Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
SEKILAS PENATALAKSANAAN NYERI
Dr. AWALUDDIN NOOR, Sp.S Prima Resort Kuningan 9 April 2010

2
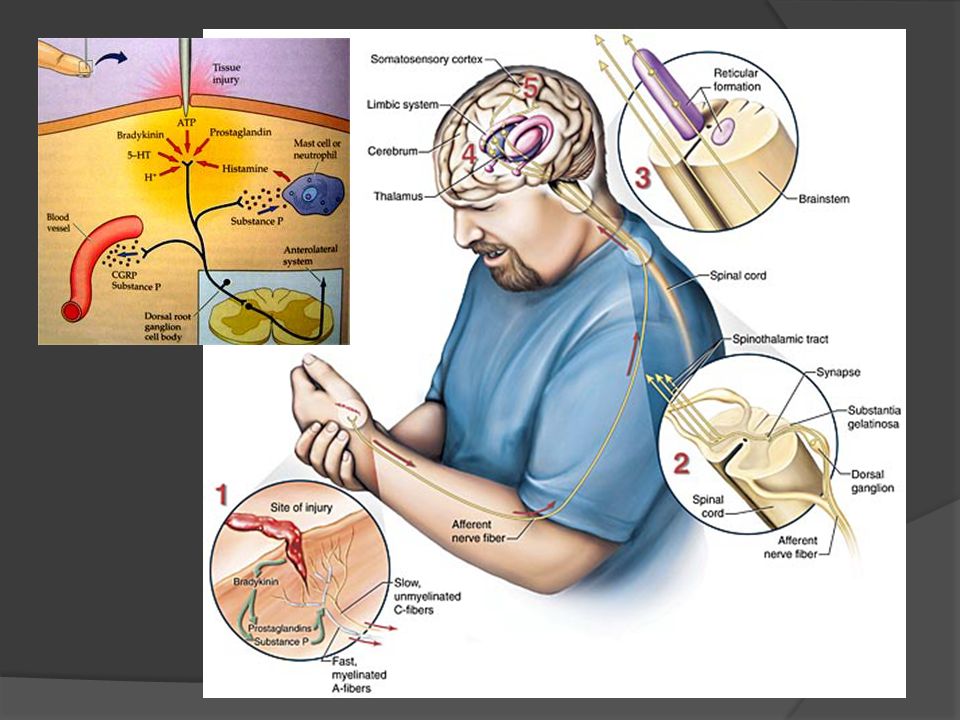
Definisi Nyeri (Pain) dari IASP
(International Association for the Study of Pain) Pain (Nyeri) adalah suatu pengalaman sensorik dan emosional yang berkaitan dengan kerusakan jaringan atau diduga ada kerusakan jaringan Nyeri adalah pengalaman sensorik yang berkaitan dengan aktivasi nociceptor dan lintasan nyeri Nyeri adalah suatu pengalaman emosional Kerusakan jaringan tidak mesti ada
 Pain (Nyeri) adalah suatu pengalaman sensorik dan emosional yang berkaitan dengan kerusakan jaringan atau diduga ada kerusakan jaringan. Nyeri adalah pengalaman sensorik yang berkaitan dengan aktivasi nociceptor dan lintasan nyeri. Nyeri adalah suatu pengalaman emosional. Kerusakan jaringan tidak mesti ada.")
3
JENIS NYERI Neuropathic Pain Inflammatory Pain
Pain initiated or caused by a primary lesion or dysfunction in the nervous system (either peripheral or central nervous system)1 Inflammatory Pain Pain caused by injury to body tissues (musculoskeletal, cutaneous or visceral)2 Mixed Pain Pain with neuropathic and nociceptive components Examples Peripheral Post herpetic neuralgia Trigeminal neuralgia Diabetic peripheral neuropathy Postsurgical neuropathy Posttraumatic neuropathy Central Posts troke pain Common descriptors2 Burning Tingling Hypersensitivity to touch or cold Examples Pain due to inflammation Limb pain after a fracture Joint pain in osteoarthritis Postoperative visceral pain Common descriptors2 Aching Sharp Throbbing Examples Low back pain with radiculopathy Cervical radiculopathy Cancer pain Carpal tunnel syndrome 1. International Association for the Study of Pain. IASP Pain Terminology. 2. Raja et al. in Wall PD, Melzack R (Eds). Textbook of pain. 4th Ed ;11-57 LYRICA Neuropathic Pain Slide Kit: February 2005 Update
1. Inflammatory Pain. Pain caused by injury to body tissues (musculoskeletal, cutaneous or visceral)2. Mixed Pain. Pain with. neuropathic and. nociceptive. components. Examples. Peripheral. Post herpetic neuralgia. Trigeminal neuralgia. Diabetic peripheral neuropathy. Postsurgical neuropathy. Posttraumatic neuropathy. Central. Posts troke pain. Common descriptors2. Burning. Tingling. Hypersensitivity to touch or cold. Examples. Pain due to inflammation. Limb pain after a fracture. Joint pain in osteoarthritis. Postoperative visceral pain. Common descriptors2. Aching. Sharp. Throbbing. Examples. Low back pain with radiculopathy. Cervical radiculopathy. Cancer pain. Carpal tunnel syndrome. 1. International Association for the Study of Pain. IASP Pain Terminology. 2. Raja et al. in Wall PD, Melzack R (Eds). Textbook of pain. 4th Ed ; LYRICA Neuropathic Pain Slide Kit: February 2005 Update.")
4
Neuropathic Pain is Different from Muscle/skeletal Pain
Chronic pain (months/years) Acute pain (hours or days) Caused by injury or disease to nerves Caused by injury or inflammation that affects both the muscles and joints Mild to excruciating pain that can last indefinitely Moderate to severe pain that disappears when the injury heals Causes extreme sensitivity to touch –simply wearing light clothing is painful Causes sore, achy muscles Sufferers can become depressed or socially withdrawn because they see no relief in sight and may experience sleep problems Sufferers can become anxious and distressed but optimistic about relief from pain Wall PD. Textbook of Pain. 4th ed; 1999; Jude EB. Clin in Pod Med and Surg.1999;16:81-97; Price SA. Pathophysiology: Clinical Concepts of Disease Processes. 5th ed; 1997: Goldman L. Cecil Textbook of Medicine. 21st ed; 2000
 Acute pain (hours or days) Caused by injury or disease to nerves. Caused by injury or inflammation that affects both the muscles and joints. Mild to excruciating pain that can last indefinitely. Moderate to severe pain that disappears when the injury heals. Causes extreme sensitivity to touch –simply wearing light clothing is painful. Causes sore, achy muscles. Sufferers can become depressed or socially withdrawn because they see no relief in sight and may experience sleep problems. Sufferers can become anxious and distressed but optimistic about relief from pain. Wall PD. Textbook of Pain. 4th ed; 1999; Jude EB. Clin in Pod Med and Surg.1999;16:81-97; Price SA. Pathophysiology: Clinical Concepts of Disease Processes. 5th ed; 1997: Goldman L. Cecil Textbook of Medicine. 21st ed;")
5
Symptoms of Neuropathic Pain Characterized Differently
Muscle/Skeletal Pain Neuropathic Pain Price SA. Pathophysiology: Clinical Concepts of Disease Processes. 5th ed; 1997; Galer BS et al. Diabetes Res Clin Pract. 2000;47:

11
Neurophatic pain Nociceptive/ imflammatory/ musculoskletal pain

12
Thick, myelinated, fast conducting neurons
Mediate the feeling of initial fast, sharp, highly localized pain. Very thin, unmyelinated, slow-conducting Mediate slow, dull, more diffuse, often burning pain. Rabaan Tekanan

13
Nerve Fibers Class Velocity Function A- Fast Motor A- A-
Touch, pressure A- Intermediate Muscle tone A- Pain, temperature B Small C Pain

14
Targets of Pain Therapies
Pharmacotherapy Non-opioid analgesics Opioid analgesics Nerve Blocks Adjuvant analgesics (neuropathic, musculoskeletal) tramadol Acetaminofen Electrical Stimulation Transcutaneous electrical nerve stimulation (TENS) Percutaneous electrical nerve stimulation (PENS) Alternative methods Acupuncture Physical Therapy Chiropractics Surgery (NSAID) Gottschalk et al., 2001
 tramadol. Acetaminofen. Electrical Stimulation. Transcutaneous electrical nerve stimulation (TENS) Percutaneous electrical nerve stimulation (PENS) Alternative methods. Acupuncture. Physical Therapy. Chiropractics. Surgery. (NSAID) Gottschalk et al.,")
15
ABC Tx. Nyeri Anamnesa nyeri secara sistematik dan teratur
Berpikiran positif (percaya) terhadap keluhan pasien atau keluarga Carilah metode kontrol nyeri yang nyaman untuk pasien dan keluarga Dilakukan intervensi yang tepat waktunya, logis dan terkoordinasi Edukasi pasien dan keluarga untuk mengatasi nyeri sekuat mungkin
 terhadap keluhan pasien atau keluarga. Carilah metode kontrol nyeri yang nyaman untuk pasien dan keluarga. Dilakukan intervensi yang tepat waktunya, logis dan terkoordinasi. Edukasi pasien dan keluarga untuk mengatasi nyeri sekuat mungkin.")
16
Analgesics Non-opioid analgesics (non-opioids): paracetamol, acetylsalicylic acid, metamizole* and nonsteroidal anti-inflammatory drugs (NSAIDs). Opioid analgesics (opioids): weak opioids (codeine, dihydrocodeine, tramadol) and strong opioids (i.e., morphine). Co-analgesics: a diverse group of drugs, with primary indications for conditions other than pain, with analgesic properties relevant to some conditions. Commonly used adjuvant analgesics include antiepileptic drugs (AEDs), tricyclic antidepressants (TCAs) and local anaesthetics (LAs). Papaver somniferum
: weak opioids (codeine, dihydrocodeine, tramadol) and strong opioids (i.e., morphine). Co-analgesics: a diverse group of drugs, with primary indications for conditions other than pain, with analgesic properties relevant to some conditions. Commonly used adjuvant analgesics include antiepileptic drugs (AEDs), tricyclic antidepressants (TCAs) and local anaesthetics (LAs). Papaver somniferum.")
18
Diagnosis Drug Treatment Acute and chronic pain
NSAIDS , Opioids (al tramadol), Paracetamol Myofascial pain dysfunction Analgesics , tricyclics, centrally-acting muscle relaxants, glucocorticoids Neuropathic pain, neuralgias Carbamazepine, phenytoin, baclofen, tricyclics, gabapentin, others?
, Paracetamol. Myofascial pain dysfunction. Analgesics , tricyclics, centrally-acting muscle relaxants, glucocorticoids. Neuropathic pain, neuralgias. Carbamazepine, phenytoin, baclofen, tricyclics, gabapentin, others")
20
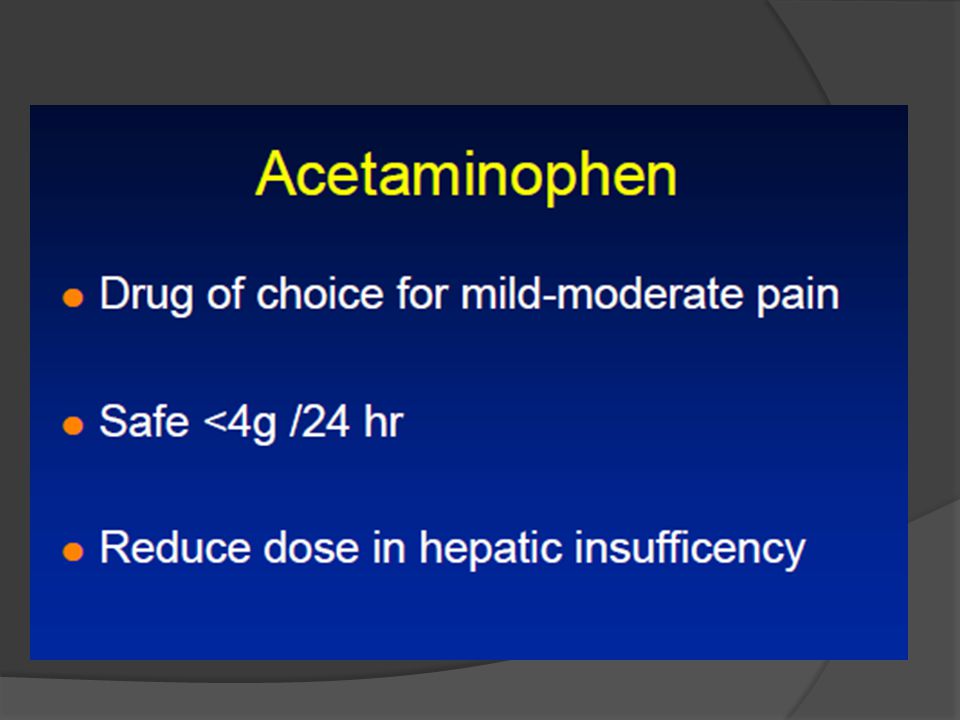
Acetaminophen May inhibit COX selectively in central nervous system
Only weak inhibitor of peripheral COX (peroxide effects?) Inhibits effects of substance P in CNS? Inhibits effects of glutamate in CNS?
 Inhibits effects of substance P in CNS Inhibits effects of glutamate in CNS")
21
Paracetamol Paracetamol is an effective analgesic for acute pain (Level I*). Paracetamol is an effective adjunct to opioids (Level I). NSAIDs given in addition to paracetamol improve analgesia (Level I). IV paracetamol is an effective analgesic after surgery (Level II), is as effective as ketorolac (Level II) and equivalent to morphine after dental surgery with better tolerance (Level II).
. IV paracetamol is an effective analgesic after surgery (Level II), is as effective as ketorolac (Level II) and equivalent to morphine after dental surgery with better tolerance (Level II).")
22
Mekanisme Kerja Tramadol
Dua mekanisme kerja yang saling melengkapi: 1. Kerja di opioid: - Agonis reseptor µ - Metabolit aktif (O-desmethyl-tramadol/M1) 2. Kerja di monoaminergic: Menghambat re-uptake serotonin/noradrenalin
 2. Kerja di monoaminergic: Menghambat re-uptake serotonin/noradrenalin.")
23
Mekanisme Kerja Tramadol
Menuju Otak Descending pathway Neuron dari saluran spinothalamic Serotonin/Noradrenalin µ-Receptor Tramadol 2 -Receptor The two mechanisms of tramadol interact synergistically at the dorsal horn neurones of the spinal cord which are involved in the transmission and modification of peripheral pain signals. The dorsal horn cells have plenty of opioid receptors. Activation of these receptors by endogenous endorphins or opioid drugs interrupts the transmission of pain to the brain. These cells can also be switched off by the brain in situations of high attention or stress. This is caused by release of the transmitter norepinephrine (NE = noradrenaline) from descending nerve pathways. The effect can be enhanced by monoaminergic drugs such as NE reuptake inhibitors (e.g. antidepressants). Transmiter nyeri Spinal neuron Rangsang Nyeri Enkephalin
 from descending nerve pathways. The effect can be enhanced by monoaminergic drugs such as NE reuptake inhibitors (e.g. antidepressants). Transmiter nyeri. Spinal neuron. Rangsang Nyeri. Enkephalin.")
25
PAIN PHARMACOTHERAPHY
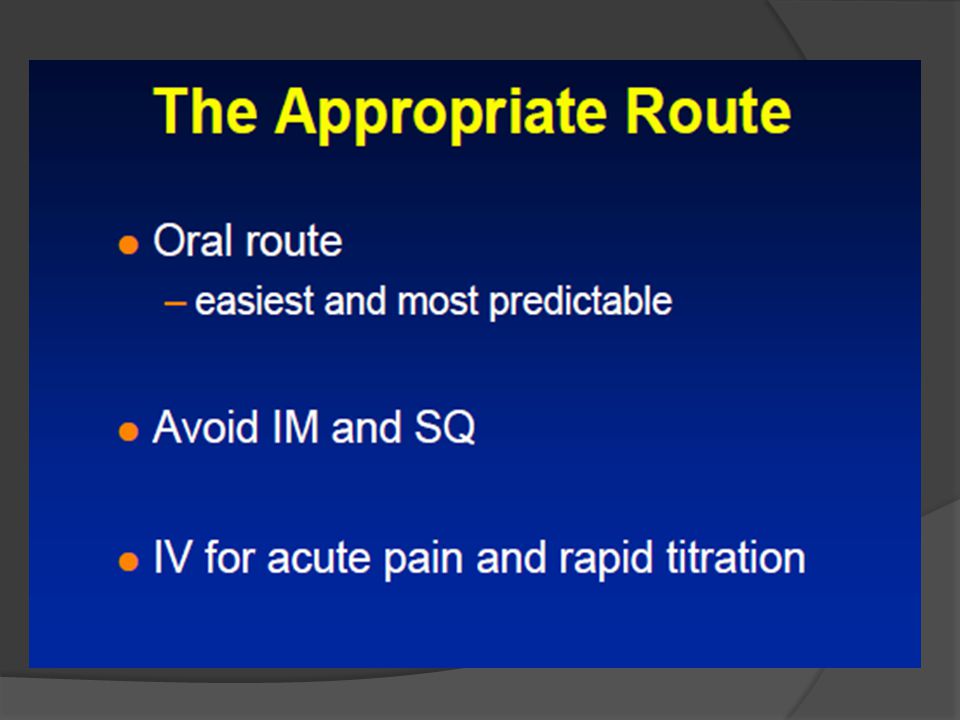
Choose drugs based on: – mechanism of pain – safety and pharmacology of aging – match pain severity with drug potency – use combined drug and non-drug strategies Use adequate dose; appropriate route Anticipate, prevent and manage side effects

26
Rationale for a fixed-dose combination analgesic
Enhanced analgesia Reduced doses of components - fewer side effects Rapid onset of action and lasting duration Broad spectrum of efficacy in terms of indications and pain intensity Higher patient compliance and ease of administration

27
Fixed drug combinations ( ZALDIAR)
Fixed combinations are appropriate for on-demand treatment typically used in acute pain conditions and situations of non-stable pain or intermittent pain in chronic conditions. A fixed analgesic combination simplifies drug delivery without the need for complicated dose-escalating regimens and, therefore, improves compliance. Free drug combinations Free drug combinations are particularly appropriate for the management of stable chronic pain syndromes. The main advantage of free drug combinations is that they allow the dose regimen to be tailored to individual requirements. On the other hand, this may be time-consuming because it involves a gradual and dose-escalating strategy.

28
Kombinasi NSAID Kombinasi 2 NSAID:
Tidak dianjurkan Efek samping meningkat Tidak menambah efikasi Kombinasi NSAID dan Analgetik (paracetamol) Masih dapat dipertanggungjawabkan Kombinasi NSAID dengan Pelindung Lambung: Ditujukan untuk sedikit mengatasi masalah efek samping terhadap lambung. Dapat diberikan bersama golongan PPI, Misoprostol
 Masih dapat dipertanggungjawabkan. Kombinasi NSAID dengan Pelindung Lambung: Ditujukan untuk sedikit mengatasi masalah efek samping terhadap lambung. Dapat diberikan bersama golongan PPI, Misoprostol.")
29
(37,5 MG TRAMADOL PLUS 325 MG PARASETAMOL)
ZALDIAR (37,5 MG TRAMADOL PLUS 325 MG PARASETAMOL) PHAROS INDONESIA
 PHAROS INDONESIA.")
30
Komposisi : Indikasi : Sediaan : Kemasan :
37.5 mg Tramadol plus 325 mg Taracetamol Indikasi : Mengurangi nyeri sedang sampai berat Sediaan : Tablet salut film Kemasan : Box isi 10 tablet Harga 1 box : Rp Harga 1 tablet Rp

31
INDIKASI ZALDIAR Nyeri sedang sampai berat seperti :
Nyeri Pasca Operasi Nyeri Osteoarthritis Tambahan pengobatan pada OA/RA yang telah diberi NSAID/COX-2 Rehabilitasi pasca cedera olahraga Trauma karena kecelakaan Bedah minor Low-back pain

32
Dosis Untuk Dewasa (>12 Tahun)
Dosis ZALDIAR fleksibel tergantung dari intensitas nyeri. Untuk nyeri yang berat dosis awal bisa tablet kemudian diberikan setiap 6 jam Rata-rata dosis per hari 3-4 tablet Maksimal 8 tablet per hari (Sama dengan 300 mg tramadol/2600 mg parasetamol)
")
33
ZALDIAR: Onset cepat durasi lama
Pain relief probabilities Kerja analgesik yang saling melengkapi: Onset cepat dari parasetamol dikombinasi dengan durasi lama dari tramadol

34
Perhatian pada kelompok pasien berikut :
ZALDIAR® jangan diberikan pada: Anak-anak <12 tahun Selama hamil Selama menyusui Kategori ZALDIAR C

35
Kontraindikasi Hipersensitif terhadap tramadol dan parasetamol
Acute intoxication alkohol, hypnotic, analgesik sentral, opioids atau obat psychotropic Pemberian bersamaan dengan MAO inhibitor or within two weeks of withdrawal Gangguan fungsi hati berat Epilepsi yang tidak sedang dalam pengobatan

36
Peringatan Dosis maksimal 8 tablet per hari
No concurrent use of any other products containing paracetamol or tramadol Tidak direkomendasikan pada pasien dengan gangguan ginjal (creatinin clearance <10ml/mm) Jangan diberikan pada pasien dengan gangguan hati berat Tidak direkomendasikan pada pasien dengan gangguan pernafasan berat
 Jangan diberikan pada pasien dengan gangguan hati berat. Tidak direkomendasikan pada pasien dengan gangguan pernafasan berat.")
37
Interaksi Kontra indikasi / tidak direkomendasikan digunakan bersamaan dengan: MAO inhibitors, Alcohol, Carbamazepine, Opioid agonists-antagonists

38
STUDI KLINIS

39
Nyeri setelah bedah mulut (gigi)
Medve RA et al. Anesthesi Prog, 2001 Tujuan: Membandingkan efikasi dan keamanan dari tramadol/parasetamol (ZALDIAR) dengan tramadol atau parasetamol monoterapi Dosis: Tramadol 75 mg/parasetamol 650 mg 75 mg tramadol 650 mg parasetamol 400 mg ibuprofen Plasebo The studies in pain after oral surgery were single-dose studies. The dental pain model was used to reflect acute pain for the determination of the therapeutic profile of tramadol/paracetamol in this kind of pain. This model evaluates pain relief and intensity after molar extraction and is frequently employed to demonstrate efficacy of analgesics in comparison to a standard substance which is needed to control the sensitivity of the model. The apparent efficacy of an analgesic can vary greatly depending on the pain model which is studied. In this study the combination was compared to tramadol, paracetamol, placebo and ibuprofen, as active control to prove the model sensitivity. The model was used to compare the efficacy and safety of the combination tramadol/paracetamol in acute pain with its components.
 dengan tramadol atau parasetamol monoterapi. Dosis: Tramadol 75 mg/parasetamol 650 mg. 75 mg tramadol. 650 mg parasetamol. 400 mg ibuprofen. Plasebo. The studies in pain after oral surgery were single-dose studies. The dental pain model was used to reflect acute pain for the determination of the therapeutic profile of tramadol/paracetamol in this kind of pain. This model evaluates pain relief and intensity after molar extraction and is frequently employed to demonstrate efficacy of analgesics in comparison to a standard substance which is needed to control the sensitivity of the model. The apparent efficacy of an analgesic can vary greatly depending on the pain model which is studied. In this study the combination was compared to tramadol, paracetamol, placebo and ibuprofen, as active control to prove the model sensitivity. The model was used to compare the efficacy and safety of the combination tramadol/paracetamol in acute pain with its components.")
40
Desain penelitian: 1200 pasien dengan nyeri sedang sampai berat setelah bedah (cabut) gigi geraham paling belakang (geraham bungsu) yang di random menjadi 3, double blind, paralel group, studi dosis tunggal yang diobservasi selama 8 jam. Tiga pusat penelitian terdiri dari 400 pasien; yang terdistribusi merata dalam pengobatan Patients included in this trial were suffering from moderate or severe pain ( 5 on a 10-point visual analogue scale) following extraction of third molars requiring bone removal. The treatment groups in each study were similar at baseline. Medve RA et al. Anesth Prog, 2001
 gigi geraham paling belakang (geraham bungsu) yang di random menjadi 3, double blind, paralel group, studi dosis tunggal yang diobservasi selama 8 jam. Tiga pusat penelitian terdiri dari 400 pasien; yang terdistribusi merata dalam pengobatan. Patients included in this trial were suffering from moderate or severe pain ( 5 on a 10-point visual analogue scale) following extraction of third molars requiring bone removal. The treatment groups in each study were similar at baseline. Medve RA et al. Anesth Prog,")
41
Hasil penelitian: efikasi
The efficacy was evaluated by using total pain relief over 8 hours (TOTPAR8) and the sum of pain intensity differences (SPID8). For this determination pain relief (scale, 0 = none to 4 = complete) and pain intensity (scale, 0 = none to 3 = severe) were reported 30 min after dosing and then hourly for 8 hours. Total pain relief over 8 hours and the sum of pain intensity differences were calculated from the hourly scores. The overall pain relief (TOTPAR8) as well as the mean overall changes in pain intensity (SPID8) after 8 hours were significantly higher in the tramadol/paracetamol group as compared to tramadol and paracetamol alone. As expected, the sensitivity of the model was confirmed by the good response of ibuprofen (gold standard in this pain model) compared with placebo. *P vs Tramadol/paracetamol; †P = vs Tramadol/paracetamol; ‡P vs all active treatments TOTPAR 8 = Total pengurangan nyeri dalam 8 jam SPID = Jumlah perbedaan intensitas nyeri dalam 8 jam
 and the sum of pain intensity differences (SPID8). For this determination pain relief (scale, 0 = none to 4 = complete) and pain intensity (scale, 0 = none to 3 = severe) were reported 30 min after dosing and then hourly for 8 hours. Total pain relief over 8 hours and the sum of pain intensity differences were calculated from the hourly scores. The overall pain relief (TOTPAR8) as well as the mean overall changes in pain intensity (SPID8) after 8 hours were significantly higher in the tramadol/paracetamol group as compared to tramadol and paracetamol alone. As expected, the sensitivity of the model was confirmed by the good response of ibuprofen (gold standard in this pain model) compared with placebo. *P vs Tramadol/paracetamol; †P = vs Tramadol/paracetamol; ‡P vs all active treatments. TOTPAR 8 = Total pengurangan nyeri dalam 8 jam. SPID = Jumlah perbedaan intensitas nyeri dalam 8 jam.")
42
Kesimpulan penelitian ZALDIAR pada pasien bedah gigi
Pengurangan / penurunan intensitas nyeri dengan ZALDIAR lebih superior dibanding tramadol atau parasetamol sendiri atau plasebo Mula kerja ZALDIAR lebih cepat dan durasi kerja lebih lama dibanding tramadol atau parasetamol sendiri. Masing-masing komponen dari ZALDIAR berkontribusi terhadap efikasi analgesik ZALDIAR adalah analgesik kuat dengan onset cepat, durasi panjang yang efektif dalam pengobatan nyeri akut In summary, the single-dose studies in post-surgical dental pain showed that pain relief and improvements in pain intensity associated with tramadol/paracetamol are superior to placebo, tramadol or paracetamol alone. It is apparent that tramadol/paracetamol is a rapidly acting, long-lasting analgesic that is effective and well tolerated in the treatment of acute pain.

43
Efek samping setelah pemberian ZALDIAR ( 5%)
Tramadol/ paracetamol (n=240) Tramadol (n=238) Paracetamol Ibuprofen Placebo (n=239) Nausea (mual) 56 (23%) 56 (24%) 22 (9%) 23 (10%) 38 (16%) Vomiting (muntah) 51 (21%) 49 (21%) 17 (7%) 16 (7%) Dizzines (pusing) 11 (5%) 12 (5%) 10 (4%) 7 (3%) 9 (4%) The adverse events in the tramadol/paracetamol group were generally transient and mild or moderate in severity. Based on the same dose of tramadol the side effect profiles and incidences were comparable between the tramadol/paracetamol group and the tramadol group. Nausea, vomiting and dizziness were the most common side effects.
 Tramadol. (n=238) Paracetamol. Ibuprofen. Placebo. (n=239) Nausea. (mual) 56 (23%) 56 (24%) 22 (9%) 23 (10%) 38 (16%) Vomiting. (muntah) 51 (21%) 49 (21%) 17 (7%) 16 (7%) Dizzines. (pusing) 11 (5%) 12 (5%) 10 (4%) 7 (3%) 9 (4%) The adverse events in the tramadol/paracetamol group were generally transient and mild or moderate in severity. Based on the same dose of tramadol the side effect profiles and incidences were comparable between the tramadol/paracetamol group and the tramadol group. Nausea, vomiting and dizziness were the most common side effects.")
44
Hasil penelitian: onset (mula kerja)
The time to onset of pain relief was determined by the double-stopwatch technique. The estimated time of onset of pain relief for tramadol/paracetamol was minutes and was found to be significantly faster as compared to tramadol with 51 minutes.

45
Hasil penelitian: durasi kerja
The time to remedication was used as a measure of the pain relief duration. The duration of pain relief provided by tramadol/paracetamol (5 hours) was longer compared to tramadol or paracetamol (2 to 3 hours).
 was longer compared to tramadol or paracetamol (2 to 3 hours).")
46
Pain: A conceptual approach to treatment (Biopsycosocial approach)
Anti-depressants / psychotropics Relaxation Spiritual Cognitive therapies Functional restoration Pain Behaviors Suffering Pain Perception Nociception Opioid Adjuvants NSAIDs? Acetaminophene Neural augmentation Ablative surgery Local block NSAIDs (Movicox ®) Surgery Physical modalities 1. Looser JD, Cousins MJ. Med J aust 1990;216: ; 2. van den Hout JH, et al. Clin J Pain. 2003;19:87-96.; 3. Mynors-Wallis L, et al. Br J Psychiatry. 1997;170: ; 4. Morley S, et al. Pain. 1999;80:1-13.
 Surgery. Physical modalities. 1. Looser JD, Cousins MJ. Med J aust 1990;216: ; 2. van den Hout JH, et al. Clin J Pain. 2003;19:87-96.; 3. Mynors-Wallis L, et al. Br J Psychiatry. 1997;170: ; 4. Morley S, et al. Pain. 1999;80:1-13.")
47
HATUR NUHUN

Presentasi serupa






>")
>")











