Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
(Leukotriene Receptor Antagonist) in Management of Asthma
GINA : The Role of LTRA (Leukotriene Receptor Antagonist) in Management of Asthma SUSANTHY DJ Medical Functional Staf Saiful Anwar Hospital, Pulmonology and Respiratory Medicine, Medical Faculty, Brawijaya University Malang
 in Management of Asthma. SUSANTHY DJ. Medical Functional Staf Saiful Anwar Hospital, Pulmonology and Respiratory Medicine, Medical Faculty, Brawijaya University Malang.")
2
Goals of asthma management
The long-term goals of asthma management are Symptom control: to achieve good control of symptoms and maintain normal activity levels Risk reduction: to minimize future risk of exacerbations, fixed airflow limitation and medication side-effects GINA 2016

3
A Real Life Issue in Asthma Management
Many asthma patients remain uncontrolled: 94.7% did not meet all GINA criteria for asthma controla (AIRE Study)1 51% did not meet criteria for asthma control despite the use of an ICS or an ICS + LABA (INSPIRE study)2
1. 51% did not meet criteria for asthma control despite the use of an ICS or an ICS + LABA (INSPIRE study)2.")
4
Studi INSPIRE Subjek: 3,415 pasien asma dewasa ≥16 thn dari 11 negara yang diresepkan ICS atau ICS+LABA Hasil: 74% masih menggunakan SABA setiap hari; 51% pasien memiliki asma yang tidak terkontrol; 21% pasien memiliki asma yang tidak terkontrol dengan baik; dan hanya 28% pasien yang diklasifikasikan memiliki asma yang terkontrol dengan baik. Partridge MR, et al. Attitudes and actions of asthma patients on regular maintenance therapy: the INSPIRE study. BMC Pulmonary Medicine 2006;6:13.

5
Studi AIRIAP II (Asthma Insights & Reality in Asia Pacific)
MSS v1c Symptom Control Index Base: All respondents, Respondents who answered ACT test (n=see brackets)
")
10
Stepwise management - pharmacotherapy
UPDATED! Diagnosis Symptom control & risk factors (including lung function) Inhaler technique & adherence Patient preference REVIEW RESPONSE ASSESS Symptoms Exacerbations Side-effects Patient satisfaction Lung function ADJUST TREATMENT Asthma medications Non-pharmacological strategies Treat modifiable risk factors STEP 5 STEP 4 STEP 3 *Not for children <12 years **For children 6-11 years, the preferred Step 3 treatment is medium dose ICS #For patients prescribed BDP/formoterol or BUD/ formoterol maintenance and reliever therapy Tiotropium by mist inhaler is an add-on treatment for patients ≥12 years with a history of exacerbations STEP 1 STEP 2 Refer for add-on treatment e.g. tiotropium,* omalizumab, mepolizumab* PREFERRED CONTROLLER CHOICE Med/high ICS/LABA Low dose ICS/LABA** Low dose ICS Other controller options Consider low dose ICS Leukotriene receptor antagonists (LTRA) Low dose theophylline* Med/high dose ICS Low dose ICS+LTRA (or + theoph*) Add tiotropium* High dose ICS + LTRA (or + theoph*) Add low dose OCS As-needed short-acting beta2-agonist (SABA) As-needed SABA or low dose ICS/formoterol# RELIEVER GINA 2016, Box 3-5 (2/8) (upper part)
 Inhaler technique & adherence. Patient preference. REVIEW RESPONSE. ASSESS. Symptoms. Exacerbations. Side-effects. Patient satisfaction. Lung function. ADJUST TREATMENT. Asthma medications. Non-pharmacological strategies. Treat modifiable risk factors. STEP 5. STEP 4. STEP 3. *Not for children <12 years. **For children 6-11 years, the preferred Step 3 treatment is medium dose ICS. #For patients prescribed BDP/formoterol or BUD/ formoterol maintenance and reliever therapy. Tiotropium by mist inhaler is an add-on treatment for patients ≥12 years with a history of exacerbations. STEP 1. STEP 2. Refer for add-on treatment. e.g. tiotropium,* omalizumab, mepolizumab* PREFERRED CONTROLLER CHOICE. Med/high ICS/LABA. Low dose ICS/LABA** Low dose ICS. Other controller options. Consider low dose ICS. Leukotriene receptor antagonists (LTRA) Low dose theophylline* Med/high dose ICS. Low dose ICS+LTRA. (or + theoph*) Add tiotropium* High dose ICS + LTRA (or + theoph*) Add low dose OCS. As-needed short-acting beta2-agonist (SABA) As-needed SABA or low dose ICS/formoterol# RELIEVER. GINA 2016, Box 3-5 (2/8) (upper part)")
11
PATOFISIOLOGI ASMA… Key components: (1) inflammation, (2) bronchial hyper-reactivity, (3) airway remodeling 1970’s ’s ’s present Bronchospasm Bronchospasm + Inflammation Bronchospasm + Inflammation + Remodeling Dendritic cells Th17 Symptoms Bronchial hyper-reactivity Fixed Obstruction Eosinophil IL-5 / IL-13 T cell Th-2 Relieve symptoms Prevent symptoms & attacks Prevent symptoms, attacks, & remodeling CHEST 2013; 144(3):1026–1032.
:1026–1032.")
12
INFLAMASI – REMODELING
Nature Reviews Immunology 2, (February 2002)
")
13
INFLAMASI – REMODELING…
Many cell include: Mast cell Eosinophil B lymphocyte T lymphocyte Macrophage Neutrophil Epithelial cell Dendritic Cell Many cytokine / chemokine released: IL4, IL5, IL8, IL9, IL13 Histamine Leukotriene © PDPI. Asma. 2006

14
Reseptor di Otot Polos Saluran Nafas
MEKANISME ASMA lipooksigenase siklooksigenase Alergen Respon Segera (Initial Phase) Sel dendritik Limfosit T Makrofag Interleukin Eosinofil Sel Mast Histamin Prostaglandin Leukotrien Bronkokonstriksi, Inflamasi Edema, Hipersekresi mukus Asma Faktor Aktivasi Platelet Respon Tertunda (Late Phase) 1 2 Reseptor di Otot Polos Saluran Nafas Asam Arakidonat Sumber : At a Glance Sistem Respirasi Edisi Kedua by Jeremy P.T Ward et al
 Sel dendritik. Limfosit T. Makrofag. Interleukin. Eosinofil. Sel Mast. Histamin. Prostaglandin. Leukotrien. Bronkokonstriksi, Inflamasi. Edema, Hipersekresi mukus. Asma. Faktor Aktivasi Platelet. Respon Tertunda (Late Phase) Reseptor di Otot Polos Saluran Nafas. Asam Arakidonat. Sumber : At a Glance Sistem Respirasi Edisi Kedua by Jeremy P.T Ward et al.")
16
ALASAN KONTROL ASMA BURUK The wrong diagnosis
Incorrect choice of inhaler, poor technique Smoking - Relative steroid resistance among smokers asthma Co-morbid Rhinitis Patients’ beliefs and adherence Individual variation in response to treatment Haughney J, Price D, Kaplan A, et al. Achieving asthma control in practice: understanding the reasons for poor control. Respir Med 2008;102:

17
B Sinha, et al 2015

18
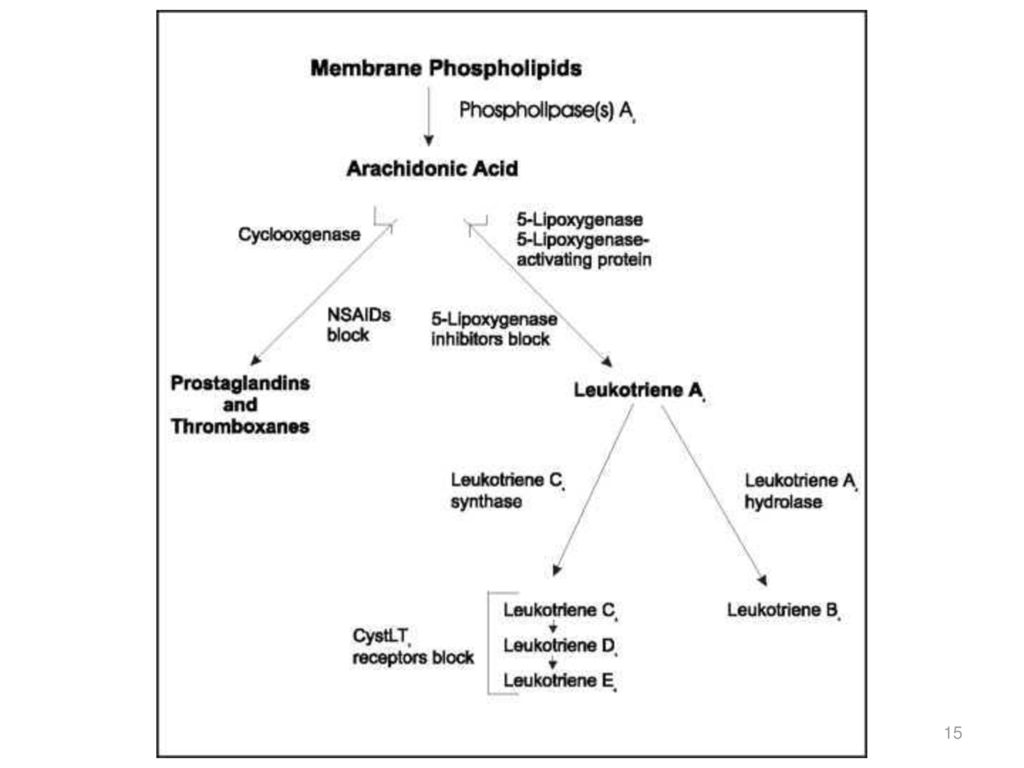
Perubahan Target Terapi: LEUKOTRIEN
Diproduksi oleh leukosit dan memiliki struktur tiga rantai ganda (triena) Mediator pro-inflamasi, hasil dari aktivasi sel-sel imun pada membran sel akibat adanya alergen Bila berikatan pada reseptor CysLT di otot polos saluran nafas kontraksi otot polos, menarik eosinofil, meningkatkan sekresi mukus, meningkatkan permeabilitas vaskuler proliferasi otot polos perubahan model saluran nafas (bronkokonstriksi, hipersekresi) Sintesis & pelepasan leukotrien tidak dihambat oleh kortikosteroid perlu anti-leukotrien / antagonis reseptor leukotrien (LTRA). Vora AC. Montelukast – place in therapy. Supplement to Journal of The Association of Physicians of India 2014(62):46-50. Benninger MS & Waters H. Montelukast: Pharmacology, safety, tolerability and efficacy. Therapeutics 2009(1):
 Mediator pro-inflamasi, hasil dari aktivasi sel-sel imun pada membran sel akibat adanya alergen. Bila berikatan pada reseptor CysLT di otot polos saluran nafas kontraksi otot polos, menarik eosinofil, meningkatkan sekresi mukus, meningkatkan permeabilitas vaskuler proliferasi otot polos perubahan model saluran nafas (bronkokonstriksi, hipersekresi) Sintesis & pelepasan leukotrien tidak dihambat oleh kortikosteroid perlu anti-leukotrien / antagonis reseptor leukotrien (LTRA). Vora AC. Montelukast – place in therapy. Supplement to Journal of The Association of Physicians of India 2014(62): Benninger MS & Waters H. Montelukast: Pharmacology, safety, tolerability and efficacy. Therapeutics 2009(1):")
19
MONTELUKAST Montelukast: LTRA paling poten dan spesifik
Sebagai pengontrol pada alergi, asma, maupun asma akibat olahraga (exercise-induced) Berikatan dengan kuat dan selektif pada reseptor CysLT1 untuk menghambat pengikatan leukotrien LTD4 antagonis leukotrien anti-inflamasi Aman & ditoleransi dengan baik tidak ada perbedaan bermakna dengan plasebo Vora AC. Montelukast – place in therapy. Supplement to Journal of The Association of Physicians of India 2014(62):46-50. Benninger MS & Waters H. Montelukast: Pharmacology, safety, tolerability and efficacy. Therapeutics 2009(1):
 Berikatan dengan kuat dan selektif pada reseptor CysLT1 untuk menghambat pengikatan leukotrien LTD4 antagonis leukotrien anti-inflamasi. Aman & ditoleransi dengan baik tidak ada perbedaan bermakna dengan plasebo. Vora AC. Montelukast – place in therapy. Supplement to Journal of The Association of Physicians of India 2014(62): Benninger MS & Waters H. Montelukast: Pharmacology, safety, tolerability and efficacy. Therapeutics 2009(1):")
20
MONTELUKAST – Studi MONICA
Subjek: ≥18thn dengan asma ringan-sedang diberikan MON 10 mg 1x1 sebagai add-on ICS atau ICS+LABA selama 6 bulan Hasil: Terjadi perbaikan klinis ketika montelukast ditambahkan pada terapi ICS atau ICS+LABA. Perbaikan tersebut mencakup kontrol asma, kualitas hidup, fungsi paru, serta status asma, dengan profil keamanan yang baik. Virchow JC, et al. Add-on montelukast in inadequately controlled asthma patients in a 6-month open-label study: the montelukast in chronic asthma (MONICA) study. Respiratory Medicine 2010;104:
 study. Respiratory Medicine 2010;104:")
21
Patients in Each ACT Category, %
Result Studi MONICA: Improvements in ACT Scores With Add-On Montelukast in ICS and ICS + LABA Subgroups 1/Virchow, p 988, C2, ¶4, L1-7; p 988, Table 1 p 991, C2, ¶4, L1-6 Graph: p 989, Fig D; p 988, Table 1 (N’s) (perm req) Bullet: p 988, Table 1 N numbers: Data on File/Source B (MONICA Final Report): p 31, Table 3.3.1C ACT Scores 25 (Completely controlled) 16–19 (Poorly controlled) –24 (Well controlled) <16 (Uncontrolled) 2.1 0.9 100 19.5 9.4 15.2 25.0 11.9 6.0 9.6 15.1 39.3 47.5 45.2 23.5 53.3 45.8 75 29.8 54.3 63.1 Patients in Each ACT Category, % 50 27.9 48.3 27.6 23.1 21.3 25 19.2 23.8 13.4 20.4 16.7 14.1 10.8 The slide shows the analysis of changes in ACT scores over 12 months in subgroups of patients treated with an ICS vs an ICS plus LABA before add-on montelukast. Mean ACT score was 15.9 in the ICS subgroup and 14.1 in the ICS plus LABA subgroup at baseline. Improvements were seen in both subgroups, but there were more well-controlled patients after add-on montelukast in the ICS subgroup (54.3%) vs the ICS plus LABA subgroup (45.8%). Mean ACT scores at Month 12 were 21.6 and 19.8 for the ICS and ICS plus LABA subgroups, respectively, reflecting least-square (LS) mean increases of 6.6 for ICS and 5.4 for ICS plus LABA.1 These data reflect improved asthma control that translated to clinically relevant benefits in the ACT score when montelukast was added in both the ICS and ICS plus LABA subgroups.1 6.5 Baseline (n=388) Month 3 (n=357) Month 6 (n=318) Month 12 (n=230) Baseline (n=1,163) Month 3 (n=1,035) Month 6 (n=911) Month 12 (n=622) ICS Subgroup ICS + LABA Subgroup ACT scores: LS mean ACT score improved from baseline to Month 12 of add-on montelukast by 6.6 in the ICS subgroup and 5.4 in the ICS + LABA subgroup. ICS or ICS + LABA at baseline; add-on montelukast at Months 3, 6, and 12 Virchow JC, et al. Add-on montelukast in inadequately controlled asthma patients in a 6-month open-label study: the montelukast in chronic asthma (MONICA) study. Respiratory Medicine 2010;104: 1. Virchow JC et al. J Asthma. 2010;47(9):986–993.
 (perm req) Bullet: p 988, Table 1. N numbers: Data on File/Source B (MONICA Final Report): p 31, Table 3.3.1C. ACT Scores. 25 (Completely controlled) 16–19 (Poorly controlled) 20–24 (Well controlled) <16 (Uncontrolled) Patients in Each ACT Category, % The slide shows the analysis of changes in ACT scores over 12 months in subgroups of patients treated with an ICS vs an ICS plus LABA before add-on montelukast. Mean ACT score was 15.9 in the ICS subgroup and 14.1 in the ICS plus LABA subgroup at baseline. Improvements were seen in both subgroups, but there were more well-controlled patients after add-on montelukast in the ICS subgroup (54.3%) vs the ICS plus LABA subgroup (45.8%). Mean ACT scores at Month 12 were 21.6 and 19.8 for the ICS and ICS plus LABA subgroups, respectively, reflecting least-square (LS) mean increases of 6.6 for ICS and 5.4 for ICS plus LABA.1. These data reflect improved asthma control that translated to clinically relevant benefits in the ACT score when montelukast was added in both the ICS and ICS plus LABA subgroups Baseline (n=388) Month 3 (n=357) Month 6 (n=318) Month 12 (n=230) Baseline (n=1,163) Month 3 (n=1,035) Month 6 (n=911) Month 12 (n=622) ICS Subgroup. ICS + LABA Subgroup. ACT scores: LS mean ACT score improved from baseline to Month 12 of add-on montelukast by 6.6 in the ICS subgroup and 5.4 in the ICS + LABA subgroup. ICS or ICS + LABA at baseline; add-on montelukast at Months 3, 6, and 12. Virchow JC, et al. Add-on montelukast in inadequately controlled asthma patients in a 6-month open-label study: the montelukast in chronic asthma (MONICA) study. Respiratory Medicine 2010;104: Virchow JC et al. J Asthma. 2010;47(9):986–993.")
22
Result Studi MONICA: Improvements in Mini AQLQ With Add-On Montelukast in ICS and ICS + LABA Subgroups 1/Virchow, p 990, Table 2; p 988, C2, ¶4, L10-13 p 990, Table 2 N numbers: Data on File/Source C (MONICA AQLQ Scores Table): p1A Baseline ICS Baseline ICS + LABA Montelukast + baseline therapy 7 5.90 6 5.53 5.32 5.43 5.11 4.86 5 4.18 3.80 4 Score 3 2 MiniAQLQ scores after 12 months of treatment with add-on montelukast were 5.90 in the subgroup of patients treated with an ICS and 5.43 in the subgroup treated with an ICS plus LABA. The mean difference from baseline to Month 12 was 1.51 for the ICS subgroup and 1.53 for the ICS plus LABA subgroup.1 1 Baseline (n=379) Month 3 (n=345) Month 6 (n=309) Month 12 (n=228) Baseline (n=1,137) Month 3 (n=983) Month 6 (n=883) Month 12 (n=613) ICS Subgroup ICS + LABA Subgroup Virchow JC, et al. Add-on montelukast in inadequately controlled asthma patients in a 6-month open-label study: the montelukast in chronic asthma (MONICA) study. Respiratory Medicine 2010;104: 1. Virchow JC et al. J Asthma. 2010;47(9):986–993.
: p1A. Baseline ICS. Baseline ICS + LABA. Montelukast + baseline therapy Score MiniAQLQ scores after 12 months of treatment with add-on montelukast were 5.90 in the subgroup of patients treated with an ICS and 5.43 in the subgroup treated with an ICS plus LABA. The mean difference from baseline to Month 12 was 1.51 for the ICS subgroup and 1.53 for the ICS plus LABA subgroup Baseline (n=379) Month 3 (n=345) Month 6 (n=309) Month 12 (n=228) Baseline (n=1,137) Month 3 (n=983) Month 6 (n=883) Month 12 (n=613) ICS Subgroup. ICS + LABA Subgroup. Virchow JC, et al. Add-on montelukast in inadequately controlled asthma patients in a 6-month open-label study: the montelukast in chronic asthma (MONICA) study. Respiratory Medicine 2010;104: Virchow JC et al. J Asthma. 2010;47(9):986–993.")
23
Improvements in Lung Function With Add-On Montelukast
Result Studi MONICA: Improvements in Lung Function With Add-On Montelukast 1/Virchow, p 646, C1, ¶1, L9-11; p 648, Table 3 (FEV and PEF + footnote (P value) p 648, Table 3 (FEV & PEF values) + footnote (P value) Footnote: p 646, C1, ¶1, L9-11 ICS or ICS + LABA Montelukast + baseline therapy 3 7 2.61a Month 3 (n=1,057) 6.20a Month 3 (n=669) 2.60a Month 6 (n=914) 6.22a Month 6 (n=563) 2.46 Baseline (n=1,445) 5.76 Baseline (n=967) 6 Lung function measurements were performed at the investigator’s discretion; thus, not all patients had data for these parameters. Both mean FEV1 values and mean PEF values improved significantly from baseline with an ICS or an ICS plus LABA at Months 3 and 6 of add-on montelukast (P< for all comparisons).1 5 2 4 FEV1, L PEF, L/s 3 1 2 1 aP< vs baseline. Lung function measurements were performed at the investigator’s discretion; thus, not all patients had data for these parameters. Virchow JC, et al. Add-on montelukast in inadequately controlled asthma patients in a 6-month open-label study: the montelukast in chronic asthma (MONICA) study. Respiratory Medicine 2010;104: 1. Virchow JC et al. Respir Med. 2010;104:644–651.
 p 648, Table 3 (FEV & PEF values) + footnote (P value) Footnote: p 646, C1, ¶1, L9-11. ICS or ICS + LABA. Montelukast + baseline therapy a. Month 3 (n=1,057) 6.20a. Month 3 (n=669) 2.60a. Month 6 (n=914) 6.22a. Month 6 (n=563) Baseline (n=1,445) Baseline (n=967) 6. Lung function measurements were performed at the investigator’s discretion; thus, not all patients had data for these parameters. Both mean FEV1 values and mean PEF values improved significantly from baseline with an ICS or an ICS plus LABA at Months 3 and 6 of add-on montelukast (P< for all comparisons) FEV1, L. PEF, L/s aP< vs baseline. Lung function measurements were performed at the investigator’s discretion; thus, not all patients had data for these parameters. Virchow JC, et al. Add-on montelukast in inadequately controlled asthma patients in a 6-month open-label study: the montelukast in chronic asthma (MONICA) study. Respiratory Medicine 2010;104: Virchow JC et al. Respir Med. 2010;104:644–651.")
24
MONTELUKAST – GINA Montelukast menghasilkan onset yang cepat, meningkatkan fungsi paru, mengurangi gejala, mengurangi frekuensi serangan, meningkatkan kualitas hidup. *Not for children <12 years. **For children 6–11 years, the preferred Step 3 treatment is medium dose ICS. # Low dose ICS/formoterol is the reliever medication for patients prescribed low dose budesonide/formoterol or low dose beclometasone/formoterol for maintenance and reliever therapy. +Tiotropium by mist inhaler is an add-on treatment for patients with a history of exacerbations*. Other controller options RELIEVER STEP 1 STEP 2 STEP 3 STEP 4 STEP 5 Low dose ICS Consider low dose ICS Leukotriene receptor antagonists (LTRA) Low dose theophylline* Med/high dose ICS Low dose ICS+LTRA (or + theoph*) As-needed short-acting beta2-agonist (SABA) Low dose ICS/LABA** Med/high ICS/LABA Refer for add-on treatment e.g. tiotropium,*+ omalizumab, mepolizumab* PREFERRED CONTROLLER CHOICE Add tiotropium# High dose ICS + LTRA (or + theoph*) Add low dose OCS As-needed SABA or low dose ICS/formoterol# Jarvis B & Markham A. Montelukast, a review of its therapeutic potential in persistent asthma. Drugs 2000;59(4): GINA 2016.
 Low dose theophylline* Med/high dose ICS. Low dose ICS+LTRA. (or + theoph*) As-needed short-acting beta2-agonist (SABA) Low dose ICS/LABA** Med/high ICS/LABA. Refer for add-on treatment. e.g. tiotropium,*+ omalizumab, mepolizumab* PREFERRED CONTROLLER CHOICE. Add tiotropium# High dose ICS + LTRA (or + theoph*) Add low dose OCS. As-needed SABA or low dose ICS/formoterol# Jarvis B & Markham A. Montelukast, a review of its therapeutic potential in persistent asthma. Drugs 2000;59(4): GINA")
25
MONTELUKAST – Kombinasi
Purpose: There have been few reports regarding the efficacy of antiasthmatics in older patients. To compare the efficacy of the addition of montelukast to low-dose inhaled budesonide (MON-400BUD) versus increasing the dose of inhaled steroid (800BUD) on asthma control in older asthmatics. Method: A randomized, open-label, parallel-designed trial was conducted for 12 weeks. The primary endpoint was the rate of patients who reached “well-controlled asthma status” after the 12-week treatment period. Additionally, asthma exacerbations, sputum inflammatory cells, asthma control test (ACT) and physical functioning scale (PFS), and adverse reactions were monitored. 60-75 YO diagnosed 6 month with asthma Budesonide 400ug or budesonide 250ug with LABA Run in 400ug budesonide then randomized to 800ug budesonide 400ug budesonide + montelukast 10 mg
 versus increasing the dose of inhaled steroid (800BUD) on asthma control in older asthmatics. Method: A randomized, open-label, parallel-designed trial was conducted for 12 weeks. The primary endpoint was the rate of patients who reached well-controlled asthma status after the 12-week treatment period. Additionally, asthma exacerbations, sputum inflammatory cells, asthma control test (ACT) and physical functioning scale (PFS), and adverse reactions were monitored YO diagnosed 6 month with asthma. Budesonide 400ug or budesonide 250ug with LABA. Run in 400ug budesonide then randomized to. 800ug budesonide. 400ug budesonide + montelukast 10 mg.")
26
HASIL A previous multinational survey indicated that an ACT score <20 predicted poorly controlled asthma in 94% of cases.

27
HASIL… Conclusion: The efficacy of 12-week treatment with MON-400BUD in older asthmatics was comparable to that of 800BUD on asthma control but associated with reduced frequency of asthma exacerbations requiring oral steroids and sore throat events. Changes in ACT and PFS can be useful predictors of asthma control status in older patients.

28
MONTELUKAST – EIB Pemberian kombinasi SABA dan Leukotrien Antagonis sebelum berolahraga sangat direkomendasikan pada pasien yang memiliki resiko EIB

29
SUMMARY Studi INSPIRE & AIRIAP menunjukkan bahwa terapi terkini belum mengontrol asma dengan optimal. Reaksi asma melibatkan peranan mediator pro-inflamasi leukotrien yang tidak bisa dihambat dengan terapi kortikosteroid, sehingga dibutuhkan antagonis reseptor leukotrien (LTRA), seperti montelukast. LTRA direkomendasikan dalam guideline GINA. Dari uji klinis, montelukast efektif digunakan sebagai monoterapi maupun kombinasi, dengan profil keamanan setara dengan plasebo pada dewasa maupun pediatri. MONARIN mengandung LTRA montelukast sebagai anti-inflamasi pada kasus asma dengan/tanpa rinitis.
, seperti montelukast. LTRA direkomendasikan dalam guideline GINA. Dari uji klinis, montelukast efektif digunakan sebagai monoterapi maupun kombinasi, dengan profil keamanan setara dengan plasebo pada dewasa maupun pediatri. MONARIN mengandung LTRA montelukast sebagai anti-inflamasi pada kasus asma dengan/tanpa rinitis.")
30
TERIMA KASIH

Presentasi serupa












>")






