Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
RESPIRATORY GAS TRANSPORT
Biochemistry Departement Medical Faculty Of Andalas University Padang

3
Oxygen Transport

4
Total Body Oxygen Stores
Oxygen in the Lung (~500 ml O2). Oxygen in the Blood (~850 ml O2). Oxygen in the Cells (very little except Mb-bound). 5
. Oxygen in the Blood (~850 ml O2). Oxygen in the Cells (very little except Mb-bound). 5.")
6
At the Lung Level 10

7
At the Tissue Level 10

8
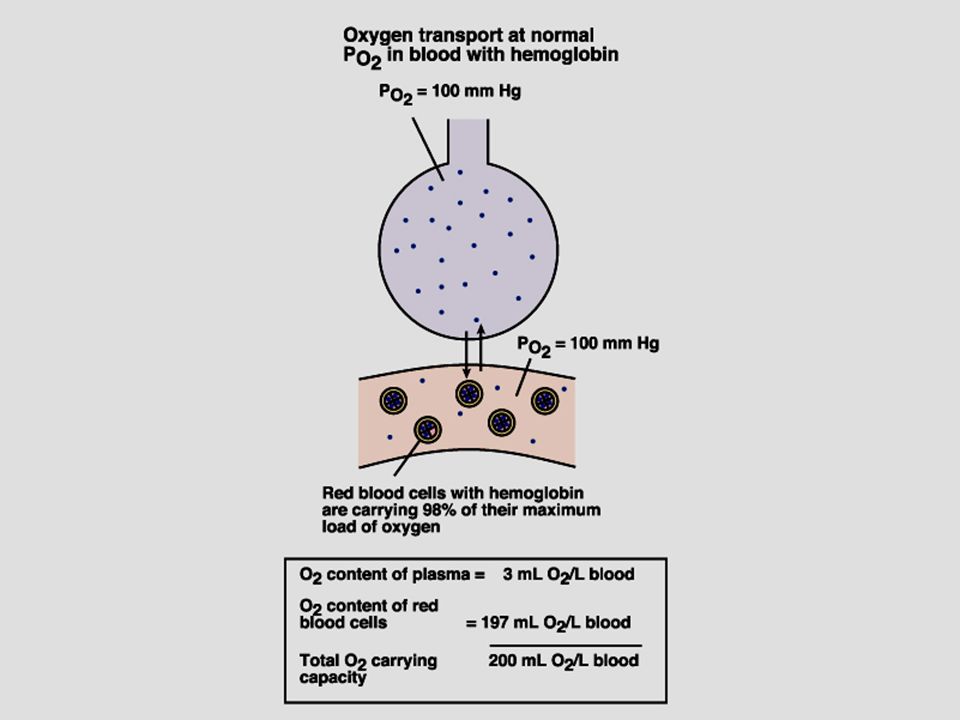
Oxygen Is Carried in Blood in 2 Forms
Bound to hemoglobin in red blood cells. Dissolved in plasma. Normally insignificant. 13

9
Hemoglobin Each “heme” molecule is capable of binding with 1 O2 molecule and each “globin” molecule is capable of binding with 1 CO2 molecule. So, each molecule of Hb can bind to either 4 molecules of O2 and 1 molecule of CO2 100 ml of blood has about 15 gm of Hb, at Hct = 0.45

10
Binding of O2 to 4 heme sites given by:
Equilibrium constants for different reactions different Binding of first O2 relatively low affinity 2nd, 3rd and 4th - much higher affinity

11
Oxygen as Oxyhemoglobin
Each gram of Hb can store about 1.34 ml of O2: 1 L of blood (150 gm of Hb) can store about 208 ml of O2 Oxygen Capacity of Hb. With normal cardiac output, about 1040 ml of O2 can be carried in blood per minute. (4 times of the metabolic demands).
 can store about 208 ml of O2 Oxygen Capacity of Hb. With normal cardiac output, about 1040 ml of O2 can be carried in blood per minute. (4 times of the metabolic demands).")
14
O2 Saturation. Units: percent.
Fraction or percentage of all the hemoglobin binding sites that are currently occupied by oxygen. 17

15
Oxygen Saturation of Hb
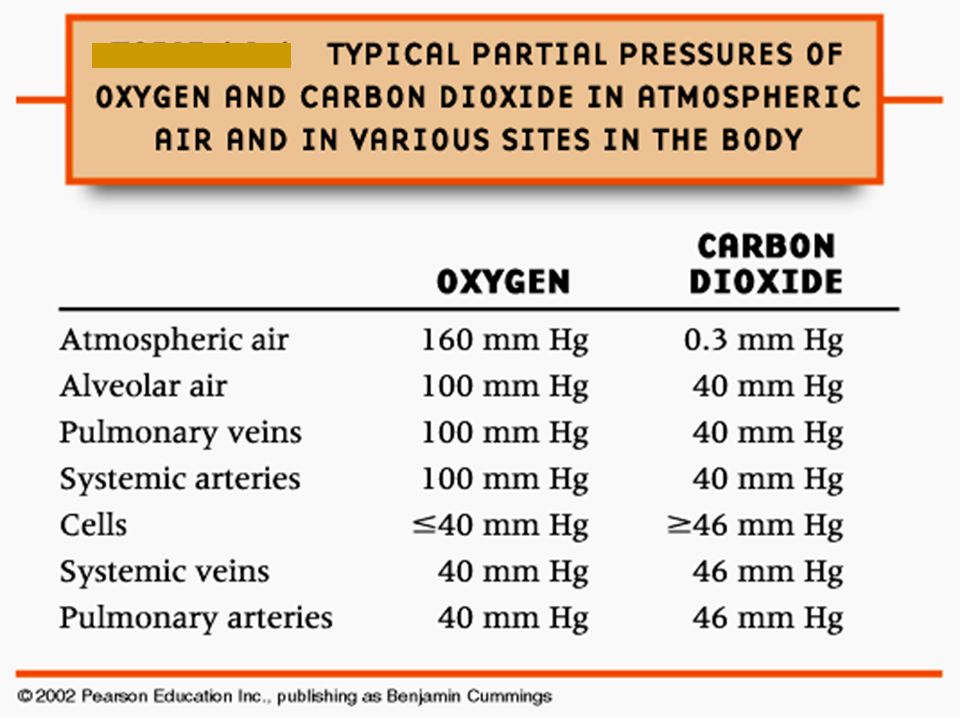
Saturation at the arterial end (PO2 = 100 mmHg) is about 97% and oxygen content of blood is about 20 ml of O2 per 100 ml of blood. Saturation at the venous end (pO2 = 40 mmHg) is about 75% and oxygen content of blood is about 15 ml of O2 per 100 ml of blood. P50 is about 26 mmHg. Concentration of bound oxygen is considerably high compared to that of the dissolved oxygen. The saturation profile is mostly flat in the physiological range of PO2 (40 mmHg – 100 mmHg).
 is about 97% and oxygen content of blood is about 20 ml of O2 per 100 ml of blood. Saturation at the venous end (pO2 = 40 mmHg) is about 75% and oxygen content of blood is about 15 ml of O2 per 100 ml of blood. P50 is about 26 mmHg. Concentration of bound oxygen is considerably high compared to that of the dissolved oxygen. The saturation profile is mostly flat in the physiological range of PO2 (40 mmHg – 100 mmHg).")
16
Four (5-6?) Things Change Oxyhemoglobin Affinity
Hydrogen Ion Concentration, [H+] Carbon Dioxide Partial Pressure, PCO2 Temperature [2,3-DPG] Special Case: Carbon Monoxide Hemoglobin variants 31

18
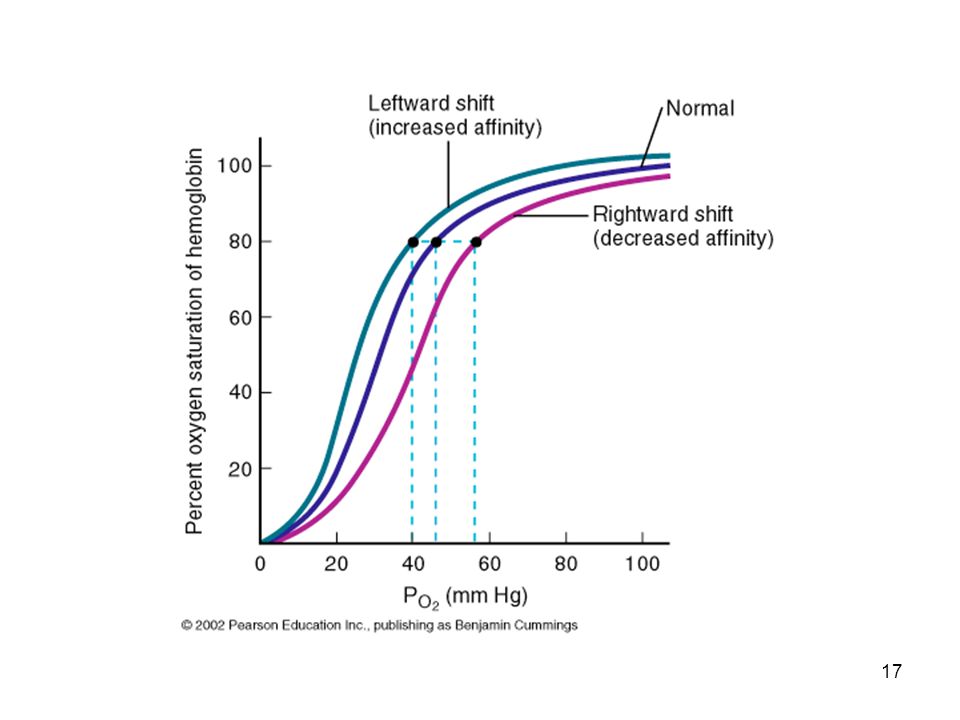
Factors Affecting Hb-O2 Affinity: Summary
Hydrogen Ion: Increased H+ (decreased pH) increases H+ binding to Hb and reduces O2 affinity (HbO2+H+HbH++O2). Carbon Dioxide (Bohr effect): Increased PCO2 increases CO2 binding to Hb and reduces O2 affinity (increased O2 delivery to tissue). Increased PCO2 increases H+ and reduces O2 affinity (fixed acid Bohr effect). Temperature and 2,3-DPG (diphosphoglycerate): Increased temperature and 2,3-DPG reduces O2 affinity. Normal CO2 Bohr’s effect and fixed acid Bohr’s effect. CO2 hydration reaction in RBCs is catalyzed by the Carbonic Anhydrase (CA).
 increases H+ binding to Hb and reduces O2 affinity (HbO2+H+HbH++O2). Carbon Dioxide (Bohr effect): Increased PCO2 increases CO2 binding to Hb and reduces O2 affinity (increased O2 delivery to tissue). Increased PCO2 increases H+ and reduces O2 affinity (fixed acid Bohr effect). Temperature and 2,3-DPG (diphosphoglycerate): Increased temperature and 2,3-DPG reduces O2 affinity. Normal CO2 Bohr’s effect and fixed acid Bohr’s effect. CO2 hydration reaction in RBCs is catalyzed by the Carbonic Anhydrase (CA).")
19
Effect of CO & Anemia on Hb-O2 Affinity
Carbon monoxide (CO) and O2 bind reversibly to the same site on the hemoglobin molecule. Binding of CO prevent O2 binding. Because hemoglobin has an affinity for CO that is about 250 times greater than that for O2, it takes a small amount of CO to displace O2 from the heme binding site. CO binding not only decreases the O2 content but also increases the hemoglobin-oxygen affinity of the remaining heme sites. The resulting O2 equilibrium curve is reduced in magnitude as well as shifted to the left. The venous PO2 is reduced, due both to a lower O2 content and a higher O2 affinity. Normal blood with Hb=15 gm/dl, anemia with Hb=7.5 gm/dl, and normal blood with 50% HbCO (carboxyhemoglobin).
 and O2 bind reversibly to the same site on the hemoglobin molecule. Binding of CO prevent O2 binding. Because hemoglobin has an affinity for CO that is about 250 times greater than that for O2, it takes a small amount of CO to displace O2 from the heme binding site. CO binding not only decreases the O2 content but also increases the hemoglobin-oxygen affinity of the remaining heme sites. The resulting O2 equilibrium curve is reduced in magnitude as well as shifted to the left. The venous PO2 is reduced, due both to a lower O2 content and a higher O2 affinity. Normal blood with Hb=15 gm/dl, anemia with Hb=7.5 gm/dl, and normal blood with 50% HbCO (carboxyhemoglobin).")
20
Exercise Increase temperature Increased PCO2 and
Decreased pH (acidosis) 37
 37.")
21
2,3-DPG 2,3-DPG is a glycolytic intermediate
accumulates to uniquely high levels in RBCs -Increased 2,3-DPG right shift -Decreased 2,3-DPG left shift Increased 2,3-DPG associated with hypoxia. 38

22
Conditions with Increased 2,3-DPG
acclimatization to high altitudes. chronic lung disease; emphysema. anemia. hyperthyroidism. right to left shunt. congenital heart disease. pulmonary vascular disease. 39

23
Blood Bank Storage CPD (citrate phosphate dextrose) Storage 2,3-DPG depletion O.D.C. left-shifted oxygen Oxygen unloading impaired 40

24
Carbon Dioxide Transport

25
At the Tissue Level

26
At the Lung Level

27
Carbon Dioxide Transport
CO2 is transported in blood in dissolved form, as bicarbonate ions, and as protein-bound carbamino compound. Protein-bound CO2 (carbamino compounds): Amount of CO2 stored as carbamino compounds is about 21 ml/L (4% of the total art CO2).
: Amount of CO2 stored as carbamino compounds is about 21 ml/L (4% of the total art CO2).")
28
Carbon Dioxide Transport
A majority amount of CO2 is transported in the form of bicarbonate ions (HCO3-): Amount of CO2 in HCO3- form at PCO2=40 mmHg is about 420 ml/L (90% of the total arterial CO2).
: Amount of CO2 in HCO3- form at PCO2=40 mmHg is about 420 ml/L (90% of the total arterial CO2).")
29
Carbon Dioxide Transport
Haldane Effect: Increasing O2-saturation reduces CO2 content and shifts the CO2 dissociation curve to right. This is because, increasing PO2 leads to : Decrease in the formation of carbamino compound. Release of H+ ions from the hemoglobin and resulting in dehydration of HCO3-.

30
Carbon Dioxide Dissociation Curve
Over the normal physiological range (PCO2 = 30 to 55 mmHg and PO2 = 40 to 100 mmHg), the CO2 equilibrium curve is nearly linear. But, O2 equilibrium curve is highly nonlinear.
, the CO2 equilibrium curve is nearly linear. But, O2 equilibrium curve is highly nonlinear.")
31
61

32
Bicarbonate in RBCs. • Percent of the total PaCO2: 70%
Carbonic anhydrase is present in RBCs CO2 forms carbonic acid which dissociates to H+ and HCO3- Released H+ is buffered by histidine residues (imidazole group) • Percent of the total PaCO2: 70% 54
 • Percent of the total PaCO2: 70% 54.")
33
Carbamino Compounds in RBCs.
Approximately 30% of RBC contents is Hb CO2 forms carbamino hemoglobin Released H+ is buffered by histidine residues (imidazole group) • Percent of the total PaCO2: 23 % 53
 • Percent of the total PaCO2: 23 % 53.")
34
CO2 Formation in Plasma Carbamino compounds
CO2 binds the amine groups of plasma proteins to form carbamino compounds. 51

35
O2 pickup CO2 release

36
O2 release CO2 pickup

37
Chloride Shift (Hamburger Shift)
Newly formed HCO3- passes out of RBC Cl- diffuses into RBC to maintain electroneutrality Chloride shift is rapid Complete before the RBCs exit capillary 56

38
Tissue-Gas Exchange: Summary
Gas exchange processes in the peripheral organs are essentially opposite those in the lungs. O2 is released from the capillary blood to the tissues and diffuses to the mitochondria where O2 is converted to CO2 and energy (ATP) through cellular metabolism. CO2 diffuses from the tissues to the blood stream and is transported to the lungs for elimination. The exchange of O2 and CO2 in the blood-tissue exchange unit depends on PO2, PCO2, and also on O2 and CO2 saturation curves.
 through cellular metabolism. CO2 diffuses from the tissues to the blood stream and is transported to the lungs for elimination. The exchange of O2 and CO2 in the blood-tissue exchange unit depends on PO2, PCO2, and also on O2 and CO2 saturation curves.")
39
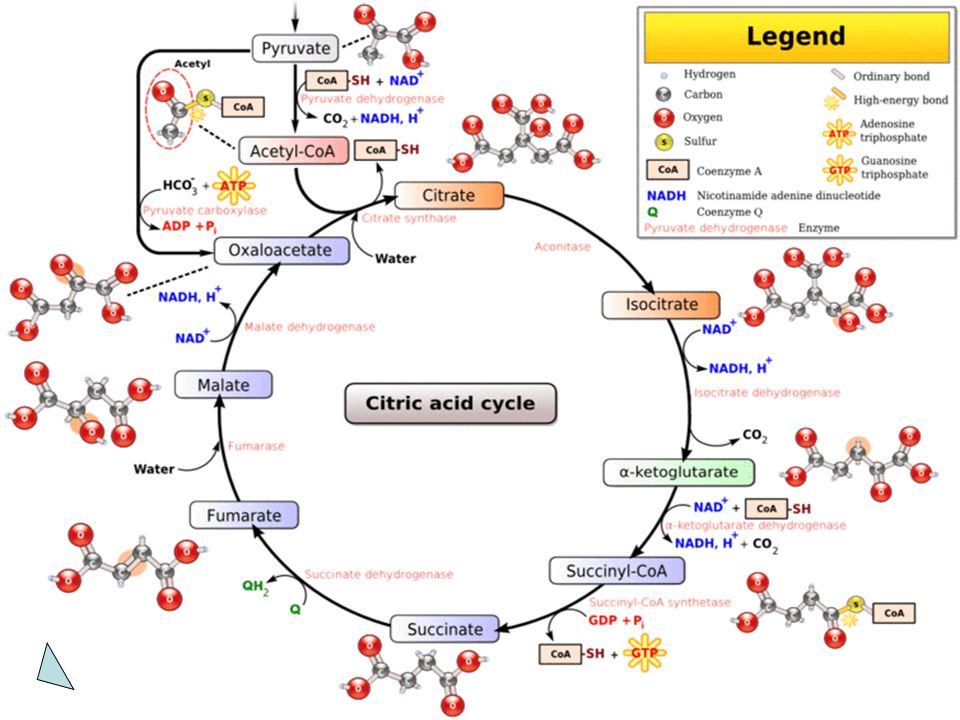
Gas Transport in Cell

41
Pelepasan CO2 Dilakukan oleh: 1. isositrat dehidrogenase
2. α-ketoglutarat dehidrogenase Pelepasan CO2 tidak mengkonsumsi oksaloasetat.

42
Siklus ATP/ADP Berperan untuk menghubungkan proses-proses yg menghasilkan P-berenergi-tinggi dgn proses yg menggunakan P-berenergi-tinggi. ATP dikonsumsi & dibentuk kembali secara kontinu. Depot ATP/ADP sangat kecil, sehingga hanya cukup untuk mempertahankan jaringan aktif dlm waktu beberapa detik saja.

43
Siklus ATP/ADP ATP CO2 Pernapasan: Penggunaan energi:
pembentukan energi biosintesis makro- dari; - karbohidrat molekul - lemak kontraksi otot - protein transpor ion aktif - termogenesis O2 ADP + Pi

44
Fosforilasi Oksidatif
Adalah sistem dalam mitokondria yang memasangkan respirasi dengan proses pembentukan intermediat berenergi tinggi, ATP. Sistem ini memungkinkan organisme aerob menangkap energi bebas dari substrat respiratorik dalam jumlah lebih besar dibanding organisme anaerob.

45
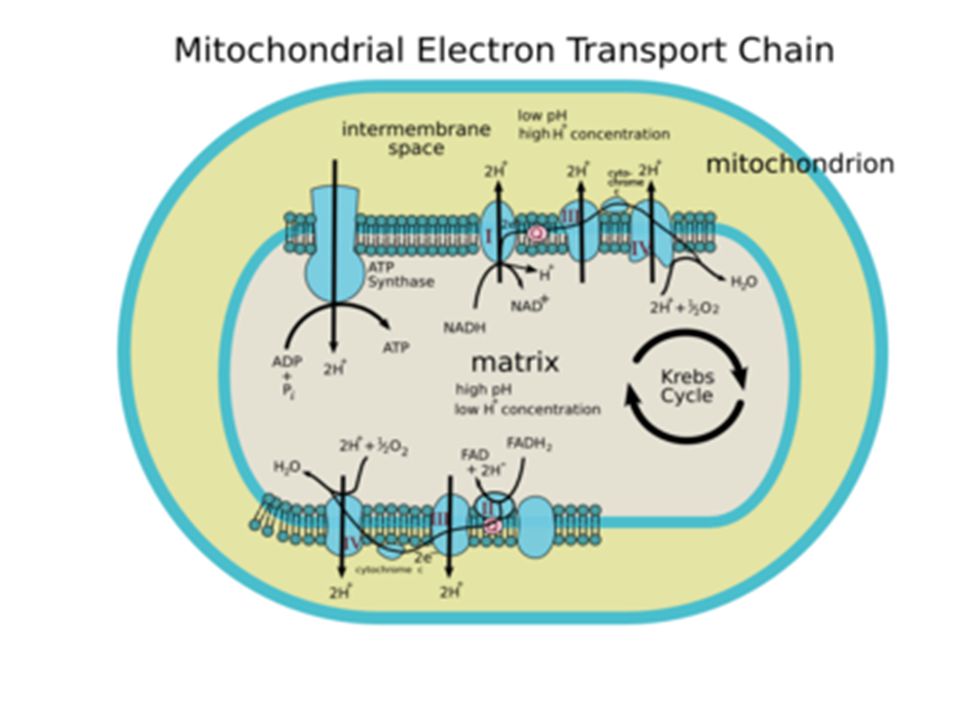
Peran Rantai Respirasi
asam lemak b-oksidasi gliserol ATP O2 glukosa Asetil KoA SAS H H2O rantai respirasi Asam amino ADP mitokondria

47
Produk ATP pada Fosforilasi Oksidatif
Berdasarkan hipotesis kimiosmotik dari Mitchell yaitu; rantai bekerja --> proton dipompa keluar dari membran dlm mitokondria --> pH antar membran turun --> proton balik ke dalam matrik lewat tonjolan ATP-sintase--> fosforilasi ADP menjadi ATP.

48
Produk ATP pada Fosforilasi Oksidatif
Diperkirakan satu ATP disintesis setiap dua proton melewati tonjolan tsb. Hasilnya ialah; - 3 mol. ATP utk oksidasi 1 mol. NADH - 2 mol. ATP utk oksidasi 1 mol. FADH2 Laju fosforilasi oksidatif dikendalikan oleh; NADH, oksigen, ADP

49
Resources BIOEN 589: Integrative Physiology. Download 24 jan 05.
Kennelly, PJ., Rodwell, V W. Proteins: Myoglobin & Hemoglobin. In: Harper’s Illustrated Biochemistry. 27th Ed Miliefsky, M. Respiratory System Ch.23. Download 24 Nov 10. Sheardown, H. Blood Biochemistry. McMaster University. Download 20 Mei 07. Irvin, CG. Respiratory Physiology. Lecture 4A CO2 Transport. In: MEDICAL PHYSIOLOGY 30. Download 22 Jun 09. Marks, DB., Marks, AD., Smith CM. Basic medical biochemistry: a clinical approach Dalam: B.U. Pendit, penerjemah. Biokimia Kedokteran Dasar: Sebuah Pendekatan Klinis. Eds. J. Suyono., V. Sadikin., L.I. Mandera. Jakarta: EGC, 2000 R.K. Murray, D.K. Granner, P.A. Mayes, V.W. Rodwell Harper’s Biochemistry. 27th ed. McGraw-Hill Companies, New York

Presentasi serupa







 untuk.>")













>")