis. At this speed, each small block represents 0.04 second. Five small blocks make up one large block = 0.20 second.")
13
Five large blocks, represent 1 second, and 30 large blocks represent 6 seconds.

14
Normal Components of the EKG Waveform
EKG paper is a grid where time is measured along the horizontal axis. Each small square is 1 mm in length and represents 0.04 seconds. Each larger square is 5 mm in length and represents 0.2 seconds. Voltage is measured along the vertical axis. 10 mm is equal to 1mV in voltage.

15
P wave Indicates atrial depolarization Normal duration is not longer than 0.12 seconds Amplitude (height) is no more than 3 mm No notching or peaking QRS complex Indicates ventricular depolarization Normally 0.06 – 0.12 seconds in duration R waves are deflected positively and the Q and S waves are negative Q pathologis = > 25 % tall R

16
T wave Indicates ventricular repolarization Not more that 5 mm in amplitude in standard leads and 10 mm in precordial leads Rounded and asymmetrical ST segment Normally not depressed more than 0.5 mm May be elevated slightly in some leads (no more than 1 mm)
")
17
Measured from the Q to the end of the T.
PR interval Indicates AV conduction time Duration time is 0.12 to 0.20 seconds QT interval Measured from the Q to the end of the T. Represents ventricular depolarization and repolarization (sodium influx and potassium efflux) QT usually less than half the R-R interval
 QT usually less than half the R-R interval.")
18
Electrocardiographic Analysis
Determine the heart rate if the rhythms are irregular, the nurse must use the 6 second strip method for accuracy.

19
Irregular 6 second = 30 big blocks 5 second = 25 big blocks

20
Regullar 1500 small blocks R-R 300 big blocks R-R Memorization

21
5 big blocks = 60 6 big blocks = 50 7 big blocks = 43 8 big blocks = 37 9 big blocks = 33 10 big blocks = 30

22
Analyze the P waves Measure the P-R Interval Measure the QRS duration Interpret the rhythm

23
NORMAL SINUS RHYTHM Irama = Teratur
Frekuensi (HR) = 60 – 100 kali/menit Gelombang P = Normal ( + di L II dan – di aVR), P : QRS = 1:1 Interval PR = 0,12 – 0,20 detik Lebar Gelombang QRS = Tidak lebih dari 0,12 detik (sempit)
 = 60 – 100 kali/menit. Gelombang P = Normal ( + di L II dan – di aVR), P : QRS = 1:1. Interval PR = 0,12 – 0,20 detik. Lebar Gelombang QRS = Tidak lebih dari 0,12 detik (sempit)")
24
SINUS BRADYCARDIA Irama = Teratur Frekuensi (HR) = < 60 kali/menit
Gelombang P = Normal ( + di L II dan – di aVR), P : QRS = 1:1 Interval PR = 0,12 – 0,20 detik Lebar Gelombang QRS = Tidak lebih dari 0,12 detik (sempit) Dominance of parasymphatetic nervous system,excessive vagal stimulation may result from carotid sinus massage, vomiting, suctioning, valsava maneuvers (e.g., bearing down for a bowel movement or gagging), ocular pressure or pain. Sinus bradycardia may also result from hypoxia, inferior wall MI, and the admnistration of drugs such as beta-adrenergic blocking agents, calcium channel blockers, and digitalis
, P : QRS = 1:1. Interval PR = 0,12 – 0,20 detik. Lebar Gelombang QRS = Tidak lebih dari 0,12 detik (sempit) Dominance of parasymphatetic nervous system,excessive vagal stimulation may result from carotid sinus massage, vomiting, suctioning, valsava maneuvers (e.g., bearing down for a bowel movement or gagging), ocular pressure or pain. Sinus bradycardia may also result from hypoxia, inferior wall MI, and the admnistration of drugs such as beta-adrenergic blocking agents, calcium channel blockers, and digitalis.")
25
SINUS TACHYCARDIA Irama = Teratur
Frekuensi (HR) = 100 – 150 kali/menit Gelombang P = Normal ( + di L II dan – di aVR), P : QRS = 1:1 Interval PR = 0,12 – 0,20 detik Lebar Gelombang QRS = Tidak lebih dari 0,12 detik (sempit) Dominant sympathetic nervous system stimulation of the heart or vagal inhibition. Increase physical activity but may also be cuased by anxiety, pain, stress, fear, fever, anemia, hypoxemia, hyperthyroidism, and pulmonary embolism. Drugs: catecholamines, atropine, caffeine, alcohol, nicotine, aminophylline, and thryroid medications may also increase the heart rate, in some cases, sinus tachycardia is a compensatory response to decreased cardiac output or blood pressure, as occurs in hypovolemia, shock, myocardial infarction (MI), and heart failure.
 = 100 – 150 kali/menit. Gelombang P = Normal ( + di L II dan – di aVR), P : QRS = 1:1. Interval PR = 0,12 – 0,20 detik. Lebar Gelombang QRS = Tidak lebih dari 0,12 detik (sempit) Dominant sympathetic nervous system stimulation of the heart or vagal inhibition. Increase physical activity but may also be cuased by anxiety, pain, stress, fear, fever, anemia, hypoxemia, hyperthyroidism, and pulmonary embolism. Drugs: catecholamines, atropine, caffeine, alcohol, nicotine, aminophylline, and thryroid medications may also increase the heart rate, in some cases, sinus tachycardia is a compensatory response to decreased cardiac output or blood pressure, as occurs in hypovolemia, shock, myocardial infarction (MI), and heart failure.")
26
SINUS ARRYTHMIA Irama = Tidak Teratur
Frekuensi (HR) = Umumnya 60 – 100 kali/menit, dapat juga < 60 atau > 100 kali/menit Gelombang P = Normal ( + di L II dan – di aVR), P : QRS = 1:1 Interval PR = 0,12 – 0,20 detik Lebar Gelombang QRS = Tidak lebih dari 0,12 detik (sempit) Sinus arrhythmia is a variant of NSR. It results from changes in intrathoracic pressure during breathing. The heart rate increases slightly during inspiration an ddecreases slightly during exhalation. This irregular rhytm is frequently observed in healthy children as well as adults.
 = Umumnya 60 – 100 kali/menit, dapat juga < 60 atau > 100 kali/menit. Gelombang P = Normal ( + di L II dan – di aVR), P : QRS = 1:1. Interval PR = 0,12 – 0,20 detik. Lebar Gelombang QRS = Tidak lebih dari 0,12 detik (sempit) Sinus arrhythmia is a variant of NSR. It results from changes in intrathoracic pressure during breathing. The heart rate increases slightly during inspiration an ddecreases slightly during exhalation. This irregular rhytm is frequently observed in healthy children as well as adults.")
27
ATRIAL EKSTRASISTOL Irama = Tidak Teratur karena ada irama Ekstrasistol Frekuensi (HR) = Tergantung Irama dasarnya Gelombang P = Timbulnya lebih awal dan bentuknya berbeda dengan bentuk gelombang irama dasarnya Interval PR = Bervariasi antara 0,12 – 0,20 detik, atau <0,12 detik jika sumber ekstrasistolnya di atrium bawah Lebar Gelombang QRS = Tidak lebih dari 0,12 detik (sempit) A premature atrial complex (PAC) occurs when atrial tissue becomes irritable. This ectopic focus fires an impulse before the next sinus impulse is due, thus usurping the sinus pacemaker. The premature P wave from the atrial focus is early and has shape different from that of the P wave generated from the sinus node. The causes: fatigue; anxiety; inflammation; infection; intake of caffeine, nicotine, or alcohol; and the administration of drugs suh as catecholamine, sympathomimetics, amphetamines, digitalis, or anesthetic agents. PACs may also resutls from myocardial ischemia, hypermetabolic states, electrolyte imbalance, or atrial strecth, as may occur with congestive heart failure, valvular disease, and pulmonary hypertension with cor pulmonale.
 A premature atrial complex (PAC) occurs when atrial tissue becomes irritable. This ectopic focus fires an impulse before the next sinus impulse is due, thus usurping the sinus pacemaker. The premature P wave from the atrial focus is early and has shape different from that of the P wave generated from the sinus node. The causes: fatigue; anxiety; inflammation; infection; intake of caffeine, nicotine, or alcohol; and the administration of drugs suh as catecholamine, sympathomimetics, amphetamines, digitalis, or anesthetic agents. PACs may also resutls from myocardial ischemia, hypermetabolic states, electrolyte imbalance, or atrial strecth, as may occur with congestive heart failure, valvular disease, and pulmonary hypertension with cor pulmonale.")
28
SUPRAVENTRIKEL TAKIKARDIA (SVT)
Irama = Teratur Frekuensi (HR) = > 150 kali/menit Gelombang P = Terlihat kecil, kadang tidak ada Interval PR = Memendek atau tidak ada Lebar Gelombang QRS = Tidak lebih dari 0,12 detik (sempit) SVT, involves the rapid stimulation of atrial tissue at a rate of 100 to 280 beats/min. SVT is most often due to a re-entry mechanism in which one impulse circulates repeatedly throughout the atrial pathway, restimulating the atrail tissue at a rapid rate. During SVT the P waves have a shape different from that of sinus P wave. The P waves may not be visible, especially if there is a 1:1 conduction with rapid rates because the P waves are emebedded in the preceding T wave. The causes of SVT are the same as those PACs.
 = > 150 kali/menit. Gelombang P = Terlihat kecil, kadang tidak ada. Interval PR = Memendek atau tidak ada. Lebar Gelombang QRS = Tidak lebih dari 0,12 detik (sempit) SVT, involves the rapid stimulation of atrial tissue at a rate of 100 to 280 beats/min. SVT is most often due to a re-entry mechanism in which one impulse circulates repeatedly throughout the atrial pathway, restimulating the atrail tissue at a rapid rate. During SVT the P waves have a shape different from that of sinus P wave. The P waves may not be visible, especially if there is a 1:1 conduction with rapid rates because the P waves are emebedded in the preceding T wave. The causes of SVT are the same as those PACs.")
29
MULTIFOKAL ATRIAL TAKIKARDI
Irama = Tidak Teratur Frekuensi (HR) = >100 kali/menit Gelombang P = Kadang terlihat besar, kadang kecil (berubah bentuk) Interval PR = Memendek Lebar Gelombang QRS = Tidak lebih dari 0,12 detik (sempit)
 = >100 kali/menit. Gelombang P = Kadang terlihat besar, kadang kecil (berubah bentuk) Interval PR = Memendek. Lebar Gelombang QRS = Tidak lebih dari 0,12 detik (sempit)")
30
ATRIAL FLUTTER Irama = Umumnya teratur dapat juga tidak teratur
Frekuensi (HR) = Frekuensi atrium 250 – 350 kali/menit Frekuensi ventrikel bervariasi. Jika HR < 60 X/mnt disebut slow response Jika HR 60 – 100 X/mnt disebut normo response Jika HR > 100 X/mnt disebut rapid response Gelombang P = Terlihat banyak seperti “gigi gergaji” Atrail flutter is rapid atrial depolarization occurring at a rate of 250 to 350 times per minute. Atrial flutter may be cuased by rheumatic or ischemic heart disease, heart failure (CHF), AV valve disease, pre-excitation syndromes, septal defects, pulmonary emboli, thyrotoxicosis, alcoholism, or pericarditis.
 = Frekuensi atrium 250 – 350 kali/menit. Frekuensi ventrikel bervariasi. Jika HR < 60 X/mnt disebut slow response. Jika HR 60 – 100 X/mnt disebut normo response. Jika HR > 100 X/mnt disebut rapid response. Gelombang P = Terlihat banyak seperti gigi gergaji Atrail flutter is rapid atrial depolarization occurring at a rate of 250 to 350 times per minute. Atrial flutter may be cuased by rheumatic or ischemic heart disease, heart failure (CHF), AV valve disease, pre-excitation syndromes, septal defects, pulmonary emboli, thyrotoxicosis, alcoholism, or pericarditis.")
31
ATRIAL FLUTTER Interval PR = Tidak dapat dihitung
Lebar Gelombang QRS = Tidak lebih dari 0,12 detik (sempit), dapat juga lebar jika disertai adanya blok interventrikuler
, dapat juga lebar jika disertai adanya blok interventrikuler.")
32
ATRIAL FIBRILASI Irama = Tidak Teratur
Frekuensi (HR) = Frekuensi atrium > 350 kali/menit Frekuensi ventrikel bervariasi. Jika HR < 60 X/mnt disebut slow response Jika HR 60 – 100 X/mnt disebut normo response Jika HR > 100 X/mnt disebut rapid response Multiple rapid impulses from many atrial foci, at a rate of 350 to 600 times per minute, depolarize the atrial in a totally disorganized manner. The result is chaos, with no P waves, no atrail contractions, loss of the atrial kick, and an irregular ventricular response. Dilation and blood stagnation in the atrial can lead to thrombus formationk and this increases the risk of stroke or other embolic events. In addition, AF causes a decrease in cardiac output, further compromising the hearts’s perfusion ability. It also occur in clients with the following conditions: MI, rheumatic heart disease with mitral stenosis, atrial septal defect, heart failure, cardiomyopathy, hyperthyroidism, pulmonary emboli WPW, congenital heart disease and chronic constrictive pericarditis.
 = Frekuensi atrium > 350 kali/menit. Frekuensi ventrikel bervariasi. Jika HR < 60 X/mnt disebut slow response. Jika HR 60 – 100 X/mnt disebut normo response. Jika HR > 100 X/mnt disebut rapid response. Multiple rapid impulses from many atrial foci, at a rate of 350 to 600 times per minute, depolarize the atrial in a totally disorganized manner. The result is chaos, with no P waves, no atrail contractions, loss of the atrial kick, and an irregular ventricular response. Dilation and blood stagnation in the atrial can lead to thrombus formationk and this increases the risk of stroke or other embolic events. In addition, AF causes a decrease in cardiac output, further compromising the hearts’s perfusion ability. It also occur in clients with the following conditions: MI, rheumatic heart disease with mitral stenosis, atrial septal defect, heart failure, cardiomyopathy, hyperthyroidism, pulmonary emboli. WPW, congenital heart disease and chronic constrictive pericarditis.")
33
ATRIAL FIBRILASI Gelombang P = Tidak dapat diidentifikasi, bahkan kadang seperti garis lurus Interval PR = Tidak dapat dihitung Lebar Gelombang QRS = Tidak lebih dari 0,12 detik (sempit), dapat juga lebar jika disertai blok interventrikuler
, dapat juga lebar jika disertai blok interventrikuler.")
34
JUNCTIONAL EKSTRASISTOL (JES)
Irama = Tidak teratur karena ada irama Ekstrasistol Frekuensi (HR) = Tergantung Irama dasarnya Gelombang P = Ada tapi kadang tidak terlihat, jika ada, timbul sesudah gelombang QRS, dan bentuknya akan terbalik (negatif) di L II dan positif di L aVR Interval PR = Memendek atau tidak dapat diukur Lebar Gelombang QRS = Tidak lebih dari 0,12 detik (sempit)
 = Tergantung Irama dasarnya. Gelombang P = Ada tapi kadang tidak terlihat, jika ada, timbul sesudah gelombang QRS, dan bentuknya akan terbalik (negatif) di L II dan positif di L aVR. Interval PR = Memendek atau tidak dapat diukur. Lebar Gelombang QRS = Tidak lebih dari 0,12 detik (sempit)")
35
JUNCTIONAL RHYTHM Irama = Teratur Frekuensi (HR) = 40 – 60 kali/menit
Gelombang P = Ada, kadang tidak terlihat, jika terlihat, timbul sebelum atau sesudah gelombang QRS Interval PR = Memendek atau tidak dapat diukur Lebar Gelombang QRS = Tidak lebih dari 0,12 detik (sempit) These rhytms are most commonly transient, and clients usually remain hemodynamically stable. The junctional rhythm initiates within the AV nodal tissue. Accelerated junctional rhythm is a result of enhanced automaticity of the AVN that supersedes the sinus node rate. During this rhythm, the AVN is firing faster than the sinus node, resulting in a regular narrow complex rhythm. These rhythms may demonstrate retrograde P waves on ECG findings, and the rates can vary from beats per minute. Sick sinus syndrome (including drug-induced) Digoxin toxicity Ischemia of the AVN, especially with acute inferior infarction Acutely after cardiac surgery, especially in children within 4 days after surgery for congenital cardiac defects Acute inflammatory processes (eg, acute rheumatic fever), which may involve the conduction system Diphtheria Other drugs (eg, beta-blockers, calcium blockers, most antiarrhythmic agents) that cause sinus bradycardia Metabolic states with increased adrenergic tone Isoproterenol infusion
 These rhytms are most commonly transient, and clients usually remain hemodynamically stable. The junctional rhythm initiates within the AV nodal tissue. Accelerated junctional rhythm is a result of enhanced automaticity of the AVN that supersedes the sinus node rate. During this rhythm, the AVN is firing faster than the sinus node, resulting in a regular narrow complex rhythm. These rhythms may demonstrate retrograde P waves on ECG findings, and the rates can vary from beats per minute. Sick sinus syndrome (including drug-induced) Digoxin toxicity. Ischemia of the AVN, especially with acute inferior infarction. Acutely after cardiac surgery, especially in children within 4 days after surgery for congenital cardiac defects. Acute inflammatory processes (eg, acute rheumatic fever), which may involve the conduction system. Diphtheria. Other drugs (eg, beta-blockers, calcium blockers, most antiarrhythmic agents) that cause sinus bradycardia. Metabolic states with increased adrenergic tone. Isoproterenol infusion.")
36
ACCELERATED JUNCTIONAL RHYTHM
Irama = Teratur Frekuensi (HR) = 60 – 100 kali/menit Gelombang P = Ada, tapi kadang tidak terlihat, jika terlihat ada di depan, di tengah, atau dibelakang gelombang QRS Interval PR = Memendek atau tidak dapat diukur Lebar Gelombang QRS = Tidak lebih dari 0,12 detik (sempit)
 = 60 – 100 kali/menit. Gelombang P = Ada, tapi kadang tidak terlihat, jika terlihat ada di depan, di tengah, atau dibelakang gelombang QRS. Interval PR = Memendek atau tidak dapat diukur. Lebar Gelombang QRS = Tidak lebih dari 0,12 detik (sempit)")
37
JUNCTIONAL TAKIKARDI Irama = Teratur
Frekuensi (HR) = > 100 kali/menit Gelombang P = Ada, tapi kadang tidak terlihat, jika terlihat ada di depan, di tengah, atau dibelakang gelombang QRS Interval PR = Memendek atau tidak dapat diukur Lebar Gelombang QRS = Tidak lebih dari 0,12 detik (sempit)
 = > 100 kali/menit. Gelombang P = Ada, tapi kadang tidak terlihat, jika terlihat ada di depan, di tengah, atau dibelakang gelombang QRS. Interval PR = Memendek atau tidak dapat diukur. Lebar Gelombang QRS = Tidak lebih dari 0,12 detik (sempit)")
38
VENTRIKEL EKSTRASISTOL (VES)
Irama = Tidak teratur karena ada irama Ekstrasistol Frekuensi (HR) = Tergantung irama dasarnya Gelombang P = Tidak ada Interval PR = Tidak ada Lebar Gelombang QRS = > 0,12 detik (Lebar) MI, CHF, chronic hypoxemia, chronic airway limitation , anemia, hypokalemia, or hypomagnesemia. The administration of catecholamines, symphathomimetics drugs, and digitalis, as well as acidosis, anesthesia, stress, nicotine intake, ingestion of caffeine and alcohol, infection, trauma, or surgeryu, can also cause PVCs. Postmenopausal women often find that caffeine causes palpitations and PVCs.
 = Tergantung irama dasarnya. Gelombang P = Tidak ada. Interval PR = Tidak ada. Lebar Gelombang QRS = > 0,12 detik (Lebar) MI, CHF, chronic hypoxemia, chronic airway limitation , anemia, hypokalemia, or hypomagnesemia. The administration of catecholamines, symphathomimetics drugs, and digitalis, as well as acidosis, anesthesia, stress, nicotine intake, ingestion of caffeine and alcohol, infection, trauma, or surgeryu, can also cause PVCs. Postmenopausal women often find that caffeine causes palpitations and PVCs.")
39
VES BIGEMINY

40
VES UNIFOKAL

41
VES MULTIFOKAL

42
VES CONSECUTIF (SALVO)
")
43
IDIOVENTRICULAR RHYTHM (IVR)
Irama = Teratur Frekuensi (HR) = 20 – 40 kali/menit Gelombang P = Tidak ada Interval PR = Tidak ada Lebar Gelombang QRS = > 0,12 detik (Lebar) The ventricular nodal cells pace the ventricles. If P waves are seen, they are independent of the QRS complexes and are nto related. Idioventricular rhythm is seen as a rhythm in the dy;ing heart, where downward displacement of the pacemaker has occurred. PEA is characterized by no palpable pulse and therefore no perfusion, although electrical activity is displayed on the monitor. Common causes of PEA are hypovolemia, hypoxia, acidosis, hyperkalemia, or hypokalemia, hypothermia, drug overdose, tension pneumothorax, coronary or pulmonary thrombosis, and cardiac tamponade.
 = 20 – 40 kali/menit. Gelombang P = Tidak ada. Interval PR = Tidak ada. Lebar Gelombang QRS = > 0,12 detik (Lebar) The ventricular nodal cells pace the ventricles. If P waves are seen, they are independent of the QRS complexes and are nto related. Idioventricular rhythm is seen as a rhythm in the dy;ing heart, where downward displacement of the pacemaker has occurred. PEA is characterized by no palpable pulse and therefore no perfusion, although electrical activity is displayed on the monitor. Common causes of PEA are hypovolemia, hypoxia, acidosis, hyperkalemia, or hypokalemia, hypothermia, drug overdose, tension pneumothorax, coronary or pulmonary thrombosis, and cardiac tamponade.")
44
ACCELERATED IDIOVENTRIKULAR RHYTM
Irama = Teratur Frekuensi (HR) = 40 – 100 kali/menit Gelombang P = Tidak ada Interval PR = Tidak ada Lebar Gelombang QRS = > 0,12 detik (Lebar)
 = 40 – 100 kali/menit. Gelombang P = Tidak ada. Interval PR = Tidak ada. Lebar Gelombang QRS = > 0,12 detik (Lebar)")
45
VENTRIKULAR TACHYCARDIA
Irama = Teratur Frekuensi (HR) = > 100 kali/menit Gelombang P = Tidak ada Interval PR = Tidak ada Lebar Gelombang QRS = > 0,12 detik (Lebar) Occurs with repetitive firing of an irritable ventricular ectopic focus. VT may result from increased automaticity or a re-entry mechanism. The sinus node may continue to discharge independently, depolarizing the atria but not the ventricles (atrioventricular dissociation), although P waves seldom seen in sustained VT. VT may occur in clients with ischemic heart disease, MI, cardiomyopathy, hypokalemis, hypomagnesemia, valvular heart disease, heart failure, drug toxicity, hypotension, or ventricular aneurysm. In clients who go into cardiac arrest, VT is commonly the initial rhythm before deterioration into ventricular fibrilation (VF) as the terminal rhythm,
 = > 100 kali/menit. Gelombang P = Tidak ada. Interval PR = Tidak ada. Lebar Gelombang QRS = > 0,12 detik (Lebar) Occurs with repetitive firing of an irritable ventricular ectopic focus. VT may result from increased automaticity or a re-entry mechanism. The sinus node may continue to discharge independently, depolarizing the atria but not the ventricles (atrioventricular dissociation), although P waves seldom seen in sustained VT. VT may occur in clients with ischemic heart disease, MI, cardiomyopathy, hypokalemis, hypomagnesemia, valvular heart disease, heart failure, drug toxicity, hypotension, or ventricular aneurysm. In clients who go into cardiac arrest, VT is commonly the initial rhythm before deterioration into ventricular fibrilation (VF) as the terminal rhythm,")
46
MONOMORPHIC

47
TORSADE DE POINTES (salah satu bentuk VT POLYMORPHIC)
")
48
VENTRIKEL FIBRILASI (VF)
Irama = Tidak Teratur Frekuensi (HR) = > 350 kali/menit Gelombang P = Tidak ada Interval PR = Tidak ada Lebar Gelombang QRS = > 0,12 detik (Lebar) VF is the result of electrical chaos in the ventricles. Impulses from many irritable foci fire in a totally disorganized manner so that ventricular contraction cannot occur. there are no recognizable deflections. Instead, there are irregular undulations of varying amplitudes, from coarse to fine. The ventricles merely quiver, consuming a tremendous amount of oxygen, there is no cardiac output or pulse and hterefore no cerebral, myocardial, or systemic perfusion. Ventricular fibrillation may b ethe first manifestation of coronary artery disease (CAD). Clients with myocardial infarction (MI) are at great risk for VF, which may also occur in clients with myocardial ischemia, hypokalemia, hypomagnesemia, hemorrhage, antidysrhytmic, therapy, rapid supraventricular tachydysrhythmias (SVTs), shock, asynchronous pacing with competition, or severe metabolic disease. VF also occurs following surgery or trauma.
 = > 350 kali/menit. Gelombang P = Tidak ada. Interval PR = Tidak ada. Lebar Gelombang QRS = > 0,12 detik (Lebar) VF is the result of electrical chaos in the ventricles. Impulses from many irritable foci fire in a totally disorganized manner so that ventricular contraction cannot occur. there are no recognizable deflections. Instead, there are irregular undulations of varying amplitudes, from coarse to fine. The ventricles merely quiver, consuming a tremendous amount of oxygen, there is no cardiac output or pulse and hterefore no cerebral, myocardial, or systemic perfusion. Ventricular fibrillation may b ethe first manifestation of coronary artery disease (CAD). Clients with myocardial infarction (MI) are at great risk for VF, which may also occur in clients with myocardial ischemia, hypokalemia, hypomagnesemia, hemorrhage, antidysrhytmic, therapy, rapid supraventricular tachydysrhythmias (SVTs), shock, asynchronous pacing with competition, or severe metabolic disease. VF also occurs following surgery or trauma.")
49
KASAR (COARSE)
")
50
HALUS (FINE)
")
51
ASISTOL Tidak ad gambaran listrik jantung, gambaran yang terlihat hanya berbentuk garis lurus Asystole: the complete absence of any ventricular rhytm. There are no electrical impulses in the ventricles and therefore no ventricular depolarization.

52
AV BLOCK DERAJAT I Irama = Teratur
Frekuensi (HR) = Umumnya normal antara 60 – 100 kali/menit Gelombang P = Normal Interval PR = Memanjang > 0,20 detik dan konstan Lebar Gelombang QRS = Tidak lebih dari 0,12 detik (sempit) First-degree AV block is actually a conduction delay rateher than a block. AV node conduction is slow, prolonging the PR interval to greater than 0,20 second. However, all sinus impulses eventually reach the ventricles. The underlyin rhtym mus still be identified (e.g., sinus rhtym with first-degree AV block).
 = Umumnya normal antara 60 – 100 kali/menit. Gelombang P = Normal. Interval PR = Memanjang > 0,20 detik dan konstan. Lebar Gelombang QRS = Tidak lebih dari 0,12 detik (sempit) First-degree AV block is actually a conduction delay rateher than a block. AV node conduction is slow, prolonging the PR interval to greater than 0,20 second. However, all sinus impulses eventually reach the ventricles. The underlyin rhtym mus still be identified (e.g., sinus rhtym with first-degree AV block).")
53
AV BLOCK DERAJAT II TIPE I (WENCHENBACH)
Irama = Irama atrial teratur, Irama ventrikel tidak teratur Frekuensi (HR) = Frekuensi atrium > frekuensi ventrikel, Umumnya dalam batas normal 60 – 100 kali/menit Gelombang P = Normal, ada satu P yang tidak diikuti gelombang QRS In second degree AV block type I, each successive sinus impulse takes a little longer to conduct through the impaired AV node, until one impulse is completely blocked and fails to depolarize the ventricles. This block results in a nonconducted or dropped beat (missing QRS complex). There is progressive prolongation of the PR interval, followed by a dropped beat and a pause
 = Frekuensi atrium > frekuensi ventrikel, Umumnya dalam batas normal 60 – 100 kali/menit. Gelombang P = Normal, ada satu P yang tidak diikuti gelombang QRS. In second degree AV block type I, each successive sinus impulse takes a little longer to conduct through the impaired AV node, until one impulse is completely blocked and fails to depolarize the ventricles. This block results in a nonconducted or dropped beat (missing QRS complex). There is progressive prolongation of the PR interval, followed by a dropped beat and a pause.")
54
AV BLOCK DERAJAT II TIPE I (WENCHENBACH)
Interval PR = Makin lama makin panjang, sampai ada gelombang P yang tidak diikuti gelombang QRS (drop beat), kemudian siklusnya berulang Lebar Gelombang QRS = Tidak Lebih dari 0,12 detik (sempit) Mobitz type I block is caused by conduction delay in the AV node in 72% of patients and by conduction delay in the His-Purkinje system in the remaining 28%. The presence of a narrow QRS complex suggests the site of the delay is more likely to be in the AV node. However, a wide QRS complex may be observed with either AV nodal or infranodal conduction delay. In Mobitz type II block, the conduction delay occurs infranodally. The QRS complex is likely to be wide, except in patients where the delay is localized to the bundle of His. Mobitz I block can occur in individuals with high vagal tone, such as athletes or young children. Mobitz I block can occur in infants and young children with structural heart disease (eg, tetralogy of Fallot) and in individuals of any age following valvular surgery (especially mitral valve). Other causes of type I block include myocardial infarction (especially inferior wall), and drug induced (including beta-blockers, calcium channel blockers, amiodarone, digoxin, and possibly pentamidine).
, kemudian siklusnya berulang. Lebar Gelombang QRS = Tidak Lebih dari 0,12 detik (sempit) Mobitz type I block is caused by conduction delay in the AV node in 72% of patients and by conduction delay in the His-Purkinje system in the remaining 28%. The presence of a narrow QRS complex suggests the site of the delay is more likely to be in the AV node. However, a wide QRS complex may be observed with either AV nodal or infranodal conduction delay. In Mobitz type II block, the conduction delay occurs infranodally. The QRS complex is likely to be wide, except in patients where the delay is localized to the bundle of His. Mobitz I block can occur in individuals with high vagal tone, such as athletes or young children. Mobitz I block can occur in infants and young children with structural heart disease (eg, tetralogy of Fallot) and in individuals of any age following valvular surgery (especially mitral valve). Other causes of type I block include myocardial infarction (especially inferior wall), and drug induced (including beta-blockers, calcium channel blockers, amiodarone, digoxin, and possibly pentamidine).")
55
AV BLOCK DERAJAT II TIPE 2
Irama = Irama atrial teratur, Irama ventrikel tidak teratur Frekuensi (HR) = Frekuensi atrium > frekuensi ventrikel Gelombang P = Normal, ada satu atau lebih gel. P yang tidak diikuti gel QRS In mobitz type II block, the block is actually infranodal, occurring below the bundle of His. It involves a constant block in one of the bundle branches, resulting in a wide QRS complex in conducted beats and an intermittent block in the other bundle branch, resulting in dropped beats because both bundles are blocked (P waves are not followed by a QRS complex). Because the block is not in the AV node, sinus impulses that conduct to the ventricles always do so with a constant PR interval. Impulses may be blocked randomly, making the ventricular rhytm irregular. Alternatively, the impulses may be blocked at regular intervals. It may occur: anterior wall MI because of severe ischemic damage to the conductionn system. It may also be caused by rheumatic heart disease or degenerative disease of the conduction system. It is a serious block that may oprogress suddenly to a third-degree AV block
 = Frekuensi atrium > frekuensi ventrikel. Gelombang P = Normal, ada satu atau lebih gel. P yang tidak diikuti gel QRS. In mobitz type II block, the block is actually infranodal, occurring below the bundle of His. It involves a constant block in one of the bundle branches, resulting in a wide QRS complex in conducted beats and an intermittent block in the other bundle branch, resulting in dropped beats because both bundles are blocked (P waves are not followed by a QRS complex). Because the block is not in the AV node, sinus impulses that conduct to the ventricles always do so with a constant PR interval. Impulses may be blocked randomly, making the ventricular rhytm irregular. Alternatively, the impulses may be blocked at regular intervals. It may occur: anterior wall MI because of severe ischemic damage to the conductionn system. It may also be caused by rheumatic heart disease or degenerative disease of the conduction system. It is a serious block that may oprogress suddenly to a third-degree AV block.")
56
AV BLOCK DERAJAT II TIPE 2
Interval PR = Normal atau memanjang tetapi konstan Lebar Gelombang QRS = Sempit, dapat juga lebar, tergantung dari mana aktivitas ventrikel berasal

57
AV BLOCK DERAJAT III (TOTAL AV BLOCK)
Irama = Teratur Frekuensi (HR) = Frekuensi atrium > frekuensi ventrikel Frekuensi ventrikel tergantung dari mana aktivitas ventrikel berasal (AV Node atau Purkinje) In third degree heart block, none of the sinus impulse conducts to the ventricles. The sinoatrial (SA) node is usuallly the pacemaker for the atria, producing P waves at a normal or even accelerated rate, while a separate, independent pacemaker paces the ventricles. Thus AV dissociation exists. If the block is in the AV node, a junctional escape focus paces the ventricles, producing normal QRS complexes at a rate of 40 to 60 beats/min. If the block is below the bundle of His (infranodal), a ventricular escape focus paces the ventricles, producing wide QRS complexes at a rate usually less than 40 beats/min. Third degree heart block in the adult may occur from ischemic injury with coronary artery disease (CAD) or Mi, degenerative disease of the conduction system, hypoxia, or calcific aortic stenosis. Third-degree heart block may occur with congenital heart disease, the effects of drugs or electrolyte disturbances, or cardiac surgery.
 = Frekuensi atrium > frekuensi ventrikel. Frekuensi ventrikel tergantung dari mana aktivitas ventrikel berasal (AV Node atau Purkinje) In third degree heart block, none of the sinus impulse conducts to the ventricles. The sinoatrial (SA) node is usuallly the pacemaker for the atria, producing P waves at a normal or even accelerated rate, while a separate, independent pacemaker paces the ventricles. Thus AV dissociation exists. If the block is in the AV node, a junctional escape focus paces the ventricles, producing normal QRS complexes at a rate of 40 to 60 beats/min. If the block is below the bundle of His (infranodal), a ventricular escape focus paces the ventricles, producing wide QRS complexes at a rate usually less than 40 beats/min. Third degree heart block in the adult may occur from ischemic injury with coronary artery disease (CAD) or Mi, degenerative disease of the conduction system, hypoxia, or calcific aortic stenosis. Third-degree heart block may occur with congenital heart disease, the effects of drugs or electrolyte disturbances, or cardiac surgery.")
58
AV BLOCK DERAJAT III (TOTAL AV BLOCK)
Gelombang P = Normal, baik bentuk maupun ukuran, ada beberapa gelombang P tidak diikuti gelombang QRS Interval PR = Tidak dapat diukur, oleh karena tidak ada hubungan antara gelombang P dan gelombang QRS

59
AV BLOCK DERAJAT III (TOTAL AV BLOCK)
Lebar Gelombang QRS = Sempit, dapat juga lebar, tergantung dari mana aktivitas ventrikel berasal Lebar jika sumber listriknya berasal dari ventrikel Sempit jika sumber listriknya berasal dari AV

61
OBAT-OBATAN PENDUKUNG KARDIOVASKULER

62
EPINEFRIN (ADRENALIN)
Menstimulasi reseptor ∝adrenergik (vasokonstriksi). Efek ∝adrenergik dari epinefrin dapat meningkatkan tekanan perfusi arteri koroner dan serebral selama RJP. Pada henti jantung epinefrin dapat diberikan 1 mg melalui IV/IO setiap 3-5 menit selama henti jantung Jika IV/IO sulit atau terlambat di pasang, epinefrin dapat diberikan melalui ETT dengan dosis mg Pada terapi bradikardi atau hipotensi dapat diberikan epinefrin per infus dengan mengambil 1 mg dilarutkan dalam 500 ml NaCl atau dekstrose 5%. Dosis awal 1 ųg/mnt. Dosis dapat mencapai 2-10 ųg/mnt.
. Efek ∝adrenergik dari epinefrin dapat meningkatkan tekanan perfusi arteri koroner dan serebral selama RJP. Pada henti jantung epinefrin dapat diberikan 1 mg melalui IV/IO setiap 3-5 menit selama henti jantung. Jika IV/IO sulit atau terlambat di pasang, epinefrin dapat diberikan melalui ETT dengan dosis mg. Pada terapi bradikardi atau hipotensi dapat diberikan epinefrin per infus dengan mengambil 1 mg dilarutkan dalam 500 ml NaCl atau dekstrose 5%. Dosis awal 1 ųg/mnt. Dosis dapat mencapai 2-10 ųg/mnt.")
63
VASOPRESIN Vasopresin adalah vasokonstriksi perifer non adrenergik dapat menyebabkan vasokonstriksi pada arteri koroner dan ginjal. Satu kali vasopresin 40 U IV/IO dapat menggantikan pada pemberian dosis pertama atau kedua epineprin dalam terapi henti jantung Of, relating to, or causing constriction of blood vessels ; One of the most important roles of AVP is to regulate the body's retention of water; it is released when the body is dehydrated and causes the kidneys to conserve water, thus concentrating the urine, and reducing urine volume. In high concentrations, it also raises blood pressure by inducing moderate vasoconstriction. In addition, it has a variety of neurological effects on the brain, having been found, for example, to influence pair-bonding in voles. A very similar substance, lysine vasopressin (LVP) or lypressin, has the same function in pigs and is often used in human therapy.
 or lypressin, has the same function in pigs and is often used in human therapy.")
64
SULFAS ATROPIN Asistol dapat terjadi akibat reflek vagal, pemberian obat vagalitik merupakan pendekatan psikologis yang tepat. Atropin murah, mudah dalam pemberiannya, dan mempunyai sedikit efek samping dan untuk itu dapat diberikan pada asistol dan PEA dengan HR < 60 x/mnt. Dosis Atropin yang direkomendasikan untuk henti jantung adalah 1 mg IV, dan dapat diulang setiap 3 sampai dengan 5 menit Dosis maksimal adalah 3 kali pemberian atau 3 mg.

65
OBAT ANTIARITMIA ADENOSIN
Adenosin dapat menghambat aktivitas SA dan AV node. Berikan 6 mg IV bolus cepat. Berikan 1-3 detik dan dilanjutkan dengan 20 ml NaCl serta tangan diangkat. Jika tidak ada perubahan irama selama 1-2 menit, berikan kembali 12 mg IV bolus cepat, berikan kembali 12 mg IV olus cepat jika dalam 1-2 menit tidak terjadi perubahan irama.

66
AMIODARON Amiodaron dapat dipertimbangkan pemberiannya pada VF atau VT tanpa nadi yang tidak bereaksi oleh defibrilasi, RJP dan vasopresor. Dosis awal adalah 300 mg IV/IO dan dapat di ulang dengan dosis 150 mg IV/IO Dosis maintenance: 360 mg/6 jam kemudian dilanjutkan dengan 540 mg/8 jam.

67
LIDOKAIN Lidokain dapat dipertimbangkan sebagai terapi alternatif selain amiodaron Dosis awal adalah mk/kg BB IV. Jika VF atau VT tanpa nadi menetap, dosis tambahan mg/kg BB IV bolus dan diberikan dengan jarak 5-10 menit, dosis maksimal 3 mg/kgBB

68
MAGNESIUM SULFAT Magnesium sulfat direkomendasikan untuk pengobatan Torsades de Pointes VT dengan atau tanpa henti jantung. Berikan magnesium sulfat 1-2 gr dilarutkan dalam 10 ml D5 IV/IO selama 5-20 menit pada henti jantung, tetapi pada kondisi torsades dengan nadi dosis yang sama dilarutkan dalam ml D5W selama 5-60 menit.

69
DOPAMIN Dopamin HCL adalah katekolamin.
Selama resusitasi sering dipergunakan untuk terapi hipotensi, khususnya jika bersamaan dengan bradikardi simptomatik. Katekolamin memfasilitasi reaksi fisik yang berkenaan dengan persiapan aksi otot mencakup peningkatan denyut jantung dan paru-paru, penghambatan kerja lambung dan usus halus, konstriksi pembuluh darah di banyak wilayah tubuh, inhibisi kelenjar air mata, pembesaran pupil mata, relaksasi kandung kemih, dan penghambatan ereksi. Katekolamin menyebabkan fisiologi tubuh secara umum merubah diri untuk menyesuaikan menghadapi aktivitas fisik.

70
NATRIUM BIKARBONAT Dalam situasi resusitasi khusus, seperti keadaan asidosis metabolik, hiperkalemia, natrium bikarbonat dapat bermanfaat. Dapat diberikan dengan dosis 1 mEq/KgBB Jika memungkinkan pemberian natrium bikarbonat harus mengetahui konsentrasi bikarbonat dalam darah atau dengan menggunakan analisa gas darah.

72
PENGOBATAN DENGAN LISTRIK
TERAPI LISTRIK

73
A. DEFIBRILASI Defibrilasi adalah pengobatan yang menggunakan aliran listrik dalam waktu yang singkat secara sinkron Indikasi : VF dan VT tanpa nadi

74
Defibrilasi harus dilakukan sedini mungkin dengan alasan:
Irama yang didapat pada permulaan henti jantung umumnya adalah VF Pengobatan yang paling efektif untuk ventrikel fibrilasi adalah defibrilasi Makin lambat defibrilasi dilakukan, makin kurang kemungkinan keberhasilannya Ventrikel fibrilasi cenderung untuk berubah menjadi asistol dalam waktu beberapa menit

75
Alat yang dipergunakan:
1. Defibrilator Defibrilator adalah alat yang dapat memberikan syok listrik dan dapat menyebabkan depolarisasi sementara dari jantung yang denyutnya tidak teratur, sehingga memungkinkan timbulnya kembali aktifitas listrik jantung yang terkoordinir. Energi dialirkan melalui suatu elektrode yang disebut paddle

76
Defibrilator diklasifikasikan menurut 2 tipe bentuk gelombangnya yaitu monophasic dan biphasic

77
2. Jeli Jeli digunakan untuk mengurangi tahanan dada dan membantu menghantarkan aliran listrik ke jantung, jeli dioleskan pada kedua paddle Untuk VF dan VT tanpa nadi, energi 360 joule dengan menggunakan monophasic defibrilator, dapat diulang setiap 2 menit dengan energi yang sama. Jika menggunakan biphasic defibrilator energi yang diperlukan berkisar antara joule Monophasic defibrillation delivers a charge in only one direction. Biphasic defibrillation delivers a charge in one direction for half of the shock and in the electrically opposite direction for the second half.

78
Prosedur defibrilasi:
Nyalakan defibrilasi Tentukan energi yang diperlukan dengan cara memutar atau menggeser tombol energi Paddle diberi jeli secukupnya Letakkan paddle dengan posisi paddle apex diletakkan pada apex jantung dan paddle sternum diletakkan pada garis sternal kanan di bawah klavikula

81
Isi (charge) energi, tunggu sampai energi terisi penuh, untuk mengetahui energi sudah penuh, banyak macamnya tergantung dari defibrilator yang dipakai, ada yang memberi tanda dengan menunjukkan angka joule yang diset, ada pula yang memberi tanda dengan bunyi bahkan ada juga yang memberi tanda dengan nyala lampu
 energi, tunggu sampai energi terisi penuh, untuk mengetahui energi sudah penuh, banyak macamnya tergantung dari defibrilator yang dipakai, ada yang memberi tanda dengan menunjukkan angka joule yang diset, ada pula yang memberi tanda dengan bunyi bahkan ada juga yang memberi tanda dengan nyala lampu")
82
Jika energi sudah penuh, beri aba-aba dengan suara keras dan jelas agar tidak ada lagi anggota tim yang masih ada kontak dengan pasien atau korban, termasuk juga yang mengoperatorkan defibrilator, sebagai contoh: Energi siap Saya siap Tim lain siap Gambaran EKG tetap..... Discharge

83
Kaji ulang layar monitor defibriltor, pastikan irama masih VF/VT tanpa nadi, pastikan energi sudah sesuai dengan yang diset, dan pastikan modus yang dipakai adalah asinkron, jika semua benar, berikan energi tersebut dengan cara menekan kedua tombol discharge pada kedua paddle. Pastikan paddle menempel dengan baik pada dada pasien (beban tekana pada paddle kira-kira 10 kg)
.")
84
Kaji ulang di layar monitor defibrilator apakah irama berubaha atau tetap sama seperti sebelum dilakukan defibrilasi, jika berubah cek nadi untuk menentukan perlu tidaknya dilakukan RJP, jika tidak berubah lakukan RJP.

85
B. KARDIOVERSI Kardioversi adalah pengobatan yang menggunakan aliran listrik dalam waktu singkat secara sinkron Indikasi: VT, SVT, Afl, AF

87
Alat yang digunakan: Defibrilator yang mempunyai modus sinkron Jeli
Troli emergensi, terutama alat bantu nafas Obat-obat analgetik dan sedatif Elektrode EKG

88
Energi: Energi awal untuk SVT dan atrial flutter adalah 50 joule, apabila tidak berhasil energi dapat dinaikkan menjadi 100 joule, 200 joule, 300 joule dan 360 joule Untuk VT monomorphic dan atrial fibrilasi, energi awal adalah 100 joule dan dapat dinaikkan sampai 360 joule Sedangkan VT polymorphic besarnya energi dan modus yang dipakai sama dengan yang digunakan pada tindakan defibrilasi

89
Prosedur: Prosedur tindakan kardioversi sama dengan tindakan defibrilasi, hanya pada saat menekan tombol discharge kedua tombol tersebut harus ditekan agak lama, karena modul yang dipakai adalah modul sinkron dimana pada modul ini, energi akan dikeluarkan (diberikan) beberapa milidetik setelah defibrilator tersebut menangkap gelombang QRS.
 beberapa milidetik setelah defibrilator tersebut menangkap gelombang QRS.")
90
Pasien dengan takikardi walaupun mungkin keadaanya tidak stabil akan tetapi kadang pasiennya masih sadar, oleh sebab itu jika diperlukan tindakan kardioversi, maka pasien perlu diberikan obat sedasi dengan atau tanpa analgetik

93
ALGORITME

94
ALGORITME HENTI JANTUNG
ALGORITME BHD: minta bantuan dan RJP Berikan oksigen bila tersedia Pasang monitor/defibrilasi kalau tersedia

95
Cek irama, adakah indikasi defibrilasi ?

96
VF/VT (-) Lakukan 1 kali DC
Kaji irama, jika irama menetap: lakukan RJP 5 siklus (30:2) Kaji irama, adakah indikasi defibrilasi? (kalau ada defibrilasi) Bila IV terpasang berikan vasopresor: Epineprin 1 mg Ulangi setiap 3-5 menit Dapat digunakan dosis tunggal vasopresin 40 u.
 Kaji irama, adakah indikasi defibrilasi (kalau ada defibrilasi) Bila IV terpasang berikan vasopresor: Epineprin 1 mg. Ulangi setiap 3-5 menit. Dapat digunakan dosis tunggal vasopresin 40 u.")
97
Kaji irama, adakah indikasi defibrilasi?
Lakukan RJP setelah defibrilasi Berikan Anti aritmia Amiodaron 300 mg IV atau Lidokain mg/kgBB utk dosis pertama, selanjutnya mg/kgBB (maksimum: 3 mg) Magnesium sulfat 1-2 gr IV untuk Torsades de Pointes Setelah 5 siklus, kaji kembali
 Magnesium sulfat 1-2 gr IV untuk Torsades de Pointes. Setelah 5 siklus, kaji kembali.")
98
Lanjutkan RJP selama 5 siklus Bila IV terpasang berikan:
ASISTOLE/PEA Lanjutkan RJP selama 5 siklus Bila IV terpasang berikan: Epineprin 1 mg IV Ulangi setiap 3-5 menit atau Vasopresin 40 u. Pikirkan pemberian atropin 1 mg IV untuk asistol atau PEA lambat, ulangi setiap 3-5 menit (3 kali pemberian). the regular beating in the arteries, caused by the contractions of the heart The impulse transmitted to arteries by contraction of the left ventricle of the heart. In an artery the pulse is due to the expansion and contraction of the elastic walls of the artery by the action of the heart upon the column of blood in the arterial system.
. the regular beating in the arteries, caused by the contractions of the heart. The impulse transmitted to arteries by contraction of the left ventricle of the heart. In an artery the pulse is due to the expansion and contraction of the elastic walls of the artery by the action of the heart upon the column of blood in the arterial system.")
99
3. Lakukan RJP 5 siklus (30:2)
")
101
ALGORITME TANPA HENTI JANTUNG
BRADIKARDI Frekuensi jantung < 60 x/mnt dan tidak adekuat untuk kondisi klinik Pertahankan jalan nafas, bila perlu Berikan oksigen Monitor EKG (kaji irama), tekanan darah, saturasi oksigen Pasang IV The pulse is most commonly felt where the radial artery lies near the surface on the thumb side of the wrist. It is made palpable by the ‘pulse pressure wave’ — initiated by each heart beat — reaching and expanding the artery. This wave is transmitted to the wrist at about 10 metres per second around forty times faster than the speed of the blood flow itself. The information obtained from feeling the pulse is limited but important. The feel of the artery itself may suggest whether its wall has normal resilience, or is hardened and thickened by arteriosclerosis. The pulse may feel, at one extreme, ‘strong’ and ‘full’ or, at the other, ‘weak’ or ‘thready’. These are indirect indications of the stroke volume of the heart. The impulse felt in the radial artery is related to the rise in arterial blood pressure generated by the heart at each beat — the pulse pressure. For any given stroke volume, this rise in pressure depends on the elasticity of the arteries: the more compliant they are the less the pressure rises; the stiffer they are with age and arteriosclerosis, the more sharply the pressure rises. These subtleties may be recognized by an experienced observer. The rate may be faster or slower than normally expected in the circumstances. In healthy adults the rate at rest, although typically 60-70, can be anything from 40 per minute, say in an elite long-distance swimmer, to about 80 per minute. Even so the rate can, for example, be used to distinguish a simple faint (slow) from loss of consciousness caused by haemorrhage (fast).
, tekanan darah, saturasi oksigen. Pasang IV. The pulse is most commonly felt where the radial artery lies near the surface on the thumb side of the wrist. It is made palpable by the ‘pulse pressure wave’ — initiated by each heart beat — reaching and expanding the artery. This wave is transmitted to the wrist at about 10 metres per second around forty times faster than the speed of the blood flow itself. The information obtained from feeling the pulse is limited but important. The feel of the artery itself may suggest whether its wall has normal resilience, or is hardened and thickened by arteriosclerosis. The pulse may feel, at one extreme, ‘strong’ and ‘full’ or, at the other, ‘weak’ or ‘thready’. These are indirect indications of the stroke volume of the heart. The impulse felt in the radial artery is related to the rise in arterial blood pressure generated by the heart at each beat — the pulse pressure. For any given stroke volume, this rise in pressure depends on the elasticity of the arteries: the more compliant they are the less the pressure rises; the stiffer they are with age and arteriosclerosis, the more sharply the pressure rises. These subtleties may be recognized by an experienced observer. The rate may be faster or slower than normally expected in the circumstances. In healthy adults the rate at rest, although typically 60-70, can be anything from 40 per minute, say in an elite long-distance swimmer, to about 80 per minute. Even so the rate can, for example, be used to distinguish a simple faint (slow) from loss of consciousness caused by haemorrhage (fast).")
102
Apakah tanda dan gejala gangguan perfusi disebabkan oleh Bradikardi (misalnya gangguan status mental, nyeri dada, hipotensi atau tanda-tanda lain dari syok) Perfusi adekuat: observasi/monitor

103
Perfusi tidak adekuat:
Siapkan pacu jantung transkutan; gunakan segera pada blok derajat II dan III Pertimbangkan pemberian Atropin 0.5 mg Pertimbangkan pembreian epineprin 2-10 ug/mnt atau dopamin 2-10ug/kgBB/mnt, sementara menunggu pacu jantung atau jika pacu jantung tidak efektif

104
Persiapkan pacu jantung transvenous
Atasi penyebab Pertimbangkan konsultasi ke ahli

105
TAKIKARDI Syarat: nadi (+), HR > 150 x/mnt, EKG= SVT, VT (+), perfusi adekuat atau tidak adekuat (tidak stabil) Penyebab, diatasi (tidak stabil): hypertermia, hipogligemik, hipo-hiperkalemia etc.
: hypertermia, hipogligemik, hipo-hiperkalemia etc.")
106
QRS SEMPIT SVT Anamnesa: Bp, cek lab, saturasi oksigen SVT stabil
Vagal manuver (sebelum vagal, siapkan SA 0.5 mg) : batuk, mengedan, pijat karotis Adenosin inj: 6 mg-12 mg-12 mg
 : batuk, mengedan, pijat karotis. Adenosin inj: 6 mg-12 mg-12 mg.")
107
Kalau pasien menjadi tidak stabil, rencanakan kardioversi:
Jelaskan Informed consent Sedatif/analgetik Siapkan alat-alat resusitasi 5. Kardioversi 50 joule (kalau gambaran EKG tetap joule meningkat dan dapat diulang setiap 3-5 menit)
")
108
QRS LEBAR VT (+), MONOMORFIK
Stabil: berikan Amiodaron 150 mg dalam cc dalam waktu 10 menit, 360 mg/6 jam, 540 mg/8 jam (oral: 3X200 mg) Tidak Stabil: cardioversi 100 joule
 Tidak Stabil: cardioversi 100 joule.")
109
VT POLIMORFIK Stabil: MGSO4 1-2 gr Lidokain mg/kgBB, maintenance 1-4 mg/menit 2. Tidak stabil: defibrilasi 360 joule

Presentasi serupa
















>")











