Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
Dr. Edhie Djohan Utama, SpMK

2
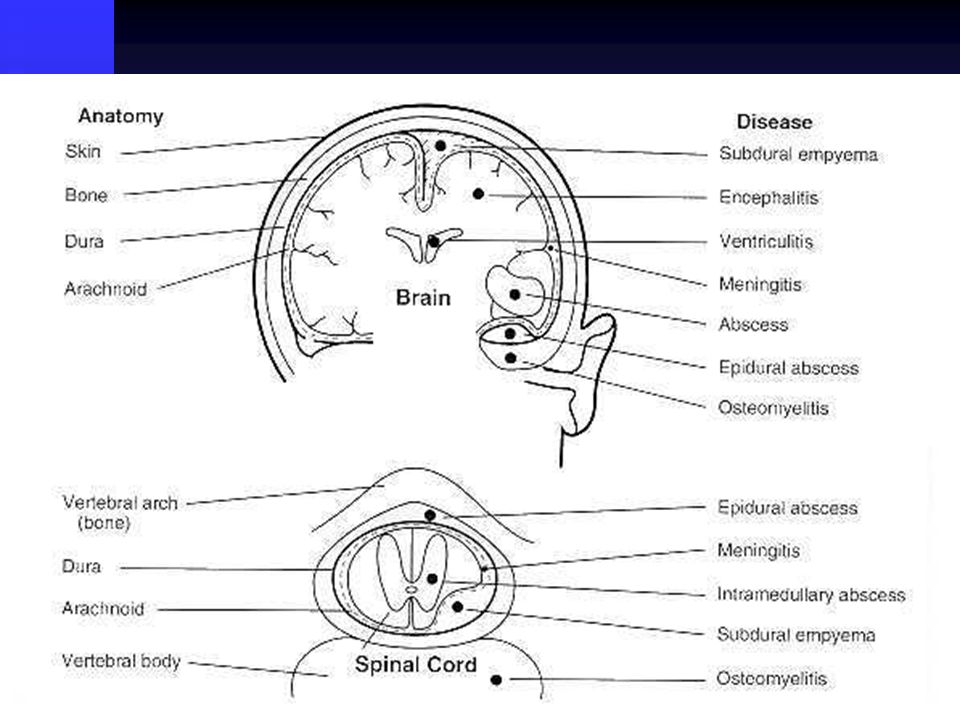
n Meningitis : c haracterized by high fever, headache, stiff neck (Infeksi Selaput Otak) n Encephalitis : c haracterized by changes in mental state, consciousness (kesadaran), behavior (tabiat) (Infeksi Jaringan Otak) n Brain Abscess : characterized by headache, focal signs and seizures indicate a brain abscess. There are also characteristic computed tomography (CT) and magnetic resonance image (MRI) findings. (Focal Purulent Infection of Brain Tissue)
 and magnetic resonance image (MRI) findings. (Focal Purulent Infection of Brain Tissue).")
3
General Concepts n The anatomy of the brain and meninges determines the special character of central nervous system (CNS) infections. n Epidural abscesses remain localized, whereas n Subdural abscesses spread over a hemisphere. n Subarachnoid space infections spread widely over the brain and spinal cord. n The blood-brain barrier formed by the tight junctions between cells of the cerebral capillaries, choroid plexus, and arachnoid largely prevents macromolecules from entering the brain parenchyma. n As a result, immunoglobulins and immune-competent cells are scarce in the brain except at foci of inflammation. n The space between cells in the brain parenchyma is too small to permit passage even of a virus. n However, tetanus toxin and some viruses travel through the CNS by axoplasmic flow.

6
INFEKSI PADA SISTEM SYARAF PUSAT BISA DISEBABKAN OLEH SEMUA AGENT YANG INFECTIOUS : = BAKTERI - PYOGENIK PYOGENIK = MYCOBACTERIA = FUNGI = SPIROCHAETA = VIRUS

7
INFEKSI SELAPUT OTAK (Meningitis) n I. MENINGITIS PURULENTA u MENINGOCOCCUS (40%) u PNEUMOCOCCUS u HAEMOPHILUS INFLUENZAE u STAPHYLOCOCCUS AUREUS u LISTERIA MONOCYTOGENES n II. MENIGITIS GRANULOMATOUS u MYCOBACTERIUM TUBERCULOSIS u COCCIDIODES IMMITIS (meningitis) u CRYPTOCOCCUS NEOFORMAN (meningitis) u HISTOPLASMA CAPSULATUM u TREPONEMA PALLIDUM u JAMUR JAMUR LAIN n III. ASEPTIC MENINGITIS u ENTEROVIRUS u POLIOMYELITIS u COXSACKIEVIRUS u ECHOVIRUS (Enteric Cytopathic Human Orphan) u RABIES u HERPES SIMPLEX u PARAMYXOVIRUS (Mumps virus) u LEPTOSPIRA u CLOSTRIDIUM TETANI
 u PNEUMOCOCCUS u HAEMOPHILUS INFLUENZAE u STAPHYLOCOCCUS AUREUS u LISTERIA MONOCYTOGENES n II. MENIGITIS GRANULOMATOUS u MYCOBACTERIUM TUBERCULOSIS u COCCIDIODES IMMITIS (meningitis) u CRYPTOCOCCUS NEOFORMAN (meningitis) u HISTOPLASMA CAPSULATUM u TREPONEMA PALLIDUM u JAMUR JAMUR LAIN n III. ASEPTIC MENINGITIS u ENTEROVIRUS u POLIOMYELITIS u COXSACKIEVIRUS u ECHOVIRUS (Enteric Cytopathic Human Orphan) u RABIES u HERPES SIMPLEX u PARAMYXOVIRUS (Mumps virus) u LEPTOSPIRA u CLOSTRIDIUM TETANI.")
8
TANDA TANDA KLINIS MENINGITIS n SAKIT KEPALA / HEADACHE n DEMAM / FEVER n GANGGUAN SENSORIS n KAKU DAN SAKIT KUDUK n TERDAPAT KELAINAN CSF (Cerebro spinal fluid)
")
9
I. MENINGITIS PURULENTA u MENINGOCOCCUS (40%) F NEISSERIA MENINGITIDIS, menyebabkan meningitis dan meningococcemia. (WATERHOUSE FREDERICHSEN SYNDROME = high fever, shock, purpura yg luas, intravascular coagulation dan adrenal insuffiency) u PNEUMOCOCCUS F DIPLOCOCCUS PNEUMONIAE / STREPTOCOCCUS PNEUMONIAE (bacterial meningitis) u HAEMOPHILUS INFLUENZAE u STAPHYLOCOCCUS AUREUS F (Toksin mediated menimbulkan shock syndrome) u LISTERIA MONOCYTOGENES (Acute meningitis pada newborn) u 80% meningitis disebabkan oleh Meningococcus dan Pneumococcus ( Levinson & Jawetz )
 F NEISSERIA MENINGITIDIS, menyebabkan meningitis dan meningococcemia. (WATERHOUSE FREDERICHSEN SYNDROME = high fever, shock, purpura yg luas, intravascular coagulation dan adrenal insuffiency) u PNEUMOCOCCUS F DIPLOCOCCUS PNEUMONIAE / STREPTOCOCCUS PNEUMONIAE (bacterial meningitis) u HAEMOPHILUS INFLUENZAE u STAPHYLOCOCCUS AUREUS F (Toksin mediated menimbulkan shock syndrome) u LISTERIA MONOCYTOGENES (Acute meningitis pada newborn) u 80% meningitis disebabkan oleh Meningococcus dan Pneumococcus ( Levinson & Jawetz ).")
10
Bacterial Diseases of the Nervous System 1. Meningitis can be caused by viruses, bacteria, fungi, and protozoa. 2. The three major causes of bacterial meningitis are Haemophilus influenzae, Streptococcus pneumoniae, and Neisseria meningitidis. These three etiological agents cause more than 70% of the meningitis cases and 70% of the related deaths. 3. Nearly 50 species of opportunistic bacteria can cause meningitis.

11
a. Neisseria Meningitidis 1. N. meningitidis (meningococcus) causes meningococcal meningitis. meningococcal meningitis. 2. This bacterium is found in the throats of healthy carriers (reservoir). The bacteria healthy carriers (reservoir). The bacteria probably gain access to the meningens through probably gain access to the meningens through the bloodstream. the bloodstream. 3. The bacteria may be found in leukocytes in the CSF.
. The bacteria healthy carriers (reservoir). The bacteria probably gain access to the meningens through probably gain access to the meningens through the bloodstream. the bloodstream. 3. The bacteria may be found in leukocytes in the CSF..")
12
4. Symptoms are due to hyperproduction of endotoxin. endotoxin. 5. The disease occurs most often in young children, but can also cause outbreaks among persons living in close can also cause outbreaks among persons living in close contact (military, college dormitories, institutional contact (military, college dormitories, institutional settings). settings). 6. Military recruits are vaccinated with purified capsular polysaccharide to prevent epidemics in training camps. polysaccharide to prevent epidemics in training camps. Unfortunately, like other polysaccharide vaccines, it is Unfortunately, like other polysaccharide vaccines, it is not effective in very young children. not effective in very young children.
. settings). 6. Military recruits are vaccinated with purified capsular polysaccharide to prevent epidemics in training camps. polysaccharide to prevent epidemics in training camps. Unfortunately, like other polysaccharide vaccines, it is Unfortunately, like other polysaccharide vaccines, it is not effective in very young children. not effective in very young children..")
13
Neisseria meningitidis ( Meningococcus ) n Spread in respiratory droplets n Inactivate IgA using IgA protease n Colonize the nasopharynx using fimbriae sore throat n Endocytized bloodstream (capsule to avoid phagocytosis) n Endotoxin: u 1. affects blood vessel permeability cross BBB (attach to dura mater w/ fimbriae) u 2. drop in blood pressure shock u 3. clotting of blood hemorrhage (rash) and DIC n Mortality in untreated - 85% n Optimal - 1% n Crowding - military, dorms, day-care
 u 2. drop in blood pressure shock u 3. clotting of blood hemorrhage (rash) and DIC n Mortality in untreated - 85% n Optimal - 1% n Crowding - military, dorms, day-care.")
14
b. Haemophilus influenzae 1. H. influenzae is part of the normal throat microbiota. 2. H. influenzae requires blood factors (X and V factors) for growth; There are six types of H. influenzae based on polysaccharide capsule differences. H. influenzae type b (HIB) is the most common cause of meningitis in children under 4 years old. 3. A conjugated vaccine directed against the capsular polysaccharide antigen is available. Use of the HIB vaccine has decreased the incidence of meningitis in children under five years of age by 99% in the U.S.
 for growth; There are six types of H. influenzae based on polysaccharide capsule differences. H. influenzae type b (HIB) is the most common cause of meningitis in children under 4 years old. 3. A conjugated vaccine directed against the capsular polysaccharide antigen is available. Use of the HIB vaccine has decreased the incidence of meningitis in children under five years of age by 99% in the U.S..")
15
Haemophilus influenzae type B n Inactivate IgA using IgA protease n Colonize the nasopharynx n Penetrate submucosa (invasive) bloodstream (capsule to avoid phagocytosis) n Endotoxin: n Inflammation, DIC n Mortality 6% n Mental retardation
 bloodstream (capsule to avoid phagocytosis) n Endotoxin: n Inflammation, DIC n Mortality 6% n Mental retardation")
16
c. Streptococcus pneumoniae ( Pneumococcal Meningitis ) 1. S. pneumoniae (pneumococcus) is commonly found in the nasopharynx. 2. Hospitalized patients and young children are most susceptible to S. pneumoniae meningitis. It is rare (3000 cases annually in U.S.) but has a high mortality rate. 3. The vaccine for pneumococcal pneumonia may provide some protection against pneumococcal meningitis.
 is commonly found in the nasopharynx. 2. Hospitalized patients and young children are most susceptible to S. pneumoniae meningitis. It is rare (3000 cases annually in U.S.) but has a high mortality rate. 3. The vaccine for pneumococcal pneumonia may provide some protection against pneumococcal meningitis..")
17
Streptococcus pneumoniae (Pneumococcus) n spreads from sinuses or middle ear brain OR n pneumonia in lungs bloodstream brain
 n spreads from sinuses or middle ear brain OR n pneumonia in lungs bloodstream brain")
18
d. Listeriosis 1. Listeria monocytogenes causes meningitis in : newborns, the immunosuppressed, pregnant women, and cancer patients. 2. Acquired by ingestion of contaminated food, it may be asymptomatic in healthy adults. 3. The organisms are capable of growing at refrigerator temperatures. 4. L. monocytogenes can cross the placenta and cause spontaneous abortion and stillbirth.

19
Diagnosis and Treatment of the Most Common Types of Bacterial Meningitis 1. Cephalosporins may be administered initially before identification of the pathogen. 2. Diagnosis is based on gram stain and serological tests of the bacteria in CSF. 3. Cultures are usually made on blood agar and incubated in an atmosphere containing reduced oxygen levels.

20
II. MENIGITIS GRANULOMATOUS n MYCOBACTERIUM TUBERCULOSIS (Tuberculosis meningitis) n COCCIDIODES IMMITIS (meningitis) n CRYPTOCOCCUS NEOFORMAN (meningitis) n HISTOPLASMA CAPSULATUM n TREPONEMA PALLIDUM (Syphilis stadium ke-3, timbul tabes dorsalis dan meningo-vascular syphilis) n JAMUR JAMUR LAIN
 n COCCIDIODES IMMITIS (meningitis) n CRYPTOCOCCUS NEOFORMAN (meningitis) n HISTOPLASMA CAPSULATUM n TREPONEMA PALLIDUM (Syphilis stadium ke-3, timbul tabes dorsalis dan meningo-vascular syphilis) n JAMUR JAMUR LAIN.")
21
Tuberculous meningitismeningitis n Infection may begins in the lungs and may spread to the meninges by a variety of routes. n Blood-borne spread certainly occurs and 25% of patients with miliary TB have TB meningitis, presumably by crossing the blood-brain barrier[1]; but a proportion of patients may get TB meningitis from rupture of a cortical focus in the brain (a so-called Rich focus); an even smaller proportion get it from rupture of a bony focus in the spine. It is rare and unusual for TB of the spine to cause TB of the central nervous system, but isolated cases have been described. miliary TBblood-brain barrier[1]Rich focuscentral nervous systemmiliary TBblood-brain barrier[1]Rich focuscentral nervous system
; an even smaller proportion get it from rupture of a bony focus in the spine. It is rare and unusual for TB of the spine to cause TB of the central nervous system, but isolated cases have been described. miliary TBblood-brain barrier[1]Rich focuscentral nervous systemmiliary TBblood-brain barrier[1]Rich focuscentral nervous system.")
22
Diagnosis n Diagnosis of TB meningitis is made by analysing CSF collected by lumbar puncture. CSFlumbar punctureCSFlumbar puncture n When collecting CSF for suspected TB meningitis, a minimum of 1ml of fluid should be taken (preferably 5 to 10ml). ml n The CSF usually has a high protein, low glucose and a raised number of lymphocytes. n Acid-fast bacilli are sometimes seen on a CSF smear, but more commonly, M. tuberculosis is grown in culture. Acid-fast bacilli Acid-fast bacilli n A spiderweb clot in the collected CSF is characteristic of TB meningitis, but is a rare finding. n More than half of cases of TB meningitis cannot be confirmed microbiologically, and these patients are treated on the basis of clinical suspicion only. n The culture of TB from CSF takes a minimum of two weeks, and therefore the majority of patients with TB meningitis are started on treatment before the diagnosis is confirmed.
. ml n The CSF usually has a high protein, low glucose and a raised number of lymphocytes. n Acid-fast bacilli are sometimes seen on a CSF smear, but more commonly, M. tuberculosis is grown in culture. Acid-fast bacilli Acid-fast bacilli n A spiderweb clot in the collected CSF is characteristic of TB meningitis, but is a rare finding. n More than half of cases of TB meningitis cannot be confirmed microbiologically, and these patients are treated on the basis of clinical suspicion only. n The culture of TB from CSF takes a minimum of two weeks, and therefore the majority of patients with TB meningitis are started on treatment before the diagnosis is confirmed..")
23
Treatment n The treatment of TB meningitis is isoniazid, rifampicin, pyrazinamide and ethambutol for two months, followed by isoniazid and rifampicin alone for a further ten months. isoniazidrifampicin pyrazinamideethambutolisoniazidrifampicin pyrazinamideethambutol n Steroids are always used in the first six weeks of treatment (and sometimes for longer). n A few patients may require immunomodulatory agents such as thalidomide. immunomodulatory thalidomideimmunomodulatory thalidomide n Treatment must be started as soon as there is a reasonable suspicion of the diagnosis. n Treatment must not be delayed while waiting for confirmation of the diagnosis. n Hydrocephalus occurs as a complication in about a third of patients with TB meningitis and will require a ventricular shunt. Hydrocephalus
. n A few patients may require immunomodulatory agents such as thalidomide. immunomodulatory thalidomideimmunomodulatory thalidomide n Treatment must be started as soon as there is a reasonable suspicion of the diagnosis. n Treatment must not be delayed while waiting for confirmation of the diagnosis. n Hydrocephalus occurs as a complication in about a third of patients with TB meningitis and will require a ventricular shunt. Hydrocephalus.")
24
Fungal meningitis n Meningitis caused by a fungal infection. Meningitis is an inflammation of the lining around the brain and spinal cord. brain n Fungal meningitis is relatively rare and results when airborne yeast cells are inhaled. n The condition mostly occurs in people with a compromised immune system such as AIDS sufferers. immune systemimmune system n COCCIDIODES IMMITIS (meningitis) n CRYPTOCOCCUS NEOFORMAN (meningitis) n HISTOPLASMA CAPSULATUM
 n CRYPTOCOCCUS NEOFORMAN (meningitis) n HISTOPLASMA CAPSULATUM.")
25
Symptoms of Fungal meningitis n Headache Headache n Blurred vision (diplopia and unequal, sluggish pupils ) Blurred vision Blurred vision n Confusion Confusion n Tiredness Tiredness n Stiff neck Stiff neck Stiff neck n Positive Kernig's sign, nuchal rigidity, irritability or restlessness
 Blurred vision Blurred vision n Confusion Confusion n Tiredness Tiredness n Stiff neck Stiff neck Stiff neck n Positive Kernig s sign, nuchal rigidity, irritability or restlessness")
26
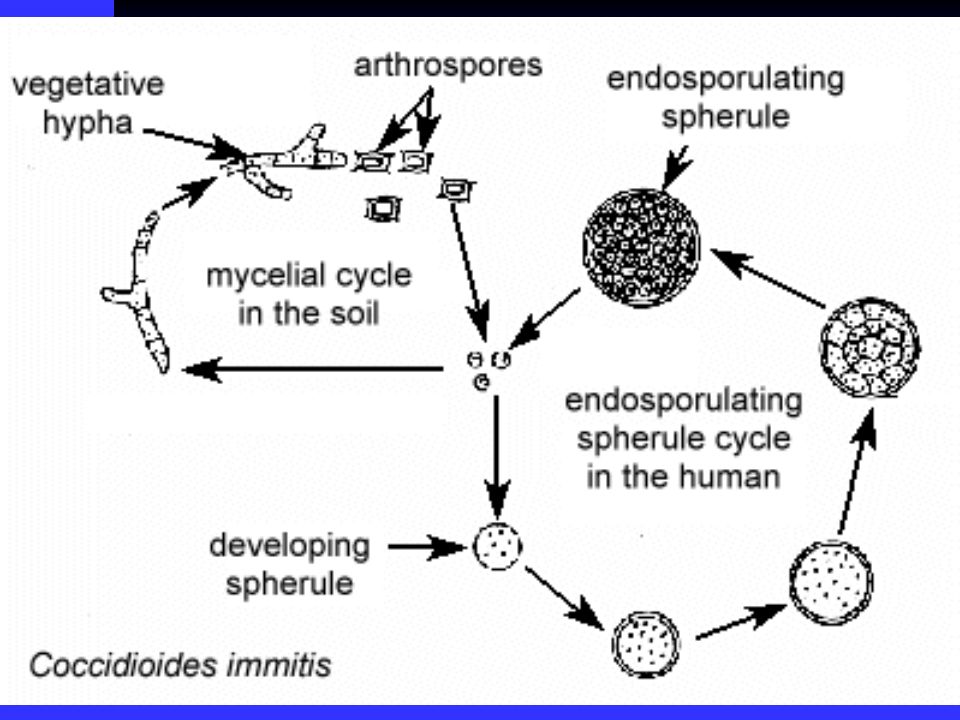
Coccidioides Immitis n n Coccidioides immitis adalah suatu jamur biasa terdapat di tanah, sehingga disebut jamur tanah. n n Bersifat endemik dan dapat menyebabkan koksidioidomikosis. n n Infeksi biasanya dapat sembuh sendiri tetapi juga dapat mematikan. n n Juga dikenal sebagai jamur dimorfik karena jamur ini mempunyai daya adaptasi morfologik yang unik terhadap pertumbuhan dalam jaringan atau pertumbuhan pada 37°C. n n Coccidioides immitis bentuk seperti bola (=sferul) yang garis tengahnya 15 - 60μm, dengan dinding tebal berbias ganda. n n Hifa dari jamur ini juga mudah pecah dan mengeluarkan spora.
 yang garis tengahnya μm, dengan dinding tebal berbias ganda. n n Hifa dari jamur ini juga mudah pecah dan mengeluarkan spora..")
27
Coccidioides Immitis n n Infeksi oleh jamur ini biasanya meliputi influenza, demam, lesu, batuk, dan adanya rasa sakit di seluruh tubuh. n n Gejala – gejala inilah yang biasanya disebut “Valley fever” dan biasanya gejala ini dapat sembuh sendiri yang dikenal dengan infeksi primer dan hanya dibutuhkan pengobatan suportif atau dapat juga kronik. n n Obat yang dipakai antara lain berupa Amphotericin B, Ketokonazol, Mikonazol. n n Penyakit ini tidak dapat ditularkan dari orang ke orang.

28
Patogenesis dan Gambaran Klinik n n Infeksi didapat melalui inhalasi artrospora yang terdapat di udara. n n Infeksi dapat bersifat asimptomatis dan mungkin hanya terbukti dengan pembentukan antibody presipitasi dan tes kulit positif dalam 2-3 minggu. n n Disamping itu penyakit yang menyerupai influenza, yang disertai demam, lesu, batuk, dan rasa sakit di seluruh tubuh juga dapat terjadi. n n Kurang dari 1% orang yang terinfeksi C. immitis, penyakitnya berkembang menjadi bentuk yang menyebar dan sangat fatal. n n Hal ini dapat sangat menyolok terlihat pada wanita yang hamil. n n Ini disebabkan karena kadar estradiol dan progesterone yang meningkat pada wanita hamil dapat menambah pertumbuhan C. immitis.

29
Patogenesis dan Gambaran Klinik n n Sebagian besar orang dapat dianggap kebal terhadap reinfeksi, setelah tes – tes kulitnya menjadi positif. n n Akan tetapi, bila individu seperti ini kekebalannya ditekan dengan obat atau penyakit, penyebarannya dapat terjadi beberapa tahun setelah infeksi primernya. n n Koksidioidomikosis yang menyebar dapat disamakan juga dengan tuberkolosis, dengan lesi pada banyak organ tubuh, tulang dan susunan saraf pusat.

32
Diagnosis n n Diagnosis koksidioidomikosis didasarkan atas: n n 1. Pemeriksaan langsung : kerokan kelainan kulit, dahak atau bilasan bronkus. Pewarnaan khusus oleh jamur pada jaringan (terlihat bulatan – bulatan kecil berisi endospora: tidak terlihat sel – sel ragi bertunas) n n 2. Biakan dari dahak, bilasan bronkus, biopsy atau kerokan kulit (bahan-bahan ini sangat menular) n n 3. Serologi diagnostic yaitu: - Tes presipitin tabung untuk mengukur titer IgM - Reaksi peningkatan komplemen untuk mengukur titer IgG - Aglutinasi lateks dan uji imunodifusi sebagai alat penyaring pada daerah endemic ternyata dapat mendeteksi 93% kasus n n 4. Tes kulit pada stadium awal infeksi
 n n 2. Biakan dari dahak, bilasan bronkus, biopsy atau kerokan kulit (bahan-bahan ini sangat menular) n n 3. Serologi diagnostic yaitu: - Tes presipitin tabung untuk mengukur titer IgM - Reaksi peningkatan komplemen untuk mengukur titer IgG - Aglutinasi lateks dan uji imunodifusi sebagai alat penyaring pada daerah endemic ternyata dapat mendeteksi 93% kasus n n 4. Tes kulit pada stadium awal infeksi.")
33
Pencegahan & Pengobatan Pencegahan Mengurangi debu, mengaspal jalan – jalan dan lapangan terbang dimana banyak debu – debu berterbangan, menanam pepohonan, dan menggunakan semprotan minyak. Pengobatan n n Pada koksidioidomikosis disseminate, Amfoterisin B diberikan secara intravena (0,4 – 0,8 mg/kg/hari). Amfoterisin B (AMB) merupakan suatu anti jamur polien yang diberikan secara intravena dan meskipun dapat menyebabkan nefrotoksin, tetapi merupakan obat pilihan pada infeksi jamur yang gawat. n n Pemberian Amfoterisin B(AMB) secara terus menerus selama beberapa bulan dapat menimbulkan remisi. n n Mikonazol dan ketokonazol sistemik juga cukup efektif dalam pengobatan koksidioidomikosis paru – paru menahun tetapi efeknya sangat terbatas pada penyakit yang menyebar. Ketokonazol adalah obat imidazol per os yang berguna untuk infeksi jamur sistemik yang tidak gawat. Sedangkan Mikonazol adalah obat imidazol lain yang perlu diberikan secara intravena dan lebih toksis daripada ketokonazol. Pada keadaan yang disertai kelainan meningeal, dosis ketonazol 800mg/hari diberikan melalui mulut dengan pemberian secara intravena ketokonazol telah memberikan efek yang memuaskan. n n Pada meningitis oleh koksidioides, amfoterisin B juga diberikan intratekal, tetapi hasilnya dalam jangka panjang seringkali kurang memuaskan.
. Amfoterisin B (AMB) merupakan suatu anti jamur polien yang diberikan secara intravena dan meskipun dapat menyebabkan nefrotoksin, tetapi merupakan obat pilihan pada infeksi jamur yang gawat. n n Pemberian Amfoterisin B(AMB) secara terus menerus selama beberapa bulan dapat menimbulkan remisi. n n Mikonazol dan ketokonazol sistemik juga cukup efektif dalam pengobatan koksidioidomikosis paru – paru menahun tetapi efeknya sangat terbatas pada penyakit yang menyebar. Ketokonazol adalah obat imidazol per os yang berguna untuk infeksi jamur sistemik yang tidak gawat. Sedangkan Mikonazol adalah obat imidazol lain yang perlu diberikan secara intravena dan lebih toksis daripada ketokonazol. Pada keadaan yang disertai kelainan meningeal, dosis ketonazol 800mg/hari diberikan melalui mulut dengan pemberian secara intravena ketokonazol telah memberikan efek yang memuaskan. n n Pada meningitis oleh koksidioides, amfoterisin B juga diberikan intratekal, tetapi hasilnya dalam jangka panjang seringkali kurang memuaskan..")
34
Cryptococcal meningitis n Cryptococcal meningitis is a life-threatening infection that can occur if there has been exposure to a fungus called Cryptococcus neoformans. n This fungus is found in the environment worldwide, particularly in soil contaminated with bird droppings. n This fungus enters the body most commonly through the lungs. Infection does not usually appear until a person's CD4 counts have dropped below 100. n Cryptococcal meningitis can not be passed from one person to another. n This fungus most commonly affects the brain, causing the condition called meningitis.

35
Cryptococcal meningitis n Meningitis is an infection and swelling of the lining of the brain and spinal cord. n Cryptococcus can also cause infections of the lungs, skin and prostate gland. n Cryptococcal meningitis may be very slow in developing, so at first, very vague symptoms may appear: mild headache, fever, nausea.

36
Special tests to confirm Cyptococcal meningitis: n Special tests are needed : n Lumbar puncture (spinal tap): taking fluid from your spinal column through a needle in your back. This fluid in then sent for special tests. Blood tests: to check whether you have been exposed to the fungus.

37
TREATMENT n Medications are usually given intravenously (directly into the vein). Amphotericin B and fluconazole (Diflucan) are the most common drugs used to treat the infection. n Once the infection has been treated, it is recommended that the person remain on one of the these drugs for the rest of their lives to prevent the infection from returning again.
 are the most common drugs used to treat the infection. n Once the infection has been treated, it is recommended that the person remain on one of the these drugs for the rest of their lives to prevent the infection from returning again..")
38
Meningitis due to Histoplasma capsulatum n Meningitis due to Histoplasma capsulatum and Mycobacterium tuberculosis in a returned traveler with acquired immunodeficiency syndrome

39
Spirochaeta n Syphilis can cause varied neurologic diseases over the lifetime of the untreated patient. n During secondary syphilis, 6 weeks to 3 months after primary infection, a benign mild meningitis may accompany the primary CNS invasion that occurs in approximately 25 percent of untreated patients. n Later complications include acute meningovascular inflammatory disease leading to stroke (meningovascular syphilis) 3 to 5 years after the primary infection, progressive dementia (general paresis) 8 to 10 years later, or a chronic arachnoiditis involving primarily the posterior roots of the spinal cord (tabes dorsalis) 10 to 20 years after infection. n This development of vasculitis, parenchymal involvement and chronic arachnoiditis parallel the complications that occur over weeks during untreated bacterial meningitis.
 3 to 5 years after the primary infection, progressive dementia (general paresis) 8 to 10 years later, or a chronic arachnoiditis involving primarily the posterior roots of the spinal cord (tabes dorsalis) 10 to 20 years after infection. n This development of vasculitis, parenchymal involvement and chronic arachnoiditis parallel the complications that occur over weeks during untreated bacterial meningitis..")
40
III. ASEPTIC MENINGITIS n ENTEROVIRUS u POLIOMYELITIS u COXSACKIEVIRUS u ECHOVIRUS (Enteric Cytopathic Human Orphan) n RABIES n HERPES SIMPLEX n PARAMYXOVIRUS (Mumps virus) n LEPTOSPIRA n CLOSTRIDIUM TETANI
 n RABIES n HERPES SIMPLEX n PARAMYXOVIRUS (Mumps virus) n LEPTOSPIRA n CLOSTRIDIUM TETANI.")
41
Viral meningitis = aseptic meningitis n Fairly common (40%) n Self-limiting, non-fatal n CSF is clear n Many different viruses n 1. Enteroviruses - 40% n 2. Mumps virus - 15% n 3. Other

42
Fungal meningitis n Chronic presentation u 1. Coccidioides immitis u 2. Cryptococcus neoformans - AIDS

43
VIRUS PENYEBAB ENCEPHALITIS n TOGAVIRIDAE (Genus Alphavirus) Chikungunya Eastern equine encephalitis (EEE), transmisi nyamuk Culiseta Western Equine Encephalitis (WEE), transmisi oleh nyamuk Culex St.Louis Encephalitis (SLE), trasmisi oleh nyamuk Culex California Encephalitis (CE), transmisi oleh nyamuk Aedes triseriatus n FLAVIVIRUS u Flavivirus berukuran kecil (40 nm), berbeda dalam morfogenesis dan berbeda dalam struktur genomnya dari Togavirus u Yang teriinfeksi sering menyebabkan encephalitis, dasarnya adalah neurotrofik khususnya pd binatang pengerat n VIRUS RABIES u Progressive encephalitis terjadi jika virus mencapai / menyebar ke CNS, gejala klinis hyrdophobia
 Chikungunya Eastern equine encephalitis (EEE), transmisi nyamuk Culiseta Western Equine Encephalitis (WEE), transmisi oleh nyamuk Culex St.Louis Encephalitis (SLE), trasmisi oleh nyamuk Culex California Encephalitis (CE), transmisi oleh nyamuk Aedes triseriatus n FLAVIVIRUS u Flavivirus berukuran kecil (40 nm), berbeda dalam morfogenesis dan berbeda dalam struktur genomnya dari Togavirus u Yang teriinfeksi sering menyebabkan encephalitis, dasarnya adalah neurotrofik khususnya pd binatang pengerat n VIRUS RABIES u Progressive encephalitis terjadi jika virus mencapai / menyebar ke CNS, gejala klinis hyrdophobia")
44
Infections of Neural Tissue Poliovirus ( poliomyelitis ) n fecal/oral route of transmission n spread by contaminated water n 90% asymptomatic infections n 10% flu-like illness n 0.01% paralytic poliomyelitis n Replicates inside epithelial cells of nose, throat, intestine lymphatics bloodstream n If enters CNS infected cells die paralytic polio n Historical rate of paralytic polio US - 21,000/yr u Peak year US - 1958 u Last case wild virus in US - 1979 u Western hemisphere declared free - 1994 u Discontinuation of oral polio vaccine - 1999 u Worldwide eradication
 n fecal/oral route of transmission n spread by contaminated water n 90% asymptomatic infections n 10% flu-like illness n 0.01% paralytic poliomyelitis n Replicates inside epithelial cells of nose, throat, intestine lymphatics bloodstream n If enters CNS infected cells die paralytic polio n Historical rate of paralytic polio US - 21,000/yr u Peak year US u Last case wild virus in US u Western hemisphere declared free u Discontinuation of oral polio vaccine u Worldwide eradication")
45
Poliomyelitis 1. The symptoms of poliomyelitis are usually headache, sore throat, fever, stiffness of the back and neck, and occasionally paralysis (less than 1% of cases). 2. Poliovirus is found only in humans and is transmitted by the ingestion of water contaminated with feces. 3. Poliovirus first invades lymph nodes of the neck and small intestine. Viremia (free viruses in the blood) and spinal cord involvement may follow. 4. Diagnosis is based on isolation of the virus from feces and throat secretions.
. 2. Poliovirus is found only in humans and is transmitted by the ingestion of water contaminated with feces. 3. Poliovirus first invades lymph nodes of the neck and small intestine. Viremia (free viruses in the blood) and spinal cord involvement may follow. 4. Diagnosis is based on isolation of the virus from feces and throat secretions..")
46
TRANSMISI VIRUS POLIO n POLIOVIRUS KELUAR BERSAMA FECES, DISEBARKAN MELALUI MAKANAN DAN MINUMAN YANG TERKONTAMINASI. n BISA MELALUI BERSIN DAN BATUK KARENA DIJUMPAI PADA MUCOSA HIDUNG DAN MULUT

47
PATHOGENESIS POLIOVIRUS n MULTIPLIKASI PADA MEMBRAN MUCOSA SALURAN MAKANAN DAN JUGA PADA SEL SEL MUCOSA PHARYNX n KEMUDIAN MENEMBUS DAN MASUK KE KELENJAR LYMPHE TERDEKAT n MASUK KEDALAM DARAH SUSUNAN SYARAF PUSAT GRAY MATTER SUM-SUM TULANG BELAKANG MERUSAK MOTOR NEURON KELUMPUHAN OTOT

48
KLINIS POLIOMYELITIS n ABORTIVE n NONPARALYTIC POLIOMYELITIS (ASEPTIC MENINGITIS) n PARALYTIC POLIOMYELITIS n PROGRESSIVE POST POLIOMYELITIS MUSCLE ATROPHY
 n PARALYTIC POLIOMYELITIS n PROGRESSIVE POST POLIOMYELITIS MUSCLE ATROPHY")
49
VACCINE POLIOMYELITIS n SALK VACCINE : parenteral u Menghasilkan humoral AB u Diberikan 4kali dalam 1-2 tahun u Efektivitas 70-90% n SABIN VACCINE : per oral u Trivalent vaccine u Idealnya diberikan pada usia 6 bulan berturut turut 3 kali jarak 6-8 minggu u Efektivitas 100% u Menghasilkan IgM, IgG dan secretory IgA dalam saluran pencernaan

50
Poliovaccine 5. The Salk vaccine (an inactivated polio vaccine, IPV) involves injection of formalin- inactivated viruses and boosters every few years. 6. The Sabin vaccine (oral polio vaccine, OPV) contains three attenuated live strains of poliovirus and is administered orally. Polio will be eliminated through vaccination.
 involves injection of formalin- inactivated viruses and boosters every few years. 6. The Sabin vaccine (oral polio vaccine, OPV) contains three attenuated live strains of poliovirus and is administered orally. Polio will be eliminated through vaccination..")
51
PENGOBATAN DAN PENCEGAHAN INFEKSI POLIOVIRUS n PENGOBATAN : u Diberikan obat penghilang rasa sakit u Obat kejang kejang otot u Mengatur respirasi u Hydrasi n PENCEGAHAN : u Salk vaccine (killed vaccine) Suntikan u Sabin vaccine : Live attenuated strain per oral
 Suntikan u Sabin vaccine : Live attenuated strain per oral")
52
Infections of Neural Tissue Viral - RABIES n Rabies - Rhabodovirus n Bite, Multiplies at site n Travels to local nerves n Peripheral nerves spinal cord brain n Long incubation (tergantung lokasi gigitan) n Prodromal phase - flulike symptoms, tingling, burning, depression n Excitation phase - muscle function, speech, vision, anxiety, hydrophobia n Paralytic phase - muscles weaken, consciousness fades, death n Mortality - 100% with best treatment n Post exposure prophylaxis (PEP) - has never failed in US
 n Prodromal phase - flulike symptoms, tingling, burning, depression n Excitation phase - muscle function, speech, vision, anxiety, hydrophobia n Paralytic phase - muscles weaken, consciousness fades, death n Mortality - 100% with best treatment n Post exposure prophylaxis (PEP) - has never failed in US")
53
n Rabies, is usually acquired through the bite of a rabid warm-blooded animal. n This virus spreads by axonal transport from the inoculated skin or muscle to the corresponding dorsal root ganglion or anterior horn cells and then to populations of neurons throughout the CNS. n The early involvement of neurons of the limbic system cause the typical behavioral changes of clinical rabies.

54
Rabies 1. Rabies virus (rhabdovirus) causes an acute, usually fatal, encephalitis called rabies. 2. Rabies may be contracted through the bite of a rabid animal, by inhalation of aerosols, or invasion through minute skin abrasions. The virus multiplies in skeletal muscle and connective tissue. 3. Encephalitis occurs when the virus moves along peripheral nerves to the CNS. 4. Symptoms of rabies include spasms of mouth and throat muscles, followed by extensive brain and spinal cord damage and death.

55
Rabies 5. Laboratory diagnosis may be made by direct immunofluorescent tests of saliva, serum, and CSF or brain smears. 6. Reservoirs for rabies in the United States include skunks, bats, foxes, and raccoons. Domestic cattle, dogs, and cats may get rabies. Rodents and rabbits seldom get rabies. 7. Current postexposure treatment includes administration of human rabies immune globulin (RIGH) along with multiple intramuscular injections of vaccine. 8. Preexposure treatment consists of vaccination.
 along with multiple intramuscular injections of vaccine. 8. Preexposure treatment consists of vaccination..")
56
Botulism 1. Botulism is caused by an exotoxin produced by Clostridium botulinum growing in foods. 2. Serological types of botulinum toxin vary in virulence, with type A being the most virulent. 3. The toxin is a neurotoxin that inhibits the transmission of nerve impulses. 4. Blurred vision occurs in 1-2 days; progressive flaccid paralysis follows for 1-10 days, resulting in respiratory and cardiac failure. 5. C. botulinum will not grow in acidic foods or in an aerobic environment.

57
6. Endospores are killed by proper canning. The addition of nitrites to foods inhibits outgrowth after endospore germination. 7. The toxin is heat labile and is destroyed by boiling (100°C) for 5 minutes. 8. Infant botulism results from the growth of Clostri- dium botulinum in an infant's intestines and has been associated with the ingestion of honey products. 9. Wound botulism occurs when C. botulinum grows in anaerobic wounds. 10. For diagnosis, mice protected with antitoxin are inoculated with toxin from the patient or foods.
 for 5 minutes. 8. Infant botulism results from the growth of Clostri- dium botulinum in an infant s intestines and has been associated with the ingestion of honey products. 9. Wound botulism occurs when C. botulinum grows in anaerobic wounds. 10. For diagnosis, mice protected with antitoxin are inoculated with toxin from the patient or foods..")
58
Arboviral Encephalitis 1. Symptoms of encephalitis are chills, headache, fever, and eventually coma. 2. Many types of arboviruses transmitted by mosquitoes cause encephalitis. 3. The incidence of arboviral encephalitis increases in the summer months when mosquitoes are most numerous.

59
Arboviral Encephalitis 5. Diagnosis is based on serological tests. 6. Control of the vector is the most effective way to control encephalitis. 4. Horses are frequently infected by EEE (eastern equine encephalitis) and WEE (western equine encephalitis) viruses.
 and WEE (western equine encephalitis) viruses..")
60
Brain Abscess n An abscess is a focus of purulent infection and is usually due to bacteria. n Brain abscesses develop from either a contiguous focus of infection (such as the ears, the sinuses, or the teeth) or hematogenous spread from a distant focus (such as the lungs or heart, particularly with chronic purulent pulmonary disease, subacute bacterial endocarditis, or cyanotic congenital heart disease). n In many cases the source is undetected. n Many brain abscesses have a mixed flora of aerobic and anaerobic bacteria. n Approximately 60 to 70 percent contain streptococci; and Staphylococcus aureus, enterobacteria and Bacteroides are frequently present. n Fungi cause fewer than 10 percent of brain abscesses
 or hematogenous spread from a distant focus (such as the lungs or heart, particularly with chronic purulent pulmonary disease, subacute bacterial endocarditis, or cyanotic congenital heart disease). n In many cases the source is undetected. n Many brain abscesses have a mixed flora of aerobic and anaerobic bacteria. n Approximately 60 to 70 percent contain streptococci; and Staphylococcus aureus, enterobacteria and Bacteroides are frequently present. n Fungi cause fewer than 10 percent of brain abscesses.")
61
CLINICAL MANIFESTATION BRAIN ABSCESS n The primary clinical manifestations of abscess are headache, focal signs, and seizures. n The headache may not be severe, however, and the development of signs may be insidious. n There may be no fever. If focal signs are present computed tomography (CT) or magnetic resonance imaging (MRI) is performed rather than CSF examination. n An abscess is identified by a hypodense area representing pus surrounded by an enhancing area representing the neovascularization and edema around the fibrous abscess wall. n The CSF is usually sterile, and bacteriologic diagnosis can only be obtained by culturing an aspirate of the abscess cavity.
 or magnetic resonance imaging (MRI) is performed rather than CSF examination. n An abscess is identified by a hypodense area representing pus surrounded by an enhancing area representing the neovascularization and edema around the fibrous abscess wall. n The CSF is usually sterile, and bacteriologic diagnosis can only be obtained by culturing an aspirate of the abscess cavity..")
62
Infections of Neural Tissue Bacterial n Tetanus - Clostridium tetani - tetanospasmin (mimics strychnine poisoning) n Botulism - Clostridium botulinum n Genes for toxin are carried on a bacteriophage n Toxin prevents release of acetylcholine n Produces a limp, flaccid, paralysis n Eyes blurry, double vision n Throat slurring speech, difficulty swallowing n Difficulty breathing n Cardiac problems
 n Botulism - Clostridium botulinum n Genes for toxin are carried on a bacteriophage n Toxin prevents release of acetylcholine n Produces a limp, flaccid, paralysis n Eyes blurry, double vision n Throat slurring speech, difficulty swallowing n Difficulty breathing n Cardiac problems")
63
Tetanus 1. Tetanus is caused by production of an exotoxin in a localized infection of a wound by Clostridium tetani. Endospores allow for long-term survival in soil. 2. C. tetani produces the neurotoxin tetanospasmin, which causes rigid paralysis with the symptoms of tetanus: spasms, contraction of muscles controlling the jaw, and death resulting from spasms of respiratory muscles. 3. C. tetani is an anaerobe that will grow in unclean wounds and wounds with little bleeding.

64
TETANUS INFECTION CONTROL 1. Acquired immunity results from DPT immunization that includes tetanus toxoid. 2. Following an injury, an immunized person may receive a booster of tetanus toxoid. (TT) 3. ATS prophylaxis (1500 IU) 4. An unimmunized person may receive (human) tetanus immune globulin (ATS therapeutis) 5. Debridement (removal of tissue) and antibiotics may be used to control the infection. Angka kematian 55% - 65% jika tidak imun !!! Angka kematian 55% - 65% jika tidak imun !!!
 3. ATS prophylaxis (1500 IU) 4. An unimmunized person may receive (human) tetanus immune globulin (ATS therapeutis) 5. Debridement (removal of tissue) and antibiotics may be used to control the infection. Angka kematian 55% - 65% jika tidak imun !!. Angka kematian 55% - 65% jika tidak imun !!!.")
65
Botulism 1. Botulism is caused by an exotoxin produced by Clostridium botulinum growing in foods. 2. Serological types of botulinum toxin vary in virulence, with type A being the most virulent. 3. The toxin is a neurotoxin that inhibits the transmission of nerve impulses. 4. Blurred vision occurs in 1-2 days; progressive flaccid paralysis follows for 1-10 days, resulting in respiratory and cardiac failure. 5. C. botulinum will not grow in acidic foods or in an anaerobic environment.

66
Botulism 1. Endospores are killed by proper canning. The addition of nitrites to foods inhibits outgrowth after endospore germination. 2. The toxin is heat labile and is destroyed by boiling (100°C) for 5 minutes. 3. Infant botulism results from the growth of C. botulinum in an infant's intestines and has been associated with the ingestion of honey products. 4. Wound botulism occurs when C. botulinum grows in anaerobic wounds. 5. For diagnosis, mice protected with antitoxin are inoculated with toxin from the patient or foods.
 for 5 minutes. 3. Infant botulism results from the growth of C. botulinum in an infant s intestines and has been associated with the ingestion of honey products. 4. Wound botulism occurs when C. botulinum grows in anaerobic wounds. 5. For diagnosis, mice protected with antitoxin are inoculated with toxin from the patient or foods..")
67
Lyme disease n Lyme disease also may be complicated by early and late neurologic involvement. Mild meningitis and facial palsy often accompany the initial rash and systemic symptoms following the tickbite. n In 15 percent of untreated patients, subacute or recurrent meningitis, encephalitis, cranial nerve palsies, and peripheral neuropathies develop 1 to 9 months later, and rarely a chronic meningoencephalitis has been described years later.

68
DAFTAR PUSTAKA n 1. Alcamo, Edward : Fundamentals of Microbiology. 6th ed. Jones and Bartlett Publshers, Boston, Toronto, London, Singapore., 2001 n 2. Brook,G.F., Butel,J.S., and Ornston,L.N. : Jawetz, Melnick & Adelberg's Medical Microbiology. 20th Ed. A Lang Medical Book, Prentice Hall Int Inc. 1995. n 3. Burdon, K.L. : Textbook of Microbiology. 4 th EdThe Macmillan Co New Jork 1961 n 4. Lennette,E.H.,Balow,A., Hausler,W. and Truant, J.P. : Manual of Clinical Microbiology, 3 Amer Society for Microbiol, Washington,D.C., 1980 n 5. Levin, W and Jaetz E. : Medical Microbiology & Immunology.6 th Ed. Lange Medical Books / McGraw- Hill, 2000. n 6. Pelczar,M.J.Jr., Chan,E.C.S. and Krieg,N.R. : Microbiology Concepts and Applications. International Ed. McGraw-Hill, Inc, 1993

Presentasi serupa




. The genome is surrounded by a large number of proteins (coat.>")










>")




 Hidsal Jamil(135020100111028) Padel Aji Pamungkas(135020100111042)>")
