Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
FAQ Laboratory Study in Sepsis
Nina Dwi Putri

5
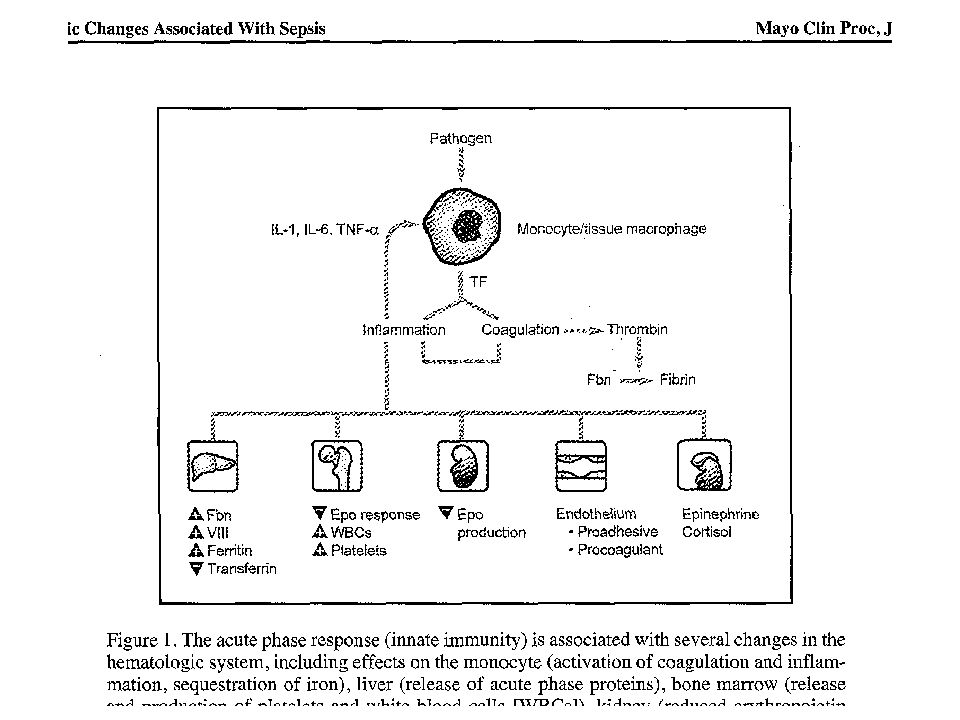
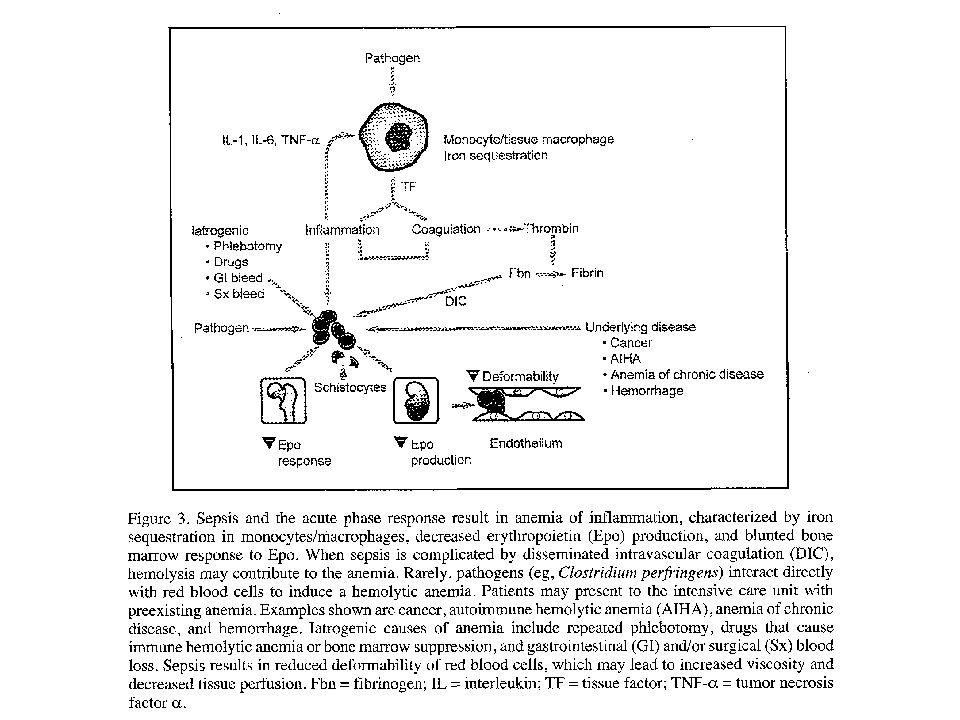
Hemoglobin-Anemia blood loss
decreased production (hypoproliferative ane- mia) a reticuloendothelial block in iron transport decreased sensitivity of the erythron to erythropoietin shortened red blood cell survival. increased destruction (hemolytic anemia) of red blood cells
 a reticuloendothelial block in iron transport. decreased sensitivity of the erythron to erythropoietin. shortened red blood cell survival. increased destruction (hemolytic anemia) of red blood cells.")
7
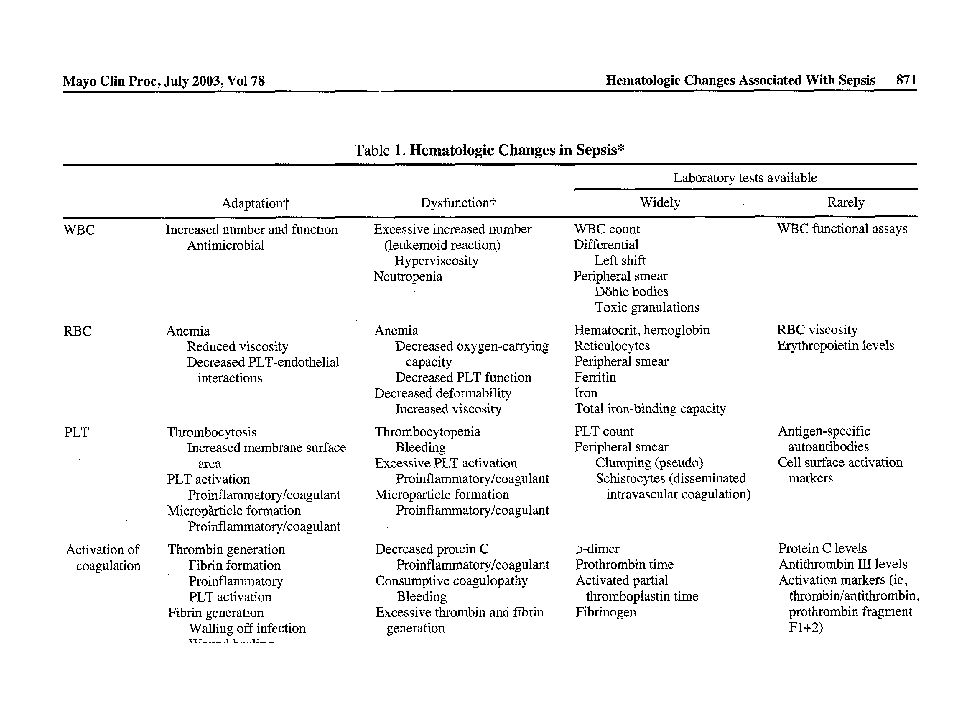
Neutrophils: phagocytosing infectious organisms, crystalline material (e.g., uric acid), and immune complexes Leucocytosis: recruitment of mature neutrophils from the marginating pool into the circulating pool mobilization of mature and developing neutrophils from the bone marrow eventually increased leukopoiesis Neutropenia: exhaustion of BM progenitors, maturation arrest, imbalance extravasation and production

8
Leucocyte

9
Platelet

12
ESR Non-specific marker of tissue injury
More useful than leukocyte count in identifying inflammatory conditions Differentiating mild versus severe states of inflammation Detection of inflammatory diseases and malignancy Less useful in categorizing the etiology behind the highly inflamed patients

13
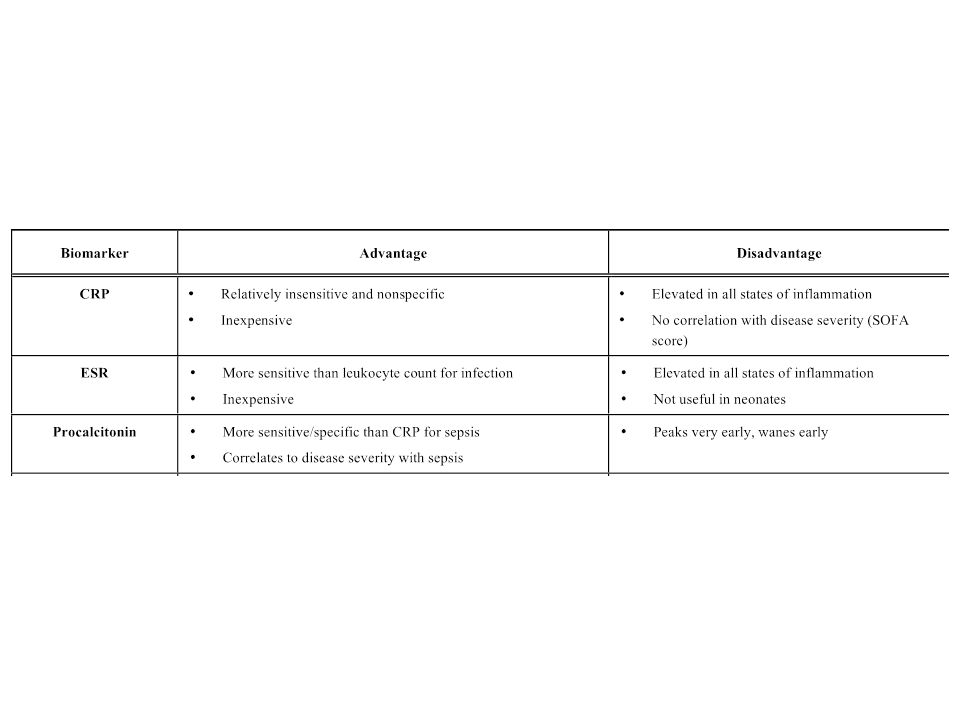
C-REACTIVE PROTEIN (CRP)
protein fase akut yang dibentuk oleh sel hepatosit akibat rangsangan sitokin anti-inflamasi CRP meningkat dalam 4-6 jam 8 jam: 2x lipat Puncaknya jam Penyembuhan: penurunan kadar CRP secara cepat CRP memiliki masa paruh 4 sampai 7 jam Sangat baik untuk menilai aktivitas penyakit dalam keadaan akut.

14
Peningkatan CRP dapat dijumpai pada kondisi selain infeksi
MAJOR ELEVATION Bacterial infection Hypersensitivity complications of infections Inflammatory disease Transplantation Cancer Necrosis trauma - pyelonephritis, pelvic infections, meningitis, endocarditis Rheumatic fever, erythema nodosum rheumatoid arthritis, juvenile chronic arthritis, ankylosing spondylitis, psoriatic arthritis, systemic vasculitis, polymialgia rheumatica, reiter’s disease, Crohn’s disease, familial mediterranian fever renal transplantation lymphoma , sarcoma myocardial infarction, tumor embolisation, acute pancreatitis burn, fractures MINOR OR NO ELEVATION Transplantations SLE, systemic sclerosis, dermatomycosis, ulcerative colitis, Sjogren’s syndrome graft vs host disease leukemia Nobre V et al. Am J Respiir Crit Care Med, 2008;117:

15
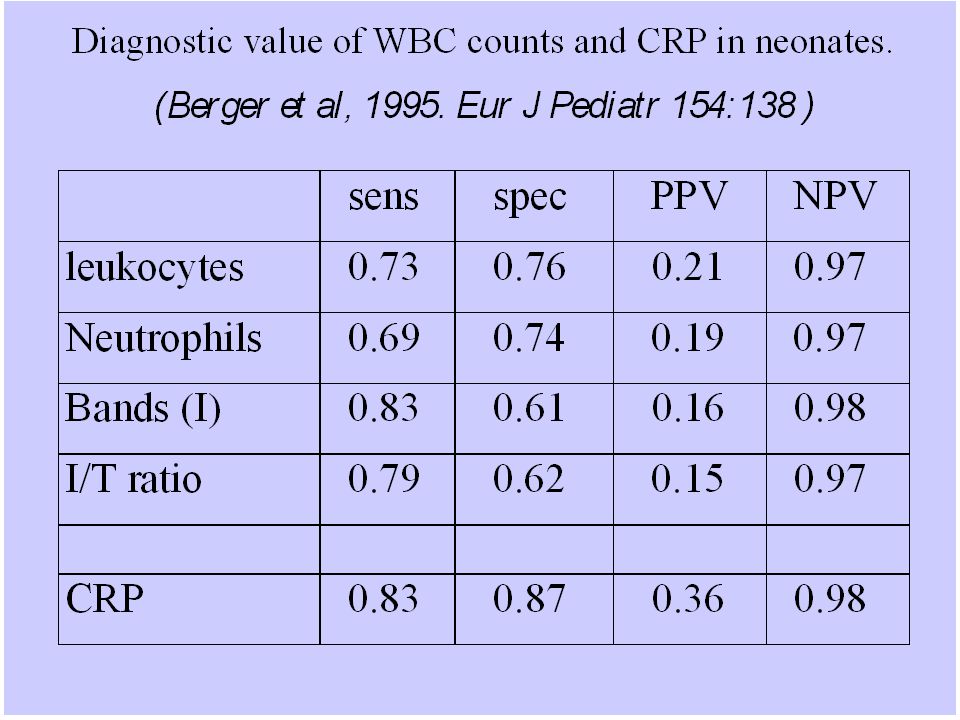
…sepsis CRP LEVEL Normal concentration in healthy human serum < 10 mg/L (increasing with aging). CRP (mg/L) 10 – 40 Mild inflammation, viral or bacterial infection, late pregnan woman Moderate inflammation, viral orbacterial infection 100 – 200 Marked inflmmation, bacterial infection > 200 Severe bacterial infection or extensive trauma It takes 6-12 hours, even up to 24 hours for CRP to rise following onset infection. Sensitivity 40%, 60% of subsequently proven sepsis episodes will have an initial CRP (compared to 80% sensitivity of immature to total neutrophil ratio) Nobre V et al. Am J Respiir Crit Care Med, 2008;117:
 Nobre V et al. Am J Respiir Crit Care Med, 2008;117:")
20
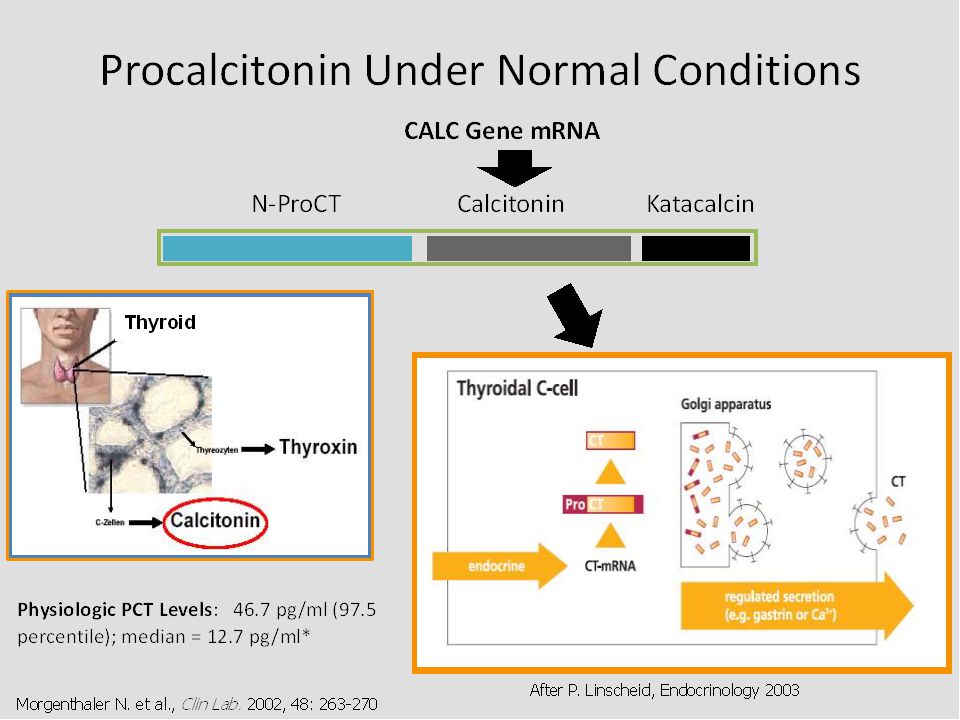
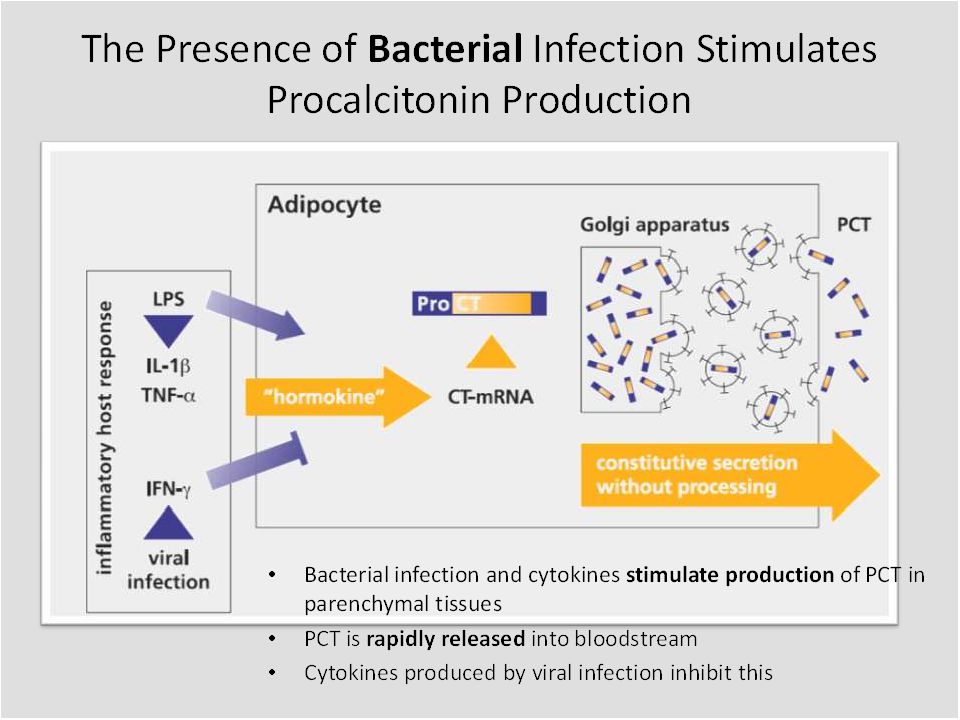
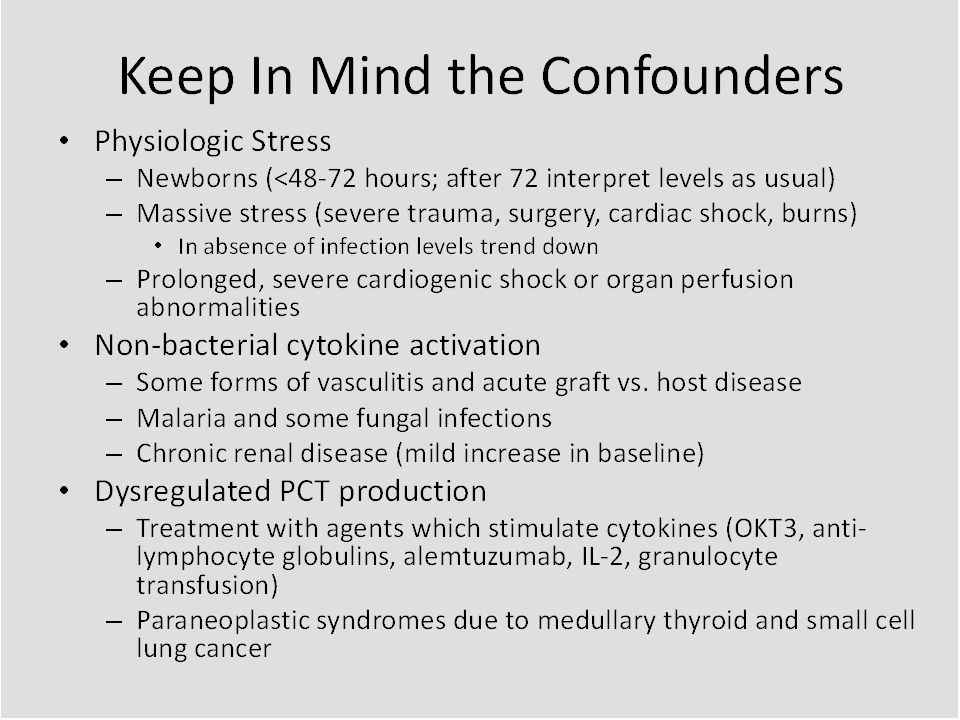
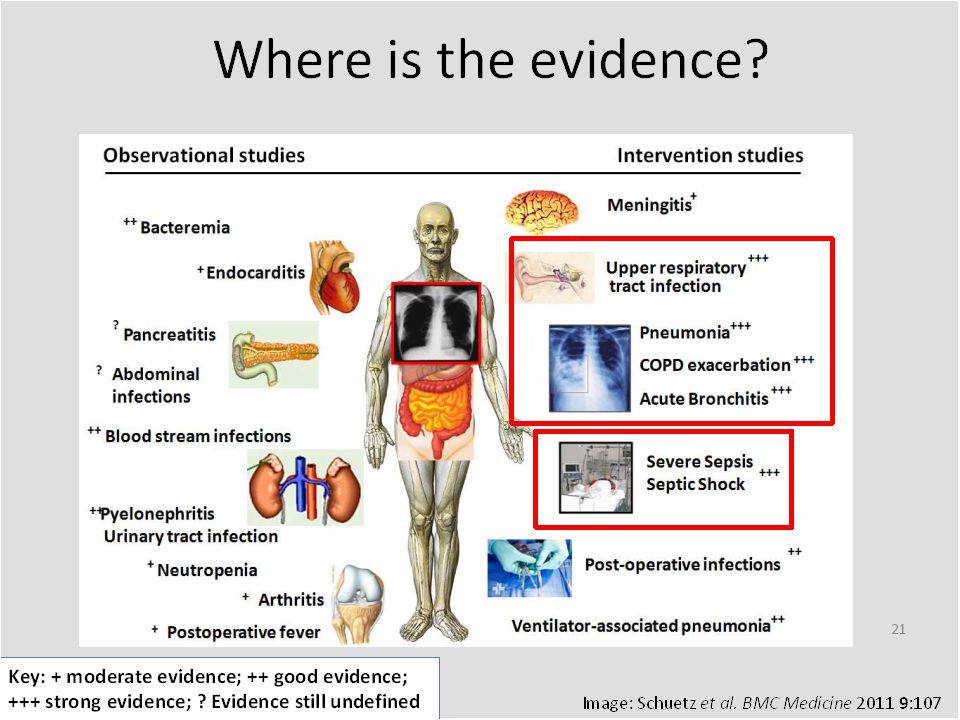
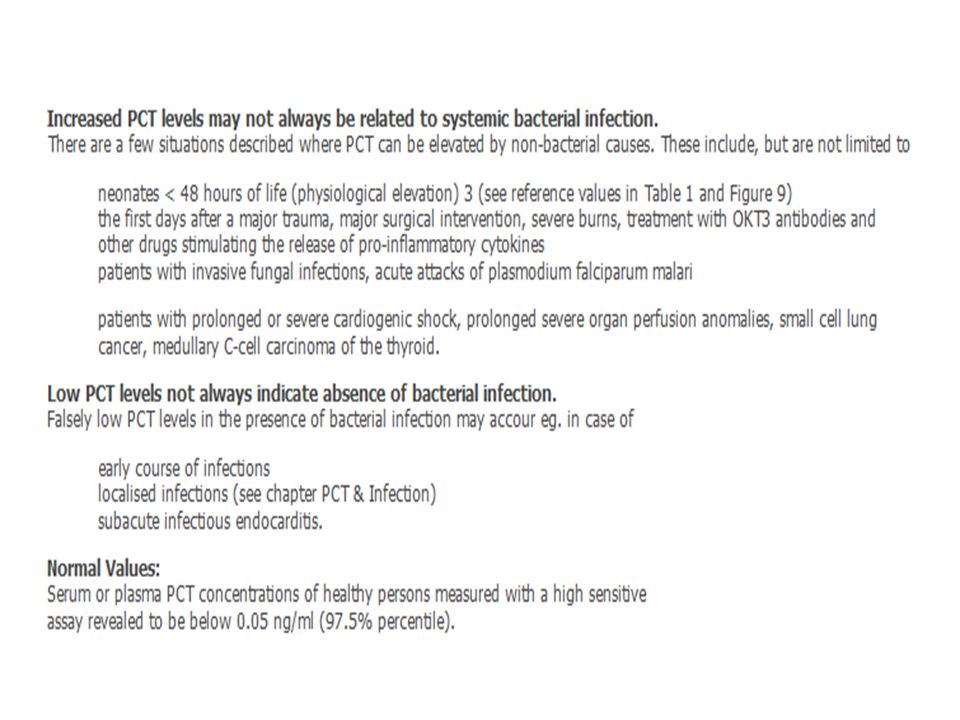
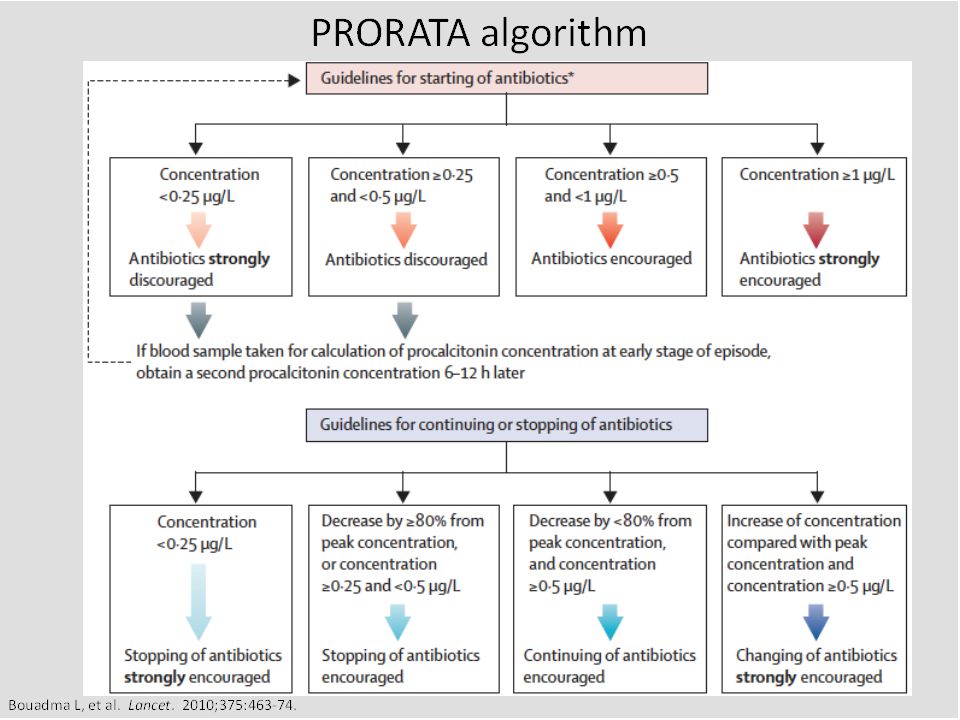
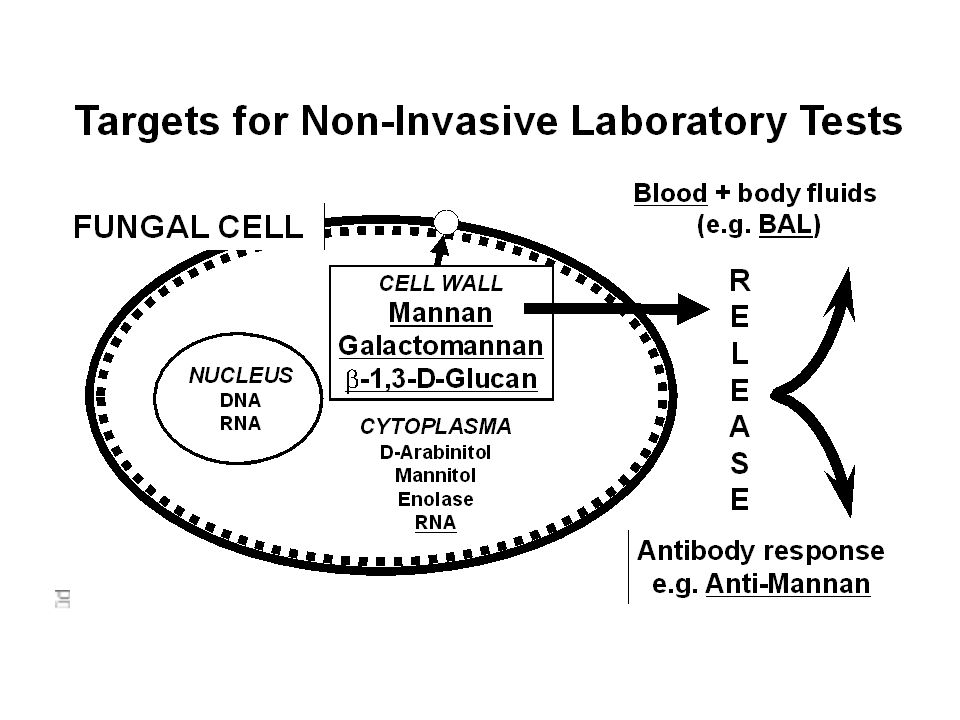
PROCALCITONIN

27
Asal Spesimen Seharusnya steril Ada flora normal komensal Darah
Sumsum tulang Cairan sendi Jaringan Saluran napas bawah Kandung kemih Saluran napas atas Kulit Saluran gastrointestinal Saluran genital perempuan Uretra Pada bagian tubuh yang seharusnya steril, apabila ditemukan m.o: Telah terjadi infeksi Cara koleksi dan waktu pengiriman tidak tepat Laboratorium terlambat memulai pemeriksaan Bila spesimen diambil dari tempat dengan flora normal: Kuantitas/jumlah spesimen perlu diperhatikan Kondisi pasien: imunokompromais/imunokompeten

28
skin nose faring Mouth Lower GI
Flora normal : adalah bakteri yang hidup berdampingan dengan kita dan ada di organ kita, mis di kulit, saluran pencernaan, dimana fungsinya adalah mencegah kolonisasi bakteri patogen dengan cara mengeluarkan substansi toksik atau bersaing dengan nutrien. Ada 1014 bakteri yg mayoritas hidup di sal cerna ( usus besar) Ada mikroba per cm2 di kulit (Staphylococcus aureus, Staphylococcus epidermidis, Diphtheroid, Streptococci, Candida dll.). Di lambung dan usus halus terdapat Lactobacilli Di usus halus terdapat 104 bakteri per gram dan di usus besar 1011 per gram, 95-99% di antaranya adalah anaerob. Di saluran kemih terdapat koloni berbagai bakteri dan difteroid Bakteri skin nose faring Mouth Lower GI Staphylococcus epidermidis ++ + Staphylococcus aureus Enterococcus fecalis Streptoccuc pneumonia Pseudomonas spp. Murray PR. Medical Microbiology 2002.
 Ada mikroba per cm2 di kulit (Staphylococcus aureus, Staphylococcus epidermidis, Diphtheroid, Streptococci, Candida dll.). Di lambung dan usus halus terdapat Lactobacilli. Di usus halus terdapat 104 bakteri per gram dan di usus besar 1011 per gram, 95-99% di antaranya adalah anaerob. Di saluran kemih terdapat koloni berbagai bakteri dan difteroid. Bakteri. skin. nose. faring. Mouth. Lower GI. Staphylococcus epidermidis Staphylococcus aureus. Enterococcus fecalis. Streptoccuc pneumonia. Pseudomonas spp. Murray PR. Medical Microbiology")
29
Volume Darah untuk Pemeriksaan Kultur
IDSA guidelines 2013 Increased volume Increased Yield 10 ml 20 ml 30 % 40 % 20 ml 30 ml 10 % 15 % NOTE: Pediatric volume guide: usually draw 1 mL/year of age.

30
Biakan Darah Diambil pd 2 sisi berbeda (Clin Microbiol. Rev19: , 2006) Jumlah volume darah sangat menentukan hasil Waktu bakteremia (penting) 2 kultur diambil dari vena dan kateter : Keduanya vena (PPV 98 %) Keduanya kateter ( 50 %) Satu vena, satu kateter ( 96 % ) Secara teori pengambilan bahan untuk biakan darah diambil pada 2 sisi berbeda, ini dapat menentukan jika kebetulan menemukan kuman flora normal mis strep. Epidermidis, jika ditemukan pada 2 bahan biakan ( pos ) keduanya, maka memang benar terjadi infeksi oleh patogen tersebut, tetapi jika hanya satu saja yang positif, kemungkinan besar masih disebabkan kontaminan. NOTE: Pediatric volume guide: One can usually draw 1 mL/year of age. Volume is very important in detection of bacteria. The more blood collected the better the chance of detecting the presence of bacteria. For pediatrics especially, there must be a balance between volume of blood collected and the clinical condition of the patient. Remove the cap and disinfect the septum with an alcohol swab and allow to dry. Do not use iodine as it may damage the septum. Remember to hold the needle down onto the vial (WHO)
 2 kultur diambil dari vena dan kateter : Keduanya vena (PPV 98 %) Keduanya kateter ( 50 %) Satu vena, satu kateter ( 96 % ) Secara teori pengambilan bahan untuk biakan darah diambil pada 2 sisi berbeda, ini dapat menentukan jika kebetulan menemukan kuman flora normal mis strep. Epidermidis, jika ditemukan pada 2 bahan biakan ( pos ) keduanya, maka memang benar terjadi infeksi oleh patogen tersebut, tetapi jika hanya satu saja yang positif, kemungkinan besar masih disebabkan kontaminan. NOTE: Pediatric volume guide: One can usually draw 1 mL/year of age. Volume is very important in detection of bacteria. The more blood collected the better the chance of detecting the presence of bacteria. For pediatrics especially, there must be a balance between volume of blood collected and the clinical condition of the patient. Remove the cap and disinfect the septum with an alcohol swab and allow to dry. Do not use iodine as it may damage the septum. Remember to hold the needle down onto the vial (WHO)")
31
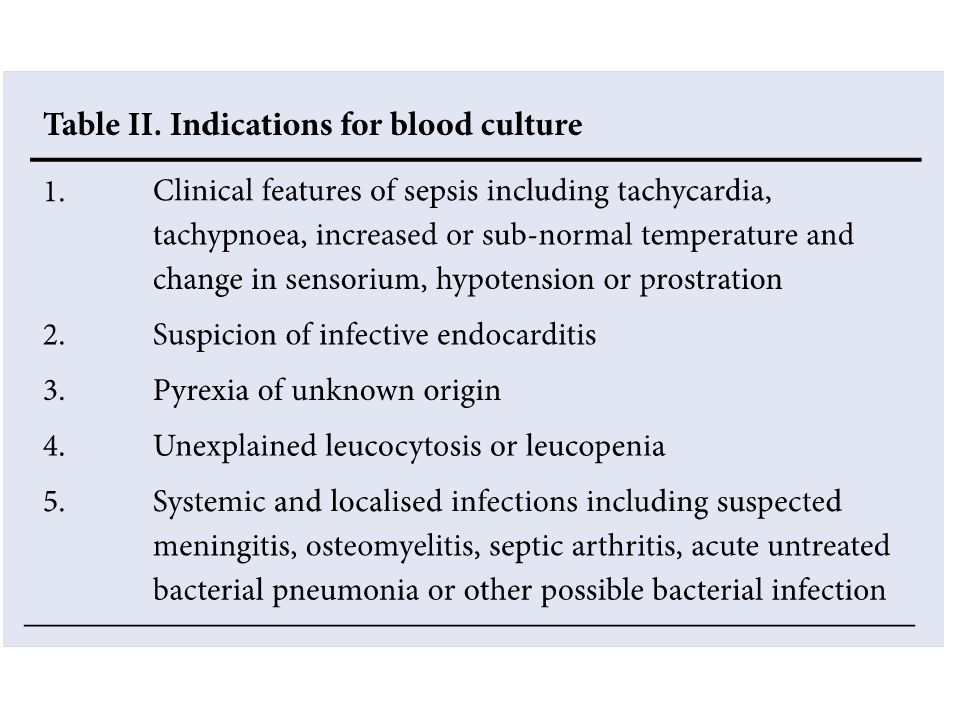
Number 1 blood culture is rarely, if ever, sufficient or advisable.
A positive result on a single culture is difficult to interpret, unless an unequivocal pathogen is isolated. 2 blood cultures are usually adequate when continuous bacteraemia is anticipated 3 blood cultures are reasonable when intermittent bacteraemia is suspected S Afr Med J 2010; 100:

32
Timing The ideal: ranging from one to several hours
2 separate sites within minutes of each other from patients who are acutely ill or those in whom the likelihood of continuous bacteraemia is high Intermittent bacteraemia: multiple blood cultures hours apart

33
Biakan Tinja dan Urin Biakan Tinja : 2 sampel berturut-turut
Tidak boleh >3 hari Biakan Urin: Pengumpulan spesimen minimal kontaminasi Pengambilan pagi hari Pengambilan sebelum pemberian antibiotik Segera dikirmkan untuk diproses, kemas dengan es Jika tidak segera dikirim masukkan almari es ( 40C ) Bakteriuria bermakna : Suprapubik : berapapun Kateter : Mid stream : Pengambilan bahan biakan sesudah diberikan terapi antimikroba dapat mempengaruhi penemuan bakteri
 Bakteriuria bermakna : Suprapubik : berapapun. Kateter : Mid stream : Pengambilan bahan biakan sesudah diberikan terapi antimikroba dapat mempengaruhi penemuan bakteri.")
34
SEPSIS Skrining sepsis : Kultur darah
Urin, secara mikroskopik dan kultur Kultur aspirat, ETT dan cairan tubuh/alat medis lainnya Procalcitonin PCR Cytokines : interleukin 6 (IL-6), interleukin 8 (IL-8), gamma interferon (IFN-γ), and tumor necrosis factor alpha (TNF-α), and cell surface antigens, including soluble intercellular adhesion molecule (sICAM) and CD64 Skrining sepsis : C-Reaktive Protein >10 mg/L. Sensitivitas tes ini: Spesifik: 83-94 Total Leucocyte Count (TLC) <5.000,>15.000 Sensitivitas tes ini: Spesifik: Absolute Neutrophil Count (ANC) Sensitivitas tes ini: Spesifik: Immature Total Ratio (ITR) >20 Sensitivitas tes ini: Spesifik: 50-78 Micro-ESR (mESR) > umur dalam hari+ 3 mm Sensitivitas: Spesifik:
, interleukin 8 (IL-8), gamma interferon (IFN-γ), and tumor necrosis factor alpha (TNF-α), and cell surface antigens, including soluble intercellular adhesion molecule (sICAM) and CD64. Skrining sepsis : C-Reaktive Protein >10 mg/L. Sensitivitas tes ini: Spesifik: Total Leucocyte Count (TLC) <5.000,> Sensitivitas tes ini: Spesifik: Absolute Neutrophil Count (ANC) Sensitivitas tes ini: Spesifik: Immature Total Ratio (ITR) >20. Sensitivitas tes ini: Spesifik: Micro-ESR (mESR) > umur dalam hari+ 3 mm. Sensitivitas: Spesifik:")
35
TERIMA KASIH

Presentasi serupa




 dan STATUS NUTRISI : MALNUTRISION INFECTION SCORE (MIS) PADA PASIEN YANG MENJALANI HEMODIALISIS REGULER.>")

>")













