Upload presentasi
1
Penanganan Gizi Obesitas
Putu Amrytha Sanjiwani, S.Gz Disampaikan Pada Kuliah Terapi Dietetik Obesitas

2
Obesitas di Indonesia (Depkes RI)
")
3
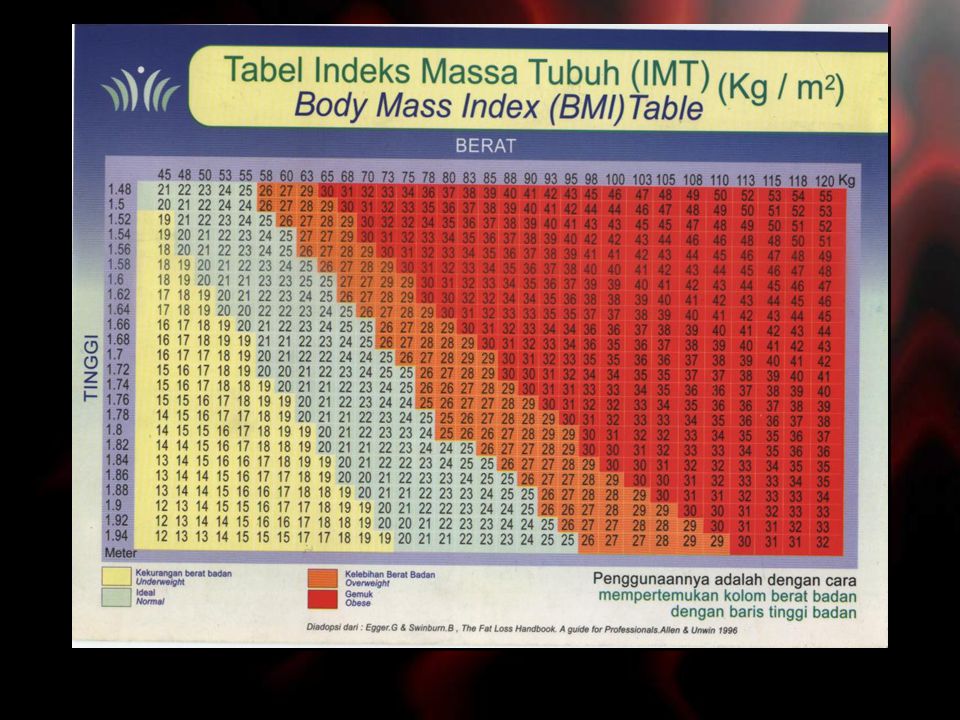
Bagaimana mengetahui Obesitas ? Ukur Tebal Lemak Bawah Kulit
Ukur TB & BB Ukur Tebal Lemak Bawah Kulit Indeks Broca : BB normal = TB-100 , BB ideal = BB normal – 10%, Obesitas > 20% BB normal. Indeks Massa Tubuh (BMI ). - kurus < normal 18-23 - overweight obese > 27 Tebal Lipatan Kulit (Mayer) daerah tricep - pria > 16 mm - wanita > 28 mm
. - kurus < normal overweight obese > 27. Tebal Lipatan Kulit (Mayer) daerah tricep. - pria > 16 mm. - wanita > 28 mm.")
5
Klasifikasi BMI pada Populasi Dewasa Asia
Classification BMI (kg/m2) Risk of Co-morbidities Underweight < 18.5 kg/m2 Low (but ↑risk of clinical problem) Normal range kg/m2 Average Overweight: > 23 At Risk 23.0 – 24.9 kg/m2 Increased Obese I kg/m2 Moderate Obese II > 30.0 kg/m2 Severe
 Risk of Co-morbidities. Underweight. < 18.5 kg/m2. Low (but ↑risk of clinical problem) Normal range kg/m2. Average. Overweight: > 23. At Risk – 24.9 kg/m2. Increased. Obese I kg/m2. Moderate. Obese II. > 30.0 kg/m2. Severe.")
6
Ukur Lingkar Pinggang Obesitas sentral (gemuk perut)
Lingkar pinggang & lingkar panggul: resiko CVD, DM, Ht, dyslipidemia (Depress, 1994; Young & Gelskey; Oshough, 1995). Obesitas sentral : >0.95 M; >0.85 F Lingkar Umbilikus: pria > 100 cm wanita > 90cm
. Obesitas sentral : >0.95 M; >0.85 F. Lingkar Umbilikus: pria > 100 cm. wanita > 90cm.")
7
Distribusi lemak tubuh
Gynoid (pear-shape) Android (apple-shape) Ovid-shape
 Android. (apple-shape) Ovid-shape.")
8
Siapa yang bisa kegemukan ?
Semua lapisan umur bisa, tetapi ternyata pria lebih banyak (survey epidemiologi di USA tahun 1990 didapat overweight dan obesitas 25-40% adalah pria), namun lebih banyak wanita yang mengeluh. Pada status sosial ekonomi rendah ternyata (di Amerika) obesitas lebih banyak (30% pada wanita miskin, 16% pada kelas menengah & 5% pada wanita tingkat atas dan kaya.
, namun lebih banyak wanita yang mengeluh. Pada status sosial ekonomi rendah ternyata (di Amerika) obesitas lebih banyak (30% pada wanita miskin, 16% pada kelas menengah & 5% pada wanita tingkat atas dan kaya.")
9
Dimana & kapan bisa terjadi ?
Dimana saja dan kapan saja (baik di negara berkembang maupun negara yang sudah maju, disemua lapisan umur).
.")
10
Mengapa bisa terjadi ? Masukan kalori melebihi pemakaian berlangsung lama > kelebihannya disimpan jari lemak----> obesitas Makanan faktor terpenting penyebab tunggal/ bersama penyakit lain. Bouchard (1991): a. penyebab utama (95%) karena gangguan pola makan (makan dalam jumlah yang banyak; sering ngemil terutama terjadi di sore & malam hari sekitar jam 18 – 24 saat nonton TV; rakus makanan tertentu: kacang, coklat, es krim, bakso yang ternyata kaya karbohidrat dan lemak; b. tak seimbangnya bahan makanan (bergeser ke arah lemak hampir 50% dan dari tepung ke bahan yang mudah diserap yaitu gula) C. 5% faktor genetik.
: a. penyebab utama (95%) karena gangguan pola makan. (makan dalam jumlah yang banyak; sering ngemil terutama terjadi di sore & malam hari sekitar jam 18 – 24 saat nonton TV; rakus makanan tertentu: kacang, coklat, es krim, bakso yang ternyata kaya karbohidrat dan lemak; b. tak seimbangnya bahan makanan (bergeser ke arah lemak hampir. 50% dan dari tepung ke bahan yang mudah diserap yaitu gula) C. 5% faktor genetik.")
11
Penyebab Obesitas: Faktor genetik Faktor lingkungan & perilaku:
Pola & kesenangan makan dini dipelajari dari ortu Kadar lemak makanan yang dikonsumsi Asupan Alkohol Energy expenditure aktifitas fisik Pengaruh Sosio-ekonomi, pendidikan, budaya Mood & cooping strategies Proses menua Kehamilan pada wanita

12
Mengapa kita bertambah gemuk?
Energy OUT Energy IN Energy IN = Energy OUT

13
PENYAKIT AKIBAT OBESITAS

14
5 Prinsip Utama Menejemen Obesitas
Modifikasi Perilaku: 1st line strategi Terapi Gizi Medis & Modifikasi Diit: 2 macam diit yg efektif turunkan BB LCD & VLCD Gaya Hidup Sehat: Aktifitas Fisik Reguler Strategi obat2an: penekan nafsu makan & penghambat penyerapan lemak Operasi

15
Untuk mencegah bagaimanakah langkahnya ?
Kendalikan diri terhadap: a. makan yang tidak mendesak (makan sebelum lapar berhenti sebelum kenyang), b. isi waktu luang tidak dengan ngemil & mengurangi suka iseng (nyobain berbagai macam makanan dan warung makan) , c. berolah raga yang terukur dan teratur (jenis & porsi yang sesuai) d. mengatasi stres yang menjadi latar belakang ngemil (diantaranya dengan selalu rajin berdo’a, serahkan diri kepada TYME
, b. isi waktu luang tidak dengan ngemil & mengurangi suka iseng (nyobain berbagai macam. makanan dan warung makan) , c. berolah raga yang terukur dan teratur (jenis & porsi yang sesuai) d. mengatasi stres yang menjadi latar belakang ngemil. (diantaranya dengan selalu rajin berdo’a, serahkan diri kepada TYME.")
16
PENGATURAN MAKAN RENDAH KALORI SEIMBANG ZAT GIZI
KURANGI KALORI 500 KCAL/ HARI BB ↓ 0.5 KG / MINGGU Makan 5-6x sehari, Porsi kecil, Harus sarapan Banyak minum, cairan tingkatkan rasa kenyang Banyak serat makanan lama mengunyah, rendah kalori, cepat kenyang Waktu/ lamanya makan minimal 20 menit Makan perlahan2, kunyah dengan baik

17
Terapi Gizi Medis Pada Obesitas
Rendah Kalori Seimbang BB lama; tidak ada efek samping Tidak sesuai harapan pasien Program BB komersial cepat tapi ada efek samping

18
Terapi Gizi Medis (TGM) Medical Nutrition Therapy (MNT) Pada Obesitas
Jumlah energi (energy content) Komposisi Makronutrien (macronutrient composition) Keaneka-ragaman pangan (Food variety) Besar porsi (Portion size) Kombinasi diet & aktivitas fisik Kombinasi diet & obat-obatan
 Komposisi Makronutrien (macronutrient composition) Keaneka-ragaman pangan (Food variety) Besar porsi (Portion size) Kombinasi diet & aktivitas fisik. Kombinasi diet & obat-obatan.")
19
Jumlah Energi: Diit Rendah Kalori Low Calorie Diets/ LCDs
The weight reducing dietary regiment tailored to an individual need initially should provide a kcal/d energy deficit, based on estimated initial maintenance energy This may be best achieved by a reduction in overall fat & CHO intake Gradual weight loss: 0.5-1kg/ week

20
Diet Sangat Rendah Kalori (Very Low Calorie Diet/ VLCD)
The used of VLCD should be advised by specialist doctor and be monitored for adversed reaction The VLCD provide calorie kcal/d, protein 30-40% of total calorie VLCD may occasionally be useful for rapid weight loss prior to a surgical procedure Very rapid weight loss

21
Komposisi Makronutrien Recommended Nutrient Content of a Weight-Reducing Diet
8%-10% Saturated fatty acids Polyunsaturated fatty acids Monounsaturated fatty acids Protein 15% <10% Fat <30% Carbohydrate >55% <15% Recommended nutrient content of a weight-reducing diet Dietary guidelines proposed by the National Institutes of Health [1] recommend a 500 kcal/d deficit for overweight persons (BMI kg/m2) who have obesity-related complications, and for persons with class I obesity (BMI kg/m2). This energy deficit will result in approximately a 1-lb (0.45 kg) weight loss per week and about a 10% weight reduction at 6 months. A kcal/d deficit is recommended for those with class II (BMI kg/m2) or class III (BMI 40 kg/m2) obesity, which will produce about a 1- to 2-lb weight loss per week and a 10% weight loss at 6 months. The recommended macronutrient composition for a low-calorie weight loss diet is shown in this figure and includes 55% or more of daily calories from carbohydrates, 15% from protein, and 30% or less from fat. In addition, specific recommendations are made regarding the composition of fat ingestion: total energy intake should be comprised of 8%-10% calories from saturated fat, 10% or less calories from polyunsaturated fats, and 15% or less calories from monounsaturated fats. Daily cholesterol intake should not exceed 300 mg/d, and daily fiber intake should be between g/d. National Institutes of Health, National Heart, Lung, and Blood Institute. Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults – The Evidence Report. Obes Res. 1998;6(suppl 2):51S-209S. Calories: kcal/d reduction Cholesterol: <300 mg/d Fiber: g/d Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults– The Evidence Report. Obes Res. 1998;6 (suppl 2).
 who have obesity-related complications, and for persons with class I obesity (BMI kg/m2). This energy deficit will result in approximately a 1-lb (0.45 kg) weight loss per week and about a 10% weight reduction at 6 months. A kcal/d deficit is recommended for those with class II (BMI kg/m2) or class III (BMI 40 kg/m2) obesity, which will produce about a 1- to 2-lb weight loss per week and a 10% weight loss at 6 months. The recommended macronutrient composition for a low-calorie weight loss diet is shown in this figure and includes 55% or more of daily calories from carbohydrates, 15% from protein, and 30% or less from fat. In addition, specific recommendations are made regarding the composition of fat ingestion: total energy intake should be comprised of 8%-10% calories from saturated fat, 10% or less calories from polyunsaturated fats, and 15% or less calories from monounsaturated fats. Daily cholesterol intake should not exceed 300 mg/d, and daily fiber intake should be between g/d. National Institutes of Health, National Heart, Lung, and Blood Institute. Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults – The Evidence Report. Obes Res. 1998;6(suppl 2):51S-209S. Calories: kcal/d reduction. Cholesterol: <300 mg/d. Fiber: g/d. Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults– The Evidence Report. Obes Res. 1998;6 (suppl 2).")
22
Aneka-ragam Pangan-Meal Variety
Increase meal variety with different taste will increase : Energy intake Positive energy balance Weight balance Stubbs et al, European J.of Clin. Nutr., 2001 * Same food at each course Different food at each course Energy Intake (kJ) 1 2 3 4 Total Meal Course *P<0.001 vs same food at each course. Rolls et al. Appetite 1984;5:337.
 Total. Meal Course. *P<0.001 vs same food at each course. Rolls et al. Appetite 1984;5:337.")
23
Besar Porsi - Portion Size
There is a linear relationship between portion size served and energy intake: increasing the portion size increased the amount that was consumed. Amount Consumed (g) Effect of portion size on energy intake Food portion size affects energy intake. In this study, young adult men and women were served four different portions of macaroni and cheese for lunch on different days, and were allowed to consume as much food as they liked [1]. The data demonstrate a linear relationship between portion size served and intake: increasing the amount of macaroni and cheese served increased the amount that was consumed. Rolls BJ, Morris EL, Roe LS. Portion size of food affects energy intake in normal-weight and overweight men and women. Am J Clin Nutr 2002 Dec;76(6): 500 625 750 1000 Amount of Macaroni and Cheese Served (g) Rolls et al. Am J Clin Nutr Dec;76(6):
 Effect of portion size on energy intake. Food portion size affects energy intake. In this study, young adult men and women were served four different portions of macaroni and cheese for lunch on different days, and were allowed to consume as much food as they liked [1]. The data demonstrate a linear relationship between portion size served and intake: increasing the amount of macaroni and cheese served increased the amount that was consumed. Rolls BJ, Morris EL, Roe LS. Portion size of food affects energy intake in normal-weight and overweight men and women. Am J Clin Nutr 2002 Dec;76(6): Amount of Macaroni and Cheese Served (g) Rolls et al. Am J Clin Nutr Dec;76(6):")
24
Pedoman makan JANGAN LEWATKAN SARAPAN SNACK BUAH2AN: PAGI SIANG
Diit Rendah Kalori 1500 JANGAN LEWATKAN SARAPAN SNACK BUAH2AN: PAGI SIANG SORE Makan, Timbang, Olah Raga Makan ½ dari biasanya Rendah MAL (Manis, Asin, & Lemak)
")
25
Beberapa Tips Buat rencana menu & daftar belanja.beli mak. Rendah kalori trt saat lapar Jangan lewatkan waktu makan. Makan & kunyah perlahan2. Bersihkan meja dari makanan. Minta tolong keluarga & teman Sisakan mak dalam piring, pilih piring yang relatif kecil Simpan mak. Hanya di dapur Cicipi mak. Hanya sekali saja Biarkan org lain bersihkan piringnya

26
Terima Kasih, Matur Nuwun,
Thank You, Mbue Bujur









 merupakan salah satu masalah yang ditakuti remaja, khususnya remaja putri. Mereka merasa kehilangan.>")











