Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
THYROIDECTOMY INK

2
THYROID GLAND

3
TWO LOBES JOINED BY ISTHMUS PYRAMIDAL LOBE (80%)PROJECT UPWARDS FROM ISTHMUS OR EITHER OF THE LOBES A FIBROMUSCULAR BAND levator glandulae thyroideae DESCEND FROM THE BODY OF THE HYOID BONE TO ISTHMUS OR TO PYRAMIDAL LOBE FROM GREEK thyreoeides= SHIELD SHAPE
PROJECT UPWARDS FROM ISTHMUS OR EITHER OF THE LOBES A FIBROMUSCULAR BAND levator glandulae thyroideae DESCEND FROM THE BODY OF THE HYOID BONE TO ISTHMUS OR TO PYRAMIDAL LOBE FROM GREEK thyreoeides= SHIELD SHAPE")
4
GLAND LIES AGAINST C5,6,7 &T1 VERTEBRAE CLASPS THE UPPER PART OF TRACHEA EACH LOBE EXTENDS FROM MIDDLE OF THYROID CARTILAGE TO 4TH OR 5TH TRACHEAL RING ISTHMUS EXTENDS FROM 2ND TO THE 3RD TRACHEAL

5
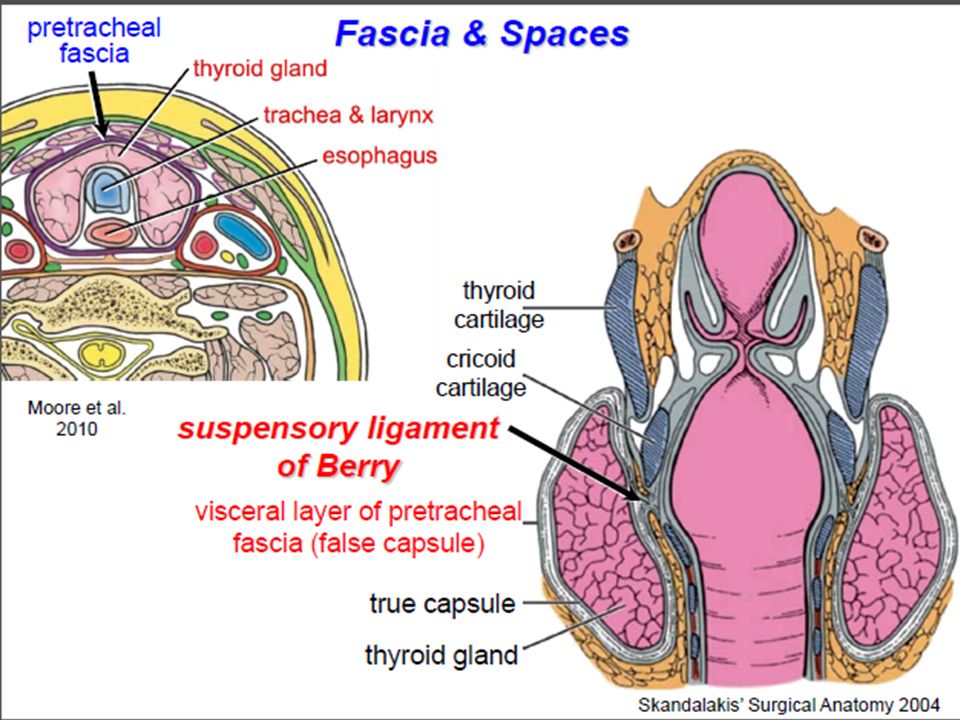
1.investing fascia 2.pretracheal fascia a.muscular layer b. visceral layer 3. prevertebral fascia 4. carotid sheath

7
Relation with Strap muscles Lateral ‐sternothyroid Anterior ‐omohyoid muscle ‐sternohyoid Inferior ‐SCM (lower portion) ** motor nerve supply from the ansa cervicalis enters these muscles inferiorly.
 ** motor nerve supply from the ansa cervicalis enters these muscles inferiorly.")
8
VASCULAR ANATOMY HIGHLY VASCULAR SUPERIOR THYROID ARTERY INFERIOR THYROID ARTERIES IMA THYROID ARTERY (rare) 3 VEINS SUP THYROID VEIN drains into IJV or COMMON FACIAL V. MIDDLE THYROID VEIN drains to IJV INFERIOR THYROID VEIN into LEFT BRACHICEPHALIC V. A 4 TH VEIN OF KOCHER’S emerge between MIDDLE and INFERIOR VEIN and drain into IJV

9
INNERVATION Principally from ANS Parasympathetic fibers – from vagus Sympathetic fibers –from superior, middle, and inferior ganglia of the sympathetic trunk Enter the gland along with the blood vessels.

12
LYMPHATICS PRIMARILY TO INTERNAL JUGULAR NODES SUPERIOR POLE & MEDIAL ISTHMUS TO SUPERIOR GROUP LOWER POLE OF THYROID TO INFERIOR GROUP EMPTY INTO PRETRACHEAL & PARATRACHEAL NODES

13
EMBRYOLOGY PROLIFERATION OF THE ENDODERMAL CELLS ON THE MIDLINE PHARYNGEAL FLOOR SURGICAL SIGNIFICANCE OF THYROID EMBRYOLOGY – ANOMALIES OF SHAPE – ANOMALIES OF POSITION – ECTOPIC THYROID – THYROGLOSSAL CYST – THYROGLOSSAL FISTULA

14
THYROIDECTOMY

15
INDICATION To establish a definitive diagnosis of a mass within the thyroid gland, especially when cytologic analysis after fine-needle aspiration (FNA) is either nondiagnostic, equivocal, or indeterminate To treat benign and malignant thyroid tumors To alleviate pressure symptoms or respiratory difficulties associated with a benign or malignant process A multinodular goiter with continued enlargement and symptoms ranging from dysphagia, choking, pain, or cosmetic concerns; Occasionally hyperthyroidism particularly if radioiodine ablation or antithyroid medications are contraindicated.
 is either nondiagnostic, equivocal, or indeterminate To treat benign and malignant thyroid tumors To alleviate pressure symptoms or respiratory difficulties associated with a benign or malignant process A multinodular goiter with continued enlargement and symptoms ranging from dysphagia, choking, pain, or cosmetic concerns; Occasionally hyperthyroidism particularly if radioiodine ablation or antithyroid medications are contraindicated.")
16
TECHNIQUE Proper positioning of the patient is critical for adequate exposure of the thyroid gland The incision line is normally approximately two fi ngerbreadths above the sternal notch, placed to conform to Langer’s lines

17
Flaps are then mobilized superiorly and inferiorly using the cautery, just deep to the platysma muscle. The superior flap is extended to the level of the thyroid cartilage and the inferior flap extends to the clavicular heads and suprasternal notch

18
The dissection then proceeds in the midline raphe, which provides a bloodless plane for the separation of the strap muscles

19
The thyroid lobe is further exposed by mobilizing the strap muscles away from the lobe using a sharp dissection If transection of the strap muscles is necessary, this should be performed superiorly to minimize denervation, because both of these muscle groups are innervated from a caudal direction through the ansa hypoglossi nerves

20
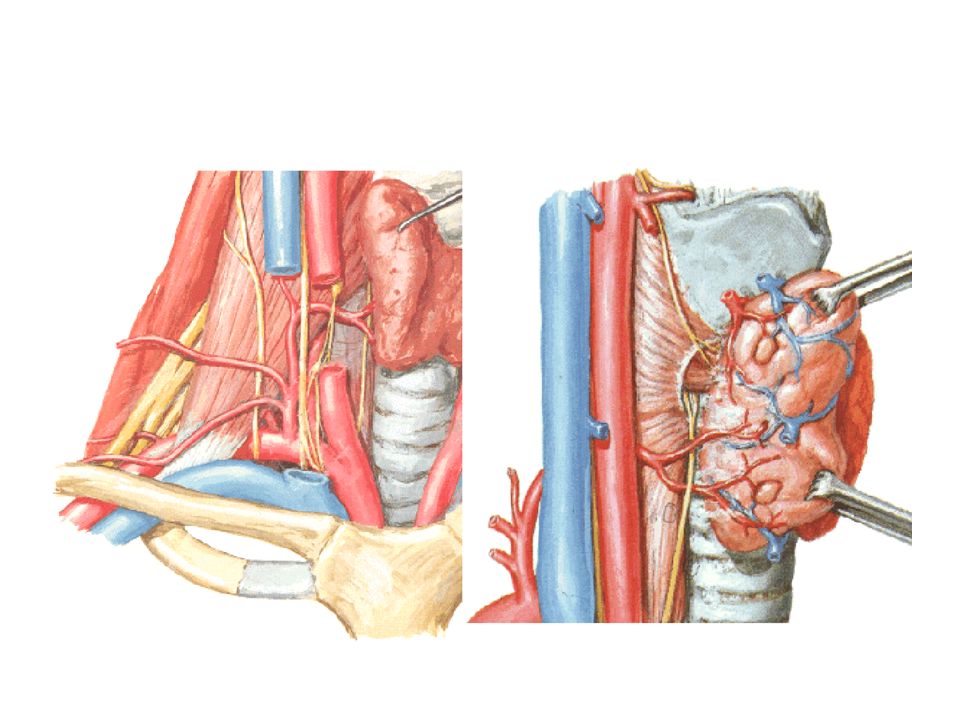
The thyroid gland is regrasped with the Babcock clamp and retracted downward to expose the superior pole vessels, including the branches of the superior thyroid artery. The external branch of the superior laryngeal nerve courses along the cricothyroid muscle just medial to the superior pole vessels

21
Babcock clamp is repositioned to grasp the thyroid lobe so that the inferior thyroid veins can be exposed and ligated as they enter the thyroid gland. Occasionally, a venous plexus (i.e., thyroid ima) is noted in the midline position
 is noted in the midline position.")
22
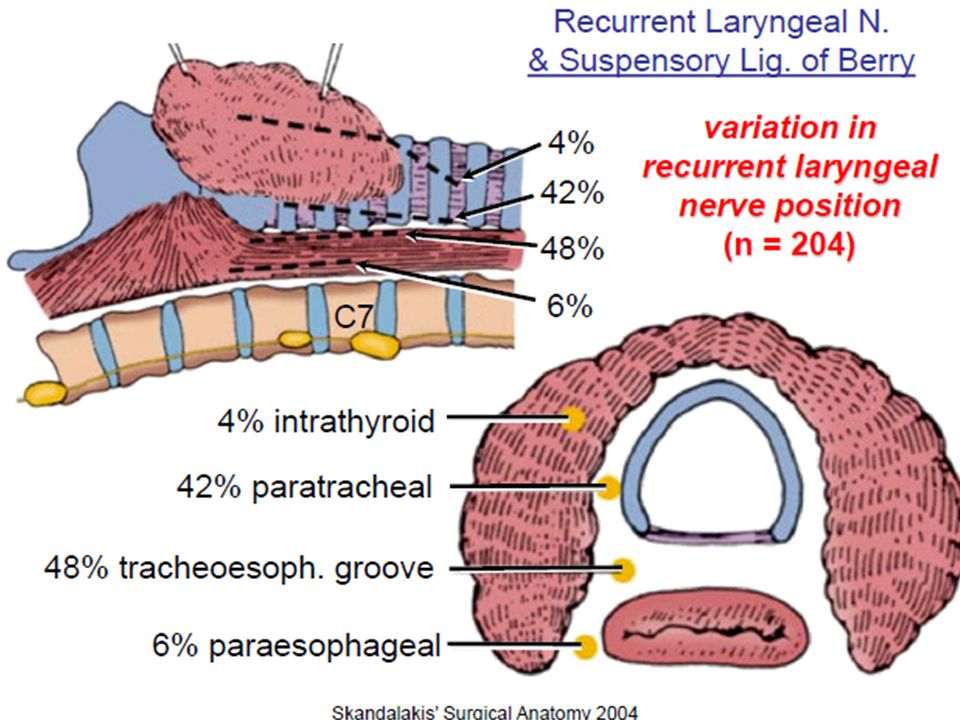
As the thyroid lobe is retracted medially, gentle dissection is performed to expose the parathyroid glands, inferior thyroid artery, and recurrent laryngeal nerve. The recurrent nerve usually passes behind the inferior thyroid artery in the tracheoesophageal groove Parathyroid glands that lie on the thyroid surface can be mobilized with their vascular supply and thus preserved

23
The connective tissue (ligament of Berry), which tethers the thyroid gland to the tracheal rings, is then carefully divided by sharp dissection Dissection of the thyroid from the trachea can then be performed with the electrocautery by division of the loose connective tissue between the structures
, which tethers the thyroid gland to the tracheal rings, is then carefully divided by sharp dissection Dissection of the thyroid from the trachea can then be performed with the electrocautery by division of the loose connective tissue between the structures")
24
If lobectomy is indicated, then the isthmus is clamped using a Kocher or tonsil clamp divided, and oversewn with an interlocking continuous 3-0 Vicryl suture If total thyroidectomy is indicated, the operation is continued in a similar fashion on the other side to remove the thyroid gland in toto and to preserve both the parathyroid glands and the recurrent laryngeal nerves

25
POST OPERATIVE CARE One of the most immediate postoperative complications can be wound hematoma, A small hematoma in this location can severely compromise respirations and should be immediately evacuated Injury of a recurrent laryngeal nerve can lead to hoarseness; bilateral injury of the recurrent laryngeal nerves may result in paralysis of both vocal cords, which would require reintubation and possibly tracheostomy. Postoperative hypoparathyroidism is usually a transient phenomenon that is relatively rare but occurs more often after total thyroidectomy. Calcium replacement and possibly vitamin D may be required to maintain adequate serum calcium levels

26
PERAWATAN POST OPERASI Komplikasi dini : – Perdarahan. – Paralisis n.rekuren laringeus dan n.laringes superior (“ vocal fatique ”). – Trakeomalasia ( stridor inspirasi ). – Infeksi luka operasi. – Komplikasi metabolik Tetani hipokalsemia ( Strumipriva ). Krisis tiroid (“ thyroid strom ”). KOMPLIKASI POST OPERASI
. – Trakeomalasia ( stridor inspirasi ). – Infeksi luka operasi. – Komplikasi metabolik Tetani hipokalsemia ( Strumipriva ). Krisis tiroid ( thyroid strom ). KOMPLIKASI POST OPERASI.")
27
Komplikasi lanjut : – Keloid luka operasi. – Hipotiroid (expected) Evaluasi TSH, FT3, FT4. Thyroxin oral.

28
Follow Up Follow-up : 1st year: every 3 mo 2nd year: every 4 mo 3rd, 4th year: every 6 mo 5th: every year Evaluate : clinical feature and thyroid function test

29
TERIMA KASIH

Presentasi serupa












>")






