Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
PANKREATITIS AKUT OLEH HADI PURWANTO

2
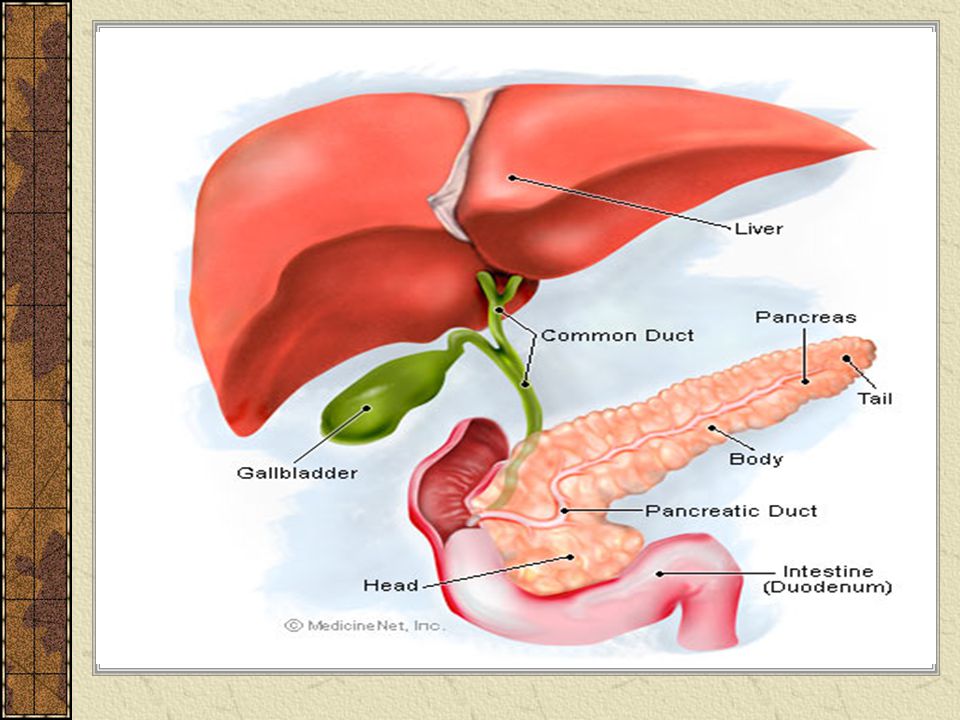
PENDAHULUAN The pancreas is a large gland behind the stomach and close to the duodenum. The duodenum is the upper part of the small intestine. The pancreas secretes digestive enzymes (TRYPSIN, AMYLASE, LIPASE) into the small intestine through a tube called the pancreatic duct. These enzymes help digest fats, proteins, and carbohydrates in food. The pancreas also releases the hormones insulin and glucagon into the bloodstream. These hormones help the body use the glucose it takes from food for energy.
 into the small intestine through a tube called the pancreatic duct. These enzymes help digest fats, proteins, and carbohydrates in food. The pancreas also releases the hormones insulin and glucagon into the bloodstream. These hormones help the body use the glucose it takes from food for energy.")
3
LANJUTAN… Normally, digestive enzymes do not become active until they reach the small intestine, where they begin digesting food. But if these enzymes become active inside the pancreas, they start "digesting" the pancreas itself.

5
PANKREATITIS AKUT Pankreatitis akut adalah reaksi peradangan pankreas yang secara klinis ditandai dengan nyeri perut yang akut disertai kenaikan enzim pankreas dalam darah dan urin Pada pankreatitis akut, didapati autodigesti dari enzim pankreas terhadap sel pankreas sehingga menimbulkan reaksi inflamasi

6
LANJUTAN… Inflamasi dimulai dari perilobuler dan jaringan peripankreas dengan manifestasi edema dan nekrosis setempat Setelah itu, mengenai sel asiner perifer, duktus pankreatikus, pembuluh darah, dan jaringan sekitarnya

7
What are the causes of acute pancreatitis?
Acute pancreatitis is usually caused by gallstones or by drinking too much alcohol, but these aren't the only causes. If alcohol use and gallstones are ruled out, other possible causes of pancreatitis should be carefully examined so that appropriate treatment—if available—can begin.

8
What are the symptoms of acute pancreatitis?
Acute pancreatitis usually begins with pain in the upper abdomen that may last for a few days. The pain may be severe and may become constant—just in the abdomen—or it may reach to the back and other areas Other symptoms may include swollen and tender abdomen nausea vomiting fever rapid pulse

9
How is acute pancreatitis diagnosed?
Besides asking about a person's medical history and doing a physical exam, a doctor will order a blood test to diagnose acute pancreatitis. During acute attacks, the blood contains at least three times more amylase and lipase than usual. Amylase and lipase are digestive enzymes formed in the pancreas. Changes may also occur in blood levels of glucose, calcium, magnesium, sodium, potassium, and bicarbonate. After the pancreas improves, these levels usually return to normal.

10
LANJUTAN… A doctor may also order an abdominal ultrasound to look for gallstones and a CAT (computerized axial tomography) scan to look for inflammation or destruction of the pancreas
 scan to look for inflammation or destruction of the pancreas.")
11
How is acute pancreatitis treated?
Treatment depends on the severity of the attack. If no kidney or lung complications occur, acute pancreatitis usually improves on its own. Treatment, in general, is designed to support vital bodily functions and prevent complications. A hospital stay will be necessary so that fluids can be replaced intravenously.

12
LANJUTAN... If pancreatic pseudocysts occur and are considered large enough to interfere with the pancreas's healing, your doctor may drain or surgically remove them. Unless the pancreatic duct or bile duct is blocked by gallstones, an acute attack usually lasts only a few days. In severe cases, a person may require intravenous feeding for 3 to 6 weeks while the pancreas slowly heals. This process is called total parenteral nutrition

13
LANJUTAN… Before leaving the hospital, a person will be advised not to drink alcohol and not to eat large meals. After all signs of acute pancreatitis are gone, the doctor will try to decide what caused it in order to prevent future attacks. Antibiotic

14
LANJUTAN… Secara klinis, penderita pankreatitis akut dapat beragam, dari yang mudah sembuh (self limiting) sampai yang dapat menimbulkan gejala-gejala berat dan kematian. Untuk itu, diperlukan identifikasi pasien yang mempunyai risiko untuk kematian berupa penilaian berat atau tidaknya penyakit yang diderita Saat ini banyak terdapat sistem penilaian, seperti: Kriteria Ranson Kriteria Glasgow (modifikasi) APACHE II
 sampai yang dapat menimbulkan gejala-gejala berat dan kematian. Untuk itu, diperlukan identifikasi pasien yang mempunyai risiko untuk kematian berupa penilaian berat atau tidaknya penyakit yang diderita. Saat ini banyak terdapat sistem penilaian, seperti: Kriteria Ranson. Kriteria Glasgow (modifikasi) APACHE II.")
15
Kriteria Ranson Menilai pada saat pasien masuk/dirawat di rumah sakit: umur > 55 tahun; lekosit dalam darah > /ml; gula darah > 200 mg/dL; LDH > 350 IU/L; dan AST > 200 IU/L. Setelah 48 jam perawatan: penurunan hematokrit > 10%; peningkatan BUN > 5 mg/dL; kalsium dalam darah < 8 mg/dL; arterial PaO2 < 60 mmHg; defisit basa > 4 mEq/L; dan defisit cairan > 6 liter

16
Kriteria Glasgow (modifikasi)
Setelah 48 jam perawatan: arterial PaO2 < 60 mmHg; albumin < 3,2 g/L; kalsium < 2 mmol/L; lekosit dalam darah > /ml; AST/ALT > 100 U/L; LDH > 600 U/L; gula darah > 10 mmol/L (tidak ada diabetes); dan urea > 16 mmol/L
; dan urea > 16 mmol/L.")
17
APACHE II Cara kerjanya adalah dengan menjumlahkan skor-skor dari skor fisiologis akut dengan skor umur dan skor kesehatan kronis. Tetapi, skor ini cukup rumit, diperlukan komputer untuk menentukan skor, dan memerlukan standarisasi untuk menentukan angka terendah serta tertinggi

18
KOMPLIKASI Komplikasi lokal, berupa:
Pengumpulan cairan yang akut. Hal ini paling sering terjadi, biasanya terjadi pada awal perjalanan penyakit, dan dapat membaik secara spontan; Nekrosis dari pankreas. Dapat terjadi lokal atau difus, bisa juga steril dan terinfeksi; Abses pankreas. Hal ini merupakan komplikasi lokal yang jarang terjadi; serta Yang lain, seperti pendarahan, trombosis vena splenikus, nekrosis, dan impaksi batu.

19
LANJUTAN… Komplikasi sistemik, berupa: Syok sirkulasi; Gagal napas;
Gagal ginjal akut; Sepsis; KID (Koagulopati Intravaskular Diseminata); Hiperglikemia; dan Hipokalsemia
; Hiperglikemia; dan. Hipokalsemia.")
20
Dx Keperawatan Gangguan pemenuhan keb nutrisi b/d asupan :
Defisiensi vit. ADEK (larut dlm lemak) Gangguan retina (-) vit A Tetani (-) vit D Metabolisme mineral (-) kalsium), (-) magnesium Nyeri b/d meregangnya kapsul pankreas Resiko terjadi gg sirkulasi b/d perdarahan Resiko terjadi gg keseimbangan gula darah
 Gangguan retina (-) vit A. Tetani (-) vit D. Metabolisme mineral (-) kalsium), (-) magnesium. Nyeri b/d meregangnya kapsul pankreas. Resiko terjadi gg sirkulasi b/d perdarahan. Resiko terjadi gg keseimbangan gula darah.")
21
Intervensi Dx 1 Tujuan = nutrisi terpenuhi dg adekuat Kriteria hasil =
Px menghabiskan makanan BB normal Tidak ada tanda malnutrisi, dehidrasi Intervensi Resusitasi cairan Kaji status nutrisi Monitor kadar glukose, albumin, elektrolit Bila mual puasakan, beri nutrisi parenteral/enteral Ukur BB Hindari makanan berlemak

22
Intervensi Dx 2 Tujuan = px mengatakan nyeri berkurang/hilang/dpt ditoleransi Kriteria hasil : Px tenang, tidak mengeluh nyeri Dapat beraktifitas normal Intervensi : Kaji nyeri (durasi, lokasi, intensitas/skala) Monitor ansietas px Saat serangan px bedrest Atur posisi px senyaman mungkin Ajarkan teknik relaksasi atau distraksi Kolaborasi dg dr u/ pemberian anti nyeri
 Monitor ansietas px. Saat serangan px bedrest. Atur posisi px senyaman mungkin. Ajarkan teknik relaksasi atau distraksi. Kolaborasi dg dr u/ pemberian anti nyeri.")
23
Intervensi Dx 3 Tujuan = tdk terjadi gg sirkulasi Kriteria hasil :
Tanda sirkulasi normal = tensi, nadi, suhu, GCS. Intervensi : Monitor tanda vital Evaluasi intake output Panta tanda perdarahan Ukur lingkar abdomen Bedrest Panta hasil laborat

24
Intervensi Dx 4 Tujuan = tdk terjadi peningkatan gula darah
Kriteria hasil: Gula darah puasa 80 – 120 mg/DL Gula darah acak 110 – 200 mg/DL Intervensi : Beri diet sesuai gula hasil darah, BBhindari aktifitas yg berlebihan Monitor tanda/efek peningkatan gula darah Beri penjelasan resiko peningkatan gula darah Jelaskan pantangan diet yg tepat

25
SEKIAN

Presentasi serupa


>")
>")















