Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
FACULTY OF MEDICINE MALANG ISLAMIC UNIVERSITY
SKIN TEST

2
Applying the tuberculin skin test
Courtesy of Dr. Marc Steben The MTCT-Plus Initiative

3
Applying the tuberculin skin test
The MTCT-Plus Initiative

4
Applying the tuberculin skin test
Courtesy of Dr. Marc Steben The MTCT-Plus Initiative

5
Reading the tuberculin skin test
Read 2-3 days after placing the test Feel for induration Color change without induration is not included in the measurement Use a ruler or calipers Have someone else check if unsure Always document the exact size (mm) – not just “positive” or “negative” The MTCT-Plus Initiative
 – not just positive or negative The MTCT-Plus Initiative.")
6
Reading the tuberculin skin test
Courtesy of Dr. Marc Steben The MTCT-Plus Initiative

7
Reading the tuberculin skin test
The MTCT-Plus Initiative

12
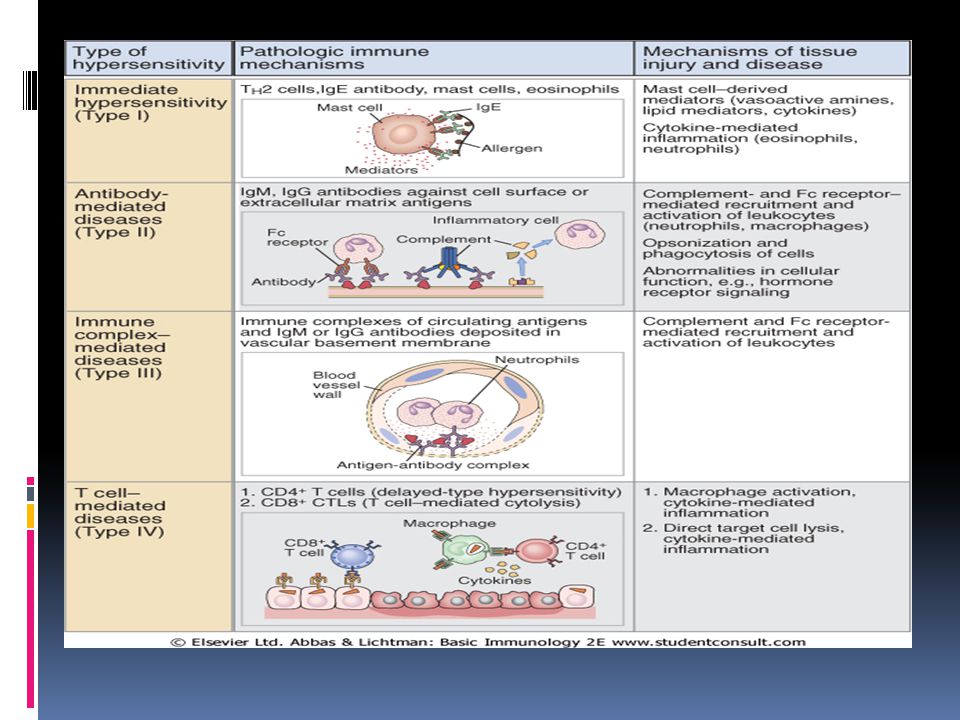
REAKSI HIPERSENSITIVITAS
Y Y REAKSI HIPERSENSITIVITAS

13
Hipersensitivitas adalah suatu reaksi yang tidak diharapkan dari respon imun tubuh.
Coombs dan Gell membagi menjadi 4 tipe (mekanisme dan waktu): Rx. Hipersensitivitas tipe I Rx. Hipersensitivitas tipe II Rx. Hipersensitivitas tipe III Rx. Hipersensitivitas tipe IV
: Rx. Hipersensitivitas tipe I. Rx. Hipersensitivitas tipe II. Rx. Hipersensitivitas tipe III. Rx. Hipersensitivitas tipe IV.")
15
4 types of hypersensitivity reactions
(hives) Allergies
 Allergies.")
16
Delayed-type hypersensitivity
Immune complex disease Delayed-type hypersensitivity

17
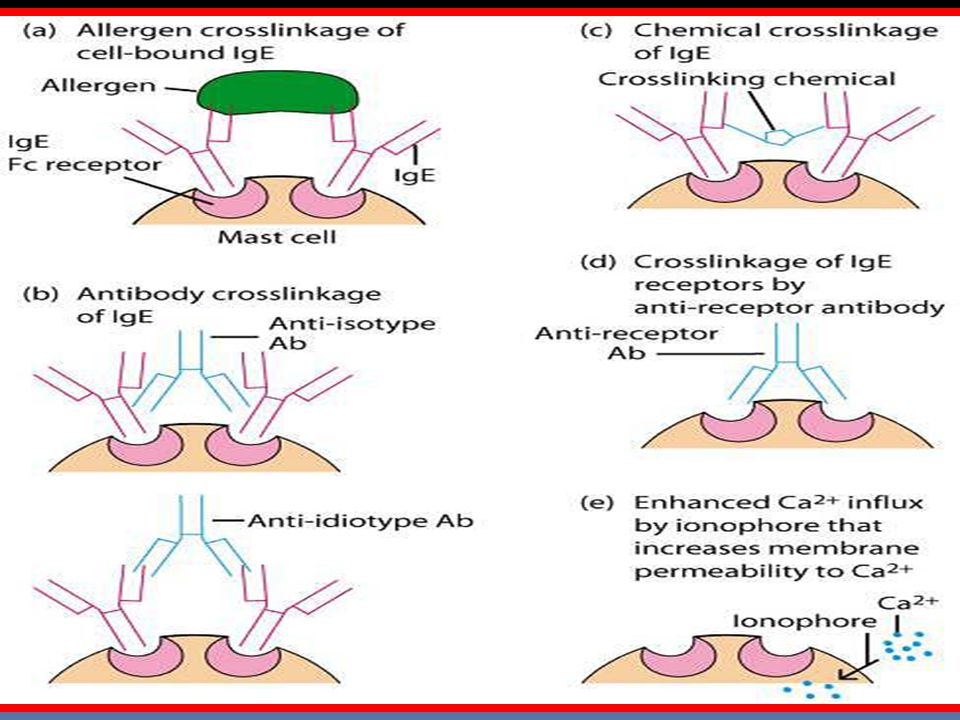
Reaksi Hipersensitivitas tipe I
Reaksi Hipersensitivitas tipe cepat atau anafilaktik Diperantarai IgE Alergenproduksi IgE berikatan spesifik dengan reseptor di permukaan sel mast dan basofil tersensitisasi Kontak berikutnya sederetan reaksi biokimia degranulasi dan pelepasan mediator2 (histamin, leukotrien dan sitokin) reaksi alergi 15-30 menit setelah terpapar antigen, kadang keterlambatan (10-12 jam) Dapat melibatkan kulit (urtikaria dan eksema), mata (konjungtivitis), nasofaring (rinitis), jaringan bronkopulmoner (asma), dan GI tract (gastroenteritis)
 reaksi alergi menit setelah terpapar antigen, kadang keterlambatan (10-12 jam) Dapat melibatkan kulit (urtikaria dan eksema), mata (konjungtivitis), nasofaring (rinitis), jaringan bronkopulmoner (asma), dan GI tract (gastroenteritis)")
18
Reaksi Hipersensitivitas tipe I……….
Contoh: reaksi anafilaksis terhadap bisa hewan, hay fever, urtikaria akibat makanan, dermatitis atopik, rhinitis alergika, konjungtivitis, asma, dll Gejala : ketidaknyamanan ringan sampai kematian Berat ringan gejala dipengaruhi : antibodi IgE jumlah alergen faktor-faktor lain yang dapat meningkatkan respon (infeksi virus dan polutan)
")
19
Biologic effects of mediators

20
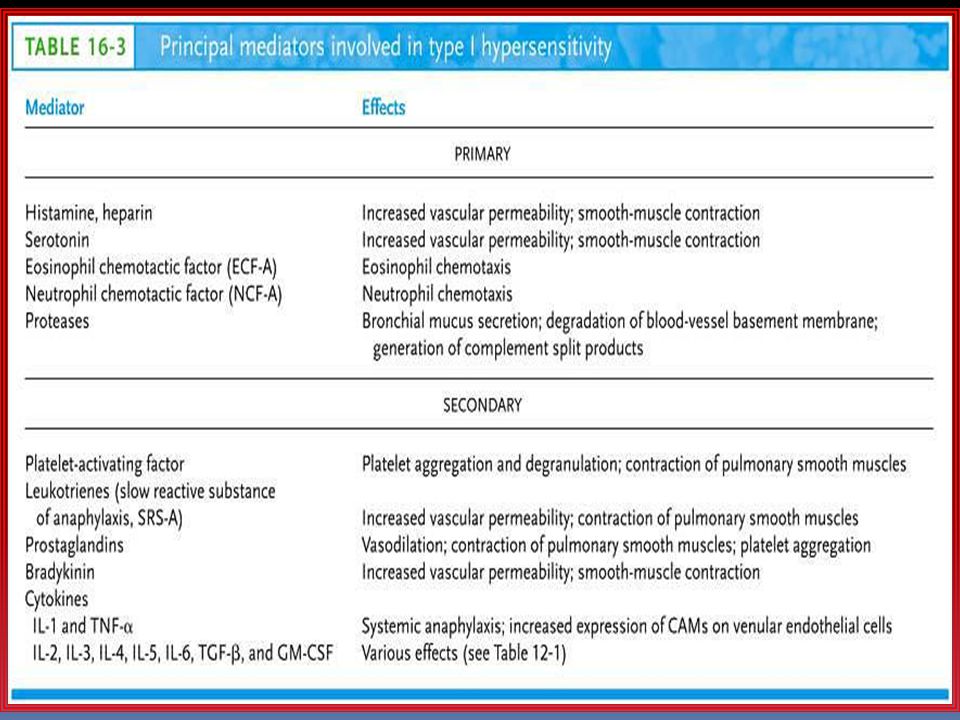
Table 1. Pharmacologic Mediators of Immediate Hypersensitivity
Preformed mediators in granules histamine bronchoconstriction, mucus secretion, vasodilatation, vascular permeability tryptase proteolysis kininogenase kinins and vasodilatation, vascular permeability, edema ECF-A (tetrapeptides) attract eosinophil and neutrophils Newly formed mediators leukotriene B4 basophil attractant leukotriene C4, D4 same as histamine but 1000x more potent prostaglandins D2 edema and pain PAF platelet aggregation and heparin release: microthrombi
 attract eosinophil and neutrophils. Newly formed mediators. leukotriene B4. basophil attractant. leukotriene C4, D4. same as histamine but 1000x more potent. prostaglandins D2. edema and pain. PAF. platelet aggregation and heparin release: microthrombi.")
21
Tes diagnostik Skin test (prick dan intradermal)
Kadar total IgE dan IgE spesifik terhadap alergen yang dicurigai (ELISA) IgE tinggi pada kondisi atopik Terapi: Antihistamin, adrenalin, bronkodilator, kortikosteroid, menghindari paparan alergen dan immunoterapi
 IgE tinggi pada kondisi atopik. Terapi: Antihistamin, adrenalin, bronkodilator, kortikosteroid, menghindari paparan alergen dan immunoterapi.")
22
Skin test for allergy Ragweed Control negative (saline)
Control positve (histamine)
")
23
Type I hypersensitivity reaction
Capillary dilation Pressure of exudate Release of chemical mediators : Histamine SRS-A Kinins Prostaglandins Increased Blood Volume Capillary permebiality Exudation of Cell, fluid protein Nerve irritation Constriction of smooth muscle Antigen Ingestants Food Drugs Pollens Dusts Molds Injectants Stings Vaccines Serum Allergen interacts with IgE on mast cell CAUSES MECHANISM PATHOPHYSIOLOGY Type I hypersensitivity reaction 23

24
Type I hypersensitivity reaction (continued)
MANIFESTATIONS CLINICAL EXAMPLES Gastrointestinal Glossitis, cardiospasm Nausea, vomitting Irritable bowel Diarrhea, pruritus ani Skin Urticaria, pruritus, Angioedema, weeping erthematosus vesico-papular lessions Respiratory tract Upper “sinus headache” itching of eyes tearing, sneezing, watery nasal discharge, itching of nose, throat irritation Lungs wheezing, dyspnea, dry cough, tightness in chest Conjunctivitis Asthma Food allergies Atopic dermatitis Urticaria Allergic rhinitis Respiratory tract Upper “sinus headache” itching of eyes tearing, sneezing, watery nasal discharge, itching of nose, throat irritation Lungs wheezing, dyspnea, dry cough, tightness in chest Type I hypersensitivity reaction (continued) 24
 24.")
26
Reaksi Hipersensitivitas tipe II
Reaksi hipersensitivitas sitotoksik Waktu reaksi : menit - jam Contoh: reaksi transfusi, drug-induced hemolytic anemia, granulositopenia, dan trombositopenia Diperantarai IgM atau IgG dan komplemen Fagosit dan sel K punya peran Interaksi antigen-antibodi pd permukaan sel, IgM atau IgG dgn antigen yang juga merupakan bagian integral membran sel atau telah terserap atau menyatu menjadi membran. Mengaktifkan sistem komplemen dan sel yang terlibat dihancurkan. Terapi: anti-inflamasi dan agen immunosupresif

28
Type II hypersensitivity reaction
CAUSES MECHANISM PATHOPHYSIOLOGY CLINICAL EXAMPLES Susceptability to infections Antigen Transfusion reaction Erythroblastosis fetalis Drugs Autoantibodies Unknown Antigen interacts with body cell i.e : Erythrocyte Leucocyte Platelet Vascular endothelium Agranulocytosis Thrombocytopenia Purpura Vesicular purpura Vasculitis Erytrhrocyte hemolysis Hemolytic anemia Reaction of IgG or IgM antobody with antigen on cell Activates complement Type II hypersensitivity reaction 28

29
Reaksi Hipersensitivitas tipe III
Reaksi hipersensitivitas kompleks imun / reaksi Arthus 3-10 jam setelah terpapar antigen Diperantarai kompleks imun (antigen-antibodi) Antigen eksogen (bakteri, virus, atau parasit)/endogen (SLE) Contoh: serum sickness,SLE,rx Arthus,lupus nephritis,RA,dll Terbentuk kompleks antigen-antibodi (toksik terhadap jaringan di tempat mereka diendapkan seperti ginjal / paru- paru) infiltrasi dinding pembuluh darah kecil aktivasi kaskade komplemen pelepasan bahan aktif secara biologis, termasuk faktor-faktor yang menarik sel-sel fagosit yang akan menfagositosis kompleks tersebut
 Antigen eksogen (bakteri, virus, atau parasit)/endogen (SLE) Contoh: serum sickness,SLE,rx Arthus,lupus nephritis,RA,dll. Terbentuk kompleks antigen-antibodi (toksik terhadap jaringan di tempat mereka diendapkan seperti ginjal / paru- paru) infiltrasi dinding pembuluh darah kecil aktivasi kaskade komplemen pelepasan bahan aktif secara biologis, termasuk faktor-faktor yang menarik sel-sel fagosit yang akan menfagositosis kompleks tersebut.")
30
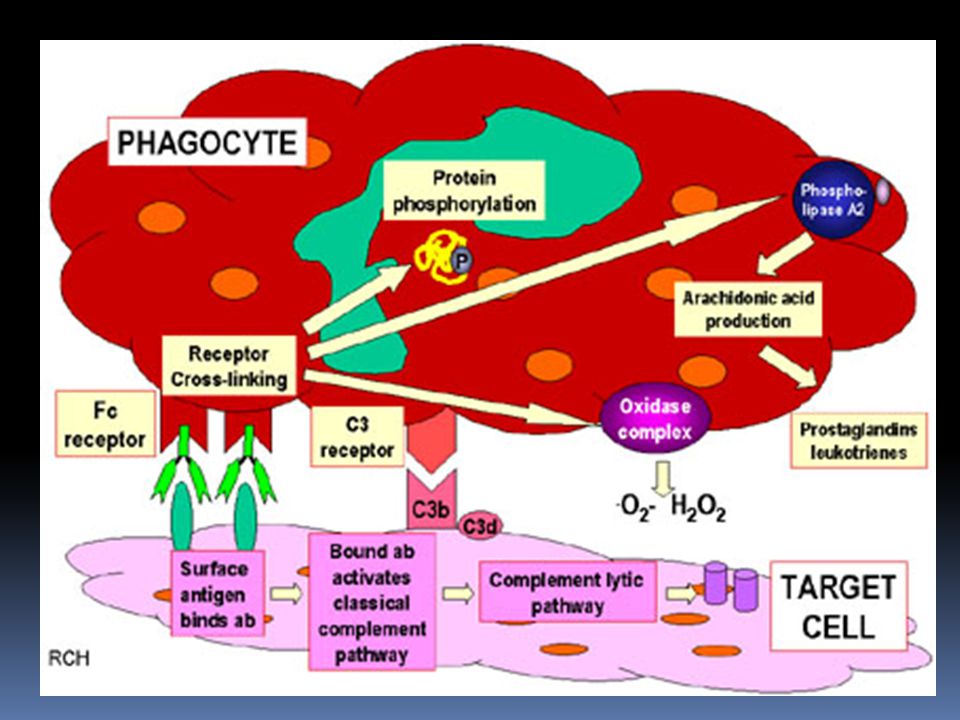
Type III hypersensitivity reactions (Arthus Reaction) - Ab-Ag Complexes
Critical mediators appear to be C5a-receptor and FcgRIII--probably present on mast cells

31
Type III hypersensitivity reaction
CAUSES MECHANISM PATHOPHYSIOLOGY CLINICAL EXAMPLES Tissue destruction Inflammation Antigen and antibody form an immune complex Antigen Autoantibodies Drugs Serum Chemicals Foreign antigen Bacteria Virus Glomerulo-nephritis Vasculitis Arthus reaction Rheumatoid diseases Serum sickness Deposits on vessel walls or basement membrane Type III hypersensitivity reaction 31

32
Diagnosis: Biopsi jaringan (endapan Ig dan komplemen)
Kompleks imun pada darah dan penurunan jumlah komplemen Terapi: Anti-inflamasi

33
Reaksi Hipersensitivitas Tipe IV
tipe seluler atau tipe lambat (delayed type hypersensitivity) > 12 jam Contoh klasik: reaksi tuberkulin (Mantoux) yang memuncak 48 jam setelah injeksi antigen Contoh lain: dermatitis kontak, penyakit autoimun dan infeksi seperti tuberkulosis, lepra, granulomatosa, toksoplasmosis, dll
 > 12 jam. Contoh klasik: reaksi tuberkulin (Mantoux) yang memuncak 48 jam setelah injeksi antigen. Contoh lain: dermatitis kontak, penyakit autoimun dan infeksi seperti tuberkulosis, lepra, granulomatosa, toksoplasmosis, dll.")
34
Biological effects of Eosinophil mediators
Late stage of an allergic response includes the recruitment of eosinophils and Th2 cells contrast with a DTH (type IV) response which includes infiltration of macrophages and Th1 cells
 response which includes infiltration of macrophages and Th1 cells.")
35
Table 3 - Delayed hypersensitivity reactions
Type Reaction time Clinical appearance Histology Antigen and site contact 48-72 hr eczema lymphocytes, followed by macrophages; edema of epidermis epidermal ( organic chemicals, poison ivy, heavy metals, etc.) tuberculin local induration lymphocytes, monocytes, macrophages intradermal (tuberculin, lepromin, etc.) granuloma 21-28 days hardening macrophages, epitheloid and giant cells, fibrosis persistent antigen or foreign body presence (tuberculosis, leprosy, etc.)
 tuberculin. local induration. lymphocytes, monocytes, macrophages. intradermal (tuberculin, lepromin, etc.) granuloma days. hardening. macrophages, epitheloid and giant cells, fibrosis. persistent antigen or foreign body presence (tuberculosis, leprosy, etc.)")
36
Mekanisme perusakan melibatkan limfosit T dan monosit dan/atau makrofag
Sel t sitotoksik (Tc) menyebabkan kerusakan langsung sedangkan sel T helper (TH1) mensekresi sitokin aktivasi Tc, makrofag serta monosit kerusakan Diagnosis: Mantoux test dan patch test Terapi: - Kortikosteroid dan agen imunosupresif
 menyebabkan kerusakan langsung sedangkan sel T helper (TH1) mensekresi sitokin aktivasi Tc, makrofag serta monosit kerusakan. Diagnosis: Mantoux test dan patch test. Terapi: - Kortikosteroid dan agen imunosupresif.")
37
Type IV hypersensitivity reaction
CAUSES MECHANISM PATHOPHYSIOLOGY CLINICAL EXAMPLES Release of : Lymphokines Migration inhibition factor Interferon Killer cells Transfer factor Injury and destruction of target organ Antigen Tuberculin Poison Ivy Chemical Fungi Transplanted organs Virus Contact dermatitis Graft vs host reactions Viral infection Autoallergic disease Sensitized Lymphocyte reacts with antigen Type IV hypersensitivity reaction 37

Presentasi serupa








>")

 Dr. Rahmatini M. Kes Bagian Farmakologi & Terapi>")





>")









