Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
GINJAL KUNCORO PUGUH S

2
FUNGSI Pengaturan keseimbangan air & elektrolit
Pengaturan konsentrasi osmolaritas cairan tubuh & elektrolit Pengaturan keseimbangan asam basa Ekskresi hasil sisa metabolisme Pengaturan tekanan arteri Sekresi hormon Glukoneogenesis

3
Functions of the urinary system
Excretion The removal of organic waste products from body fluids Elimination The discharge of waste products into the environment Homeostatic regulation of blood plasma Regulating blood volume and pressure Regulating plasma ion concentrations Stabilizing blood pH Conserving nutrients

4
ANATOMI FISIOLOGI GINJAL ANJING

5
ANATOMI FISIOLOGI GINJAL SAPI

6
Figure 26.3 The Urinary System in Gross Dissection

7
ANATOMI & FISOLOGI

8
Two types of nephron Cortical nephrons Juxtamedullary nephrons
~85% of all nephrons Located in the cortex Juxtamedullary nephrons Closer to renal medulla Loops of Henle extend deep into renal pyramids

9
Figure 26.7 Cortical and Juxtamedullary Nephrons
Figure 26.7a

10
Figure 26.7 Cortical and Juxtamedullary Nephrons
Figure 26.7b, c

12
Nephron functions include:
Production of filtrate Reabsorption of organic nutrients Reabsorption of water and ions Secretion of waste products into tubular fluid

13
Urine production maintains homeostasis
Regulating blood volume and composition Excreting waste products Urea Creatinine Uric acid

14
Basic processes of urine formation
Filtration Blood pressure Water and solutes across glomerular capillaries Reabsorption The removal of water and solutes from the filtrate Secretion Transport of solutes from the peritubular fluid into the tubular fluid

15
Figure 26.9 An Overview of Urine Formation

16
Carrier Mediated Transport
Filtration in the kidneys modified by carrier mediated transport Facilitated diffusion Active transport Cotransport Countertransport Carrier proteins have a transport maximum (Tm) Determines renal threshold
 Determines renal threshold.")
17
Reabsorption and secretion
Accomplished via diffusion, osmosis, and carrier-mediated transport Tm determines renal threshold for reabsorption of substances in tubular fluid

18
Sectional anatomy of the kidneys
Superficial outer cortex and inner medulla The medulla consists of 6-18 renal pyramids The cortex is composed of roughly 1.25 million nephrons Major and minor calyces along with the pelvis drain urine to the ureters

19
NEPHRON Merupakan unit fungsionil terkecil ginjal 1 Juta / Ginjal
Panjang seluruh nephron = 45 – 65 mm

20
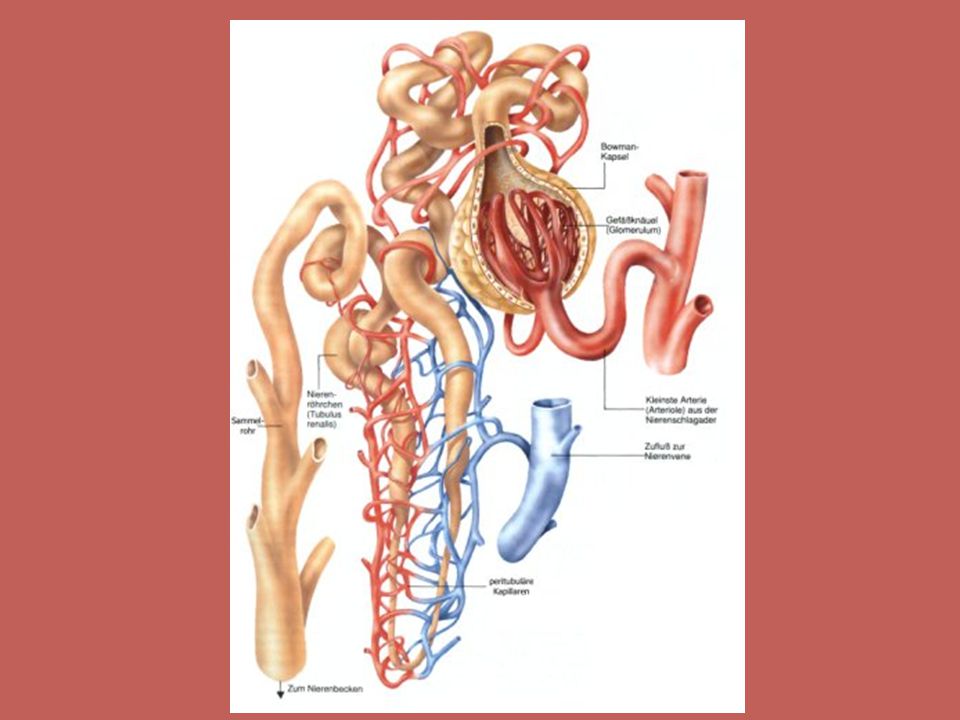
GLOMERULUS Kapsula Bowman : pars visceralis & pars parietalis
Filter glomerulus : 3 lapis Endhotelium kapiler :100nm Lamina basalis :8 nm Epithel Pars viceralis kapsula Bowman ( Podocyt) : 25 nm Luas area filtrasi 0,8 m2 Ultra filtrat = plasma - protein
 : 25 nm. Luas area filtrasi 0,8 m2. Ultra filtrat = plasma - protein.")
21
Figure 26.10 Glomerular Filtration

22
Figure 26.8 The Renal Corpuscle
Figure 26.8a, b

23
Figure 26.8 The Renal Corpuscle
Figure 26.8c, d

24
Figure 26.10 Glomerular Filtration
Figure 26.10a, b

25
Functional anatomy of the nephron
Proximal convoluted tubule (PCT) Actively reabsorbs nutrients, plasma proteins and ions from filtrate Released into peritubular fluid Loop of Henle Descending limb Ascending limb Each limb has a thick and thin section PLAY Animation: Urinary System Anatomy
 Actively reabsorbs nutrients, plasma proteins and ions from filtrate. Released into peritubular fluid. Loop of Henle. Descending limb. Ascending limb. Each limb has a thick and thin section. PLAY. Animation: Urinary System Anatomy.")
26
Reabsorption and secretion at the PCT
Glomerular filtration produces fluid similar to plasma without proteins The PCT reabsorbs 60-70% of the filtrate produced Reabsorption of most organic nutrients Active and passive reabsorption of sodium and other ions Reabsorption of water Secretion also occurs in the PCT PLAY Animation: Early Filtrate Processing PLAY Animation: Glomerular filtration

27
TUBULUS PROKSIMALIS P = 15 mm Tight junction
Lateral intercellular space Brush border Reabsorbsi 65 % Zat yg direabsorbsi tidak disekresi kecuali K+ Sekresi zat diikat oleh protein plasma

28
Figure 26.12 Transport Activities at the PCT
PLAY Animation: Proximal Convoluted Tubule Figure 26.12

29
The loop of Henle and countercurrent multiplication
Between ascending and descending limbs of loop Creates osmotic gradient in medulla Facilitates reabsorption of water and solutes before the DCT Permits passive reabsorption of water from tubular fluid

30
ANSA HENLE Pars decendent : 2- 14 mm
Pars Ascendent : mithokondria >>, Sel Junxtaglomerular vas. Afferent mensekresi RENIN ANSA HENLE SEGMEN TIPIS : permeabilitas besar, metabolisme minimal ANSA HENLE SEGMEN TEBAL : tidak permeabel thd H2O & Ureum, reabsorbsi aktif Cl- & Na+

31
Figure 26.13 Countercurrent Multiplication and Concentration of Urine
Figure 26.13a

32
Figure 26.13 Countercurrent Multiplication and Concentration of Urine
Figure 26.13b

33
Figure 26.13 Countercurrent Multiplication and Concentration of Urine

34
Functional anatomy of the nephron
Distal convoluted tubule (DCT) Actively secretes ions, toxins, drugs Reabsorbs sodium ions from tubular fluid PLAY Animation: Urinary System Dissection and Flythrough
 Actively secretes ions, toxins, drugs. Reabsorbs sodium ions from tubular fluid. PLAY. Animation: Urinary System Dissection and Flythrough.")
35
Reassertion and secretion at the DCT
DCT performs final adjustment of urine Active secretion or absorption Absorption Tubular cells actively resorb Na+ and Cl- In exchange for potassium or hydrogen ions (secreted)
")
36
TUBULUS DISTALIS P = 5 mm Ephitel lebih pipih dari ephitel tubulus proksimalis Brush border (─) Bagian proksimal = segmen tebal ansa henle Bagian distal terjadi ion exchange K+ dg Na+ : Hormon Aldosteron

37
Figure 26.14 Tubular Secretion and Solute Reabsorption at the DCT
PLAY Animation: Distal Convoluted Tubule Figure 26.14

38
Figure 26.14 Tubular Secretion and Solute Reabsorption at the DCT
Figure 26.14c

39
Reabsorption and secretion along the collecting system
Water and solute loss is regulated by aldosterone and ADH Reabsorption Sodium ion, bicarbonate, and urea are resorbed Secretion pH is controlled by secretion of hydrogen or bicarbonate ions

40
DUKTUS COLLIGENTES P = 20 mm Menampung beberapa tubulus distalis
Ber muara di papilla renalis Bagian Cortex : tidak permeabel thd ureum Bagian medulla ; permeabel thd ureum ADH < : tidak permeabel thd H2O

41
Figure 26.6 A Representative Nephron

42
Figure 26.5 The Blood Supply to the Kidneys
Figure 26.5c, d

43
Figure 26.5 The Blood Supply to the Kidneys
Figure 26.5a, b

44
SUPLAI DARAH GINJAL

46
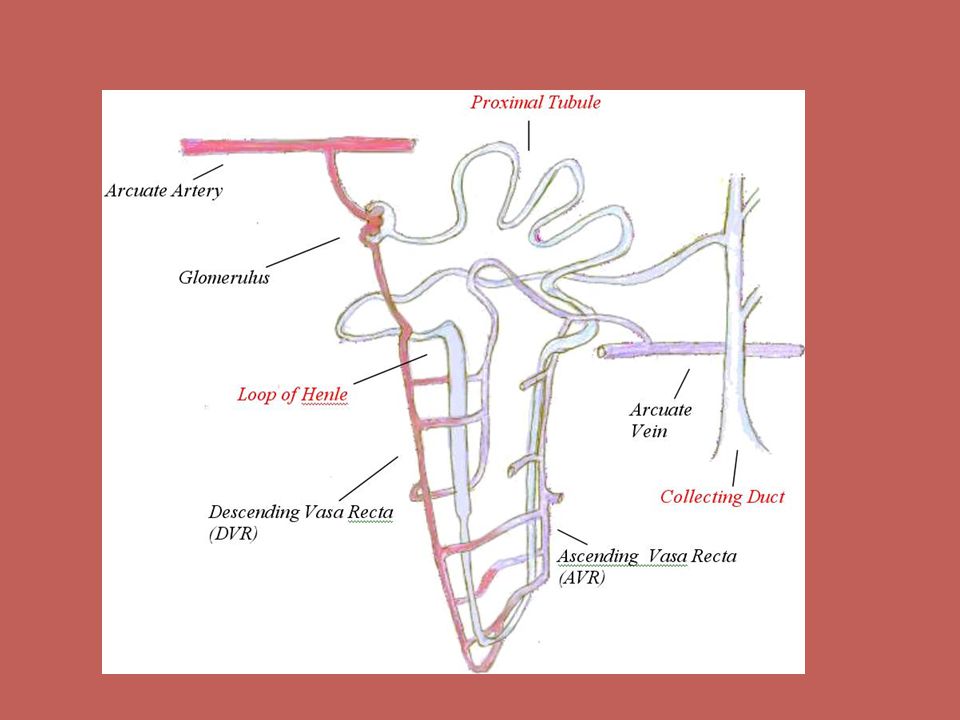
RENAL FRACTION Vasa afferent glomerulus membentuk vasa recta
Renal Blood Flow = 1200 ml/menit Cardiac Out Put = 5000ml/ menit Renal Fraction = 1200/5000 X 100% = 24%

47
KECEPATAN ALIRAN DARAH TIAP 100 g JARINGAN
ORGAN BLOOD FLOW (ml / min ) Otot Skelet Otak Hati Otot Jantung Ginjal 3 54 58 84 420
 Otot Skelet. Otak. Hati. Otot Jantung. Ginjal")
48
ALIRAN CAIRAN DLM TUBUH
JARINGAN Kecepatan (ml/min) Reabsorpsi ( %) Tubulus Proksimal Ansa Henle Tubulus Distalis Duct. Colligentes Urine 125 45 25 12 1 65 15 10 9,3 0,7
 Reabsorpsi ( %) Tubulus Proksimal. Ansa Henle. Tubulus Distalis. Duct. Colligentes. Urine ,3. 0,7.")
49
REABSORPSI ELEKTROLIT
( kation ) perlu dikendalikan, bila berubah : kegagalan faal ginjal K+ > : potensial membran < : paralisis K+ < : potensial membran > : paralisis Na+ << : Potensial aksi < : paralisis Ca++ < : permeabilitas membran > : tetani
 perlu dikendalikan, bila berubah : kegagalan faal ginjal. K+ > : potensial membran < : paralisis. K+ < : potensial membran > : paralisis. Na+ << : Potensial aksi < : paralisis. Ca++ < : permeabilitas membran > : tetani.")
50
Glomerular filtration rate (GFR)
Amount of filtrate produced in the kidneys each minute Factors that alter filtration pressure change GFR

51
GLOMERULAR FILTRATION RATE ( GFR)
Jumlah filtrat yg disaring dr plasma dalam satu menit Normal : 125 ml / min Lebih dr 99% direabsorpsi Produk urine : 1 L / hari Zat yg digunakan untuk mengukur : Inulin, Manitol

52
Factors controlling the GFR
A drop in filtration pressure stimulates Juxtaglomerular apparatus (JGA) Releases renin and erythropoietin
 Releases renin and erythropoietin.")
53
FAKTOR YG MEMPENGARUHI
Perubahan Tek. Darah Tek. Darah umum Status vasa afferent / efferent Contoh : latihan jasmani : vasokontriksi vasa afferent Caffein : Vasodilatasi vasa afferent

54
Perubahan Tekanan Capsular : Obstruksi, Edema jaringan
Perubahan Tek. Osmotik Koloid : Dehidrasi, Hipoprotein Perubahan Permeabilitas : Peny. Ginjal, Keracunan Obat Perubahan Luas Area Filtrasi : Peny. Ginjal, Nephrotomy

55
FILTRASI GLOMELURUS Effective Filtration Pressure (EFP)
Tek. Darah – Tek Capsular – Tek Koloid Osmotik = 70 – 20 – 32 = 18 mmHg

56
DIURETIKA Zat yg dpt meningkatkan kec.pembentukan urine Cara :
Meningkatkan GFR Mengurangi reabsorpsi cairan dlm tubuh Terapi : Edema , Hipertensi Mekanisme kerja : Meningkatkan muatan osmotik koloid tubuh Menghambat ADH

57
MENINGKATKAN GFR Cara : Tek darah > Vasodilatasi vasa afferent
Vasokonstriksi vasa efferent Tek. Osmotik Koloid <

58
BEBERAPA JENIS OBAT EPINEPHRINE : Tek darah Tek Caps Bowman GFR Diuresis DIGITALIS : Decompensatio Cordis sirkulasi diperbaiki P Bowman GFR Diuresis THEOPHYLIN & CAFFEIN : Vasodilatasi Vasa Aff. P Bowman GFR Diuresis

59
MENINGKATKAN MUATAN OSMOTIK TUBULUS
Mempunyai efek terutama di tub. Proks: Ureum, Sukrosa, Manitol, Glukosa Menghambat Reabsopsi Na+ Di Ansa Henle : Furosemide, Ethacrynil Acid Di Tub. Distal bgn Proksimal : thiazide, metalazone Di tub. Distalis bgn Distal : spironolactone, amiloride

60
Menghambat ADH ADH reabsorpsi H2O di Ductus colligentes diuresis Alkohol, narkotika, anastesi

61
Figure 26.11 The Response to a Reduction in the GFR
Figure 26.11a

62
Figure 26.11 The Response to a Reduction in the GFR
Figure 26.11b

63
Figure 26.16 A Summary of Renal Function

64
Figure 26.15 The Effects of ADH on the DCT and Collecting Ducts

65
Figure 26.15 The Effects of ADH on the DCT and Collecting Ducts
Figure 26.15a, b

Presentasi serupa









>")









