Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
Dr. Budi Arief Waskito, SpJP FIHA
HIPERTENSI Dr. Budi Arief Waskito, SpJP FIHA

3
Tekanan Darah Tekanan Darah ditentukan oleh 2 faktor
Cardiac output (CO): Jumlah darah yang dipompa keluar dari jantung per menit CO = HR X SV Peripheral resistance (PR): Resistensi atau kekuatan arteriol melawan aliran darah (komponen utamanya adalah vasokonstriksi) BP = CO X PR Learning Outcomes 26.1 Describe the major physiological factors that regulate blood pressure. 26.2 Understand the role of the kidneys and renin angiotensin- aldosterone system in blood pressure regulation. Blood pressure is mainly determined by two factors: cardiac output (CO) and peripheral resistance (PR). Cardiac output (CO) is the amount of blood that is pumped out of the heart per minute. Two factors determine cardiac output: the heart rate (HR) in beats per minute and the stroke volume (SV), the amount of blood pumped per beat. The peripheral resistance (PR) is the resistance or friction that the arterioles have against the flow of blood. The main factor that increases the peripheral resistance is vasoconstriction. A number of factors have been shown to affect BP. While these factors are not believed to be the cause of hypertension, controlling these factors can produce modest decreases in BP. These factors include sodium restriction, weight loss, elimination of smoking, regular physical exercise, and various relaxation techniques aimed at reducing stress. If renal blood flow is reduced, the enzyme renin is released by the kidneys into the bloodstream. Release of renin activates the renin-angiotensin-aldosterone (RAA) mechanism. Activation of the RAA mechanism causes vasoconstriction, and sodium and water retention, which increases blood pressure.
: Jumlah darah yang dipompa keluar dari jantung per menit. CO = HR X SV. Peripheral resistance (PR): Resistensi atau kekuatan arteriol melawan aliran darah (komponen utamanya adalah vasokonstriksi) BP = CO X PR. Learning Outcomes Describe the major physiological factors that regulate blood pressure Understand the role of the kidneys and renin angiotensin- aldosterone system in blood pressure regulation. Blood pressure is mainly determined by two factors: cardiac output (CO) and peripheral resistance (PR). Cardiac output (CO) is the amount of blood that is pumped out of the heart per minute. Two factors determine cardiac output: the heart rate (HR) in beats per minute and the stroke volume (SV), the amount of blood pumped per beat. The peripheral resistance (PR) is the resistance or friction that the arterioles have against the flow of blood. The main factor that increases the peripheral resistance is vasoconstriction. A number of factors have been shown to affect BP. While these factors are not believed to be the cause of hypertension, controlling these factors can produce modest decreases in BP. These factors include sodium restriction, weight loss, elimination of smoking, regular physical exercise, and various relaxation techniques aimed at reducing stress. If renal blood flow is reduced, the enzyme renin is released by the kidneys into the bloodstream. Release of renin activates the renin-angiotensin-aldosterone (RAA) mechanism. Activation of the RAA mechanism causes vasoconstriction, and sodium and water retention, which increases blood pressure.")
4
Batasan Tekanan darah sistolik lebih atau sama dengan 140 mmHg dan tekanan darah diastolik lebih atau sama dengan 90 mmHg, pada individu tanpa menggunakan obat anti HT

5
Definisi & klasifikasi Tekanan Darah (WHO – ISH 1999)
Kategori Sistolik (mmHg) Diastolik (mmHg) Optimal < 120 < 80 Normal < 130 < 85 Normal tinggi 130 – 139 85 – 89 HT derajat 1 / ringan 140 – 159 90 – 99 HT derajat 2 / sedang 160 – 179 100 – 109 HT derajat 3 / berat ≥ 180 ≥ 110
 Diastolik (mmHg) Optimal. < 120. < 80. Normal. < 130. < 85. Normal tinggi. 130 – – 89. HT derajat 1 / ringan. 140 – – 99. HT derajat 2 / sedang. 160 – – 109. HT derajat 3 / berat. ≥ 180. ≥ 110.")
6
JNC 7 Blood Pressure (BP) Classification
Diastolic BP, mm Hg BP Classification Systolic BP, mm Hg* Lifestyle Modification Normal <120 and <80 Encourage Prehypertension or Yes Stage 1 hypertension or Yes Stage 2 hypertension ≥160 or ≥100 Yes The seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) provides new guidelines for prevention and management of this highly prevalent disease. JNC 7 classifies blood pressure (BP) as follows: systolic BP (SBP) of mm Hg or a diastolic BP (DBP) of mm Hg is considered prehypertension; SBP/DBP or 90-99 mm Hg indicates stage 1 hypertension; SBP 160 mm Hg or DBP 100 mm Hg denotes stage 2 hypertension, which requires health-promoting lifestyle modifications to prevent CVD. JNC 7 = seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. *Classification for ages 18 years and older. JNC 7. JAMA ;289:
 provides new guidelines for prevention and management of this highly prevalent disease. JNC 7 classifies blood pressure (BP) as follows: systolic BP (SBP) of mm Hg or a diastolic BP (DBP) of mm Hg is considered prehypertension; SBP/DBP or 90-99 mm Hg indicates stage 1 hypertension; SBP 160 mm Hg or DBP 100 mm Hg denotes stage 2 hypertension, which requires health-promoting lifestyle modifications to prevent CVD. JNC 7 = seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. *Classification for ages 18 years and older. JNC 7. JAMA. 2003;289:")
7
Etiologi HT Hipertensi esensial atau primer Hipertensi sekunder

8
1. Hipertensi esensial / primer
Tidak jelas penyebabnya (multifaktor) 95% kasus
 95% kasus.")
9
2. Hipertensi sekunder 5% kasus Macam : Gagal ginjal kronik
Peny. Renovaskuler Coartasio aorta Aldosteronisme primer Cushing’s syndrome Pheochromocytoma

10
Pemeriksaan pada Hipertensi
Anamnesa Pemeriksaan fisik Pemeriksaan laboratorium Pemeriksaan tambahan

11
Anamnesa Lama dan klasifikasi HT Pola hidup
Faktor resiko peny. Kardiovaskuler Keluhan Pemakaian obat yang meningkatkan TD

12
Faktor risiko peny. Kardiovaskuler
HT Merokok Dislipidemia Umur (> 55 th) Riwayat keluarga peny. Kardiovaskuler Obesitas Kurang olahraga Diabetes
 Riwayat keluarga peny. Kardiovaskuler. Obesitas. Kurang olahraga. Diabetes.")
13
Keluhan Sering sakit kepala, terutama bagian belakang kepala
Keluhan cardio : berdebar, dada terasa berat, sesak Keluhan lain : sulit tidur, migrain, mudah marah Sering tanpa keluhan

14
Obat yang meningkatkan TD
Kortikosteroid Obat flu (dekongestan, mis efedrin) Kontrasepsi oral NSAID Simpatomimetik Antidepresan
 Kontrasepsi oral. NSAID. Simpatomimetik. Antidepresan.")
15
Pemeriksaan fisik Pengukuran TD pada 2-3 x kunjungan, posisi terlentang, duduk dan berdiri, pada lengan kanan dan kiri Pemeriksaan TB & BB Pemeriksaan jantung : pembesaran, gallop, murmur dll Pemeriksaan leher, abdomen, extremitas Pemeriksaan reflex saraf

16
Pemeriksaan Sebaiknya periksa TD pada kedua lengan Fundus okuli
Menghitung BMI (perlu juga mengukur lingkar perut) Auskultasi bruit arteri karotis, abdominalis, dan femoralis Palpasi kelenjar tiroid
 Auskultasi bruit arteri karotis, abdominalis, dan femoralis. Palpasi kelenjar tiroid.")
17
Pemeriksaan (lanjutan)
Pemeriksaan jantung dan paru Pemeriksaan Abdomen: pembesaran ginjal, massa, dan pulsasi aorta yang abnormal Ekstremitas bawah: edema dan pulsasi Pemeriksaan Neurologis

18
Pemeriksaan laboratorium
Darah lengkap Urinalisis Fungsi ginjal : BUN, SC Gula darah : BSN, 2 JPP Profil lemak : cholesterol, trigliserida, HDL, LDL Elektrolit : K / Na Asam urat

19
Pemeriksaan tambahan Funduscopy, untuk mencari retinopati kw I – IV
EKG, untuk mengetahui adanya : Hipertrofi ventrikel kiri Iskemi Infark miokard Thorax foto, untuk melihat : Cardiomegali / configurasi HT Congestif / edema paru Echocardiografi

20
Penatalaksanaan Non farmakologis Farmakologis

21
JNC 7: Considerations for Special Populations
Treatment generally similar for all demographic groups Socioeconomic factors and lifestyle important barriers to BP control Prevalence, severity of hypertension increased in blacks The treatment of hypertension is generally similar across all demographic groups. Socioeconomic factors and lifestyle are important barriers to BP control in minority populations. The prevalence, severity, and impact of hypertension are increased in blacks, who also demonstrate a reduced BP response to certain types of antihypertensive monotherapy. JNC 7. JAMA. 2003;289:

22
Non Farmakologis Menurunkan berat badan Olahraga teratur
Mengurangi asupan garam (< 6 gram /hari) Mengurangi asupan lemak / kolesterol Menghindari rokok, alkohol Relaxasi Mengurangi stres psikososial
 Mengurangi asupan lemak / kolesterol. Menghindari rokok, alkohol. Relaxasi. Mengurangi stres psikososial.")
23
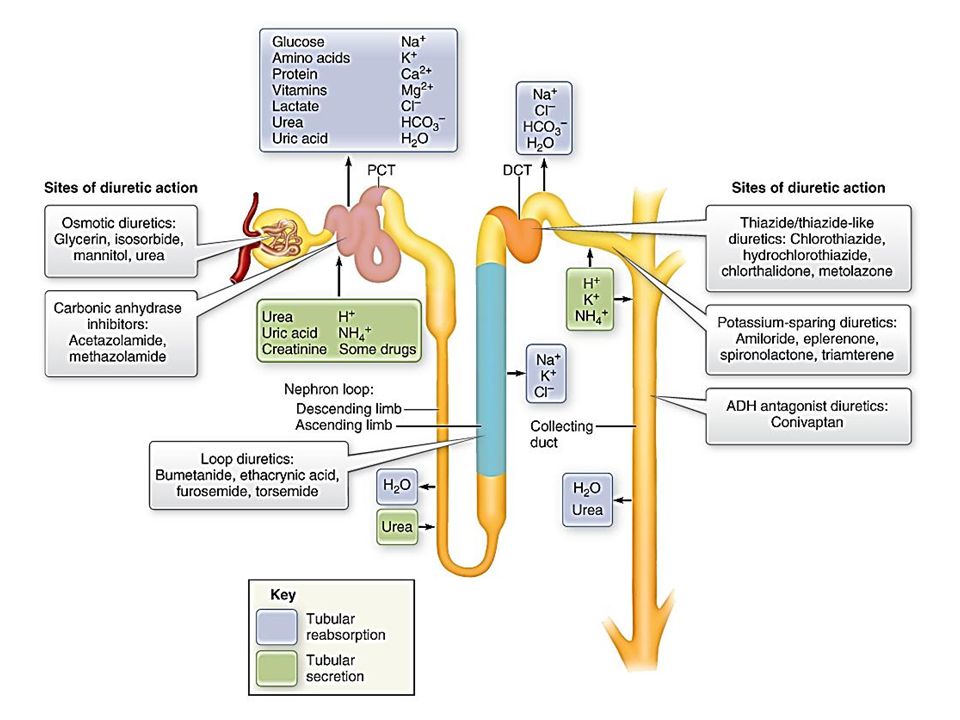
Farmakologis Diuretika Betabloker Kalsium antagonis ACE inhibitor
Angiotensin-2 reseptor bloker Alfa bloker Alfa-2 agonis

24
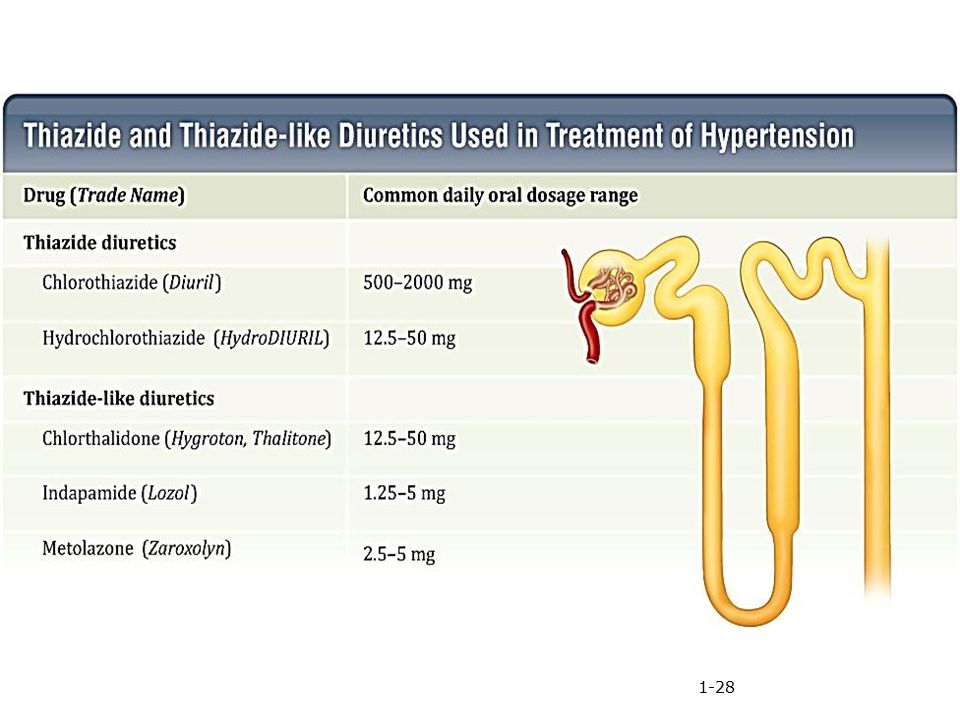
Diuretika Mulai Dosis kecil Efektif, sekali pemberian / hari
Menurunkan kadar Na+ Macam : HCT, dosis 6,25 – 50 mg / hari Chlorthalidon, dosis 12,5 – 50 mg / hari Indapamide, dosis 1,25 – 5 mg / hari

25
Diuretik Ekskresi sodium TD Obat tunggal untuk hipertensi ringan
Efek vasodilatasi timbul setelah beberapa minggu Pada hipertensi sedang-berat, kombinasi diuretik dengan obat hipertensi lainnya Learning Outcomes 26.3 Explain the antihypertensive actions of thiazide and loop diuretics. The diuretics, which increase the excretion of sodium from the kidneys, have been shown to lower blood pressure. Both salt restriction and diuretic therapy are effective measures to reduce BP. The hypotensive effect of these drugs is initially caused by increased excretion of sodium and water, which reduces blood volume and cardiac output. The antihypertensive effect of thiazide and thiazide-like diuretics occurs at low dosages. Higher diuretic dosages do increase urine output but do not result in greater decreases in peripheral resistance. Diuretics are used alone in mild hypertension. Usually several weeks of treatment are required for the vasodilating effect to fully develop. In moderate or severe hypertension, the diuretics are combined with other antihypertensive drugs.

26
Diuretik Diuretik yang digunakan untuk terapi hipertensi adalah thiazide dan thiazide like diuretic. Efek hipotensinya disebabkan karena peningkatan ekskresi sodium dan cairan, sehingga menurunkan volume darah dan cardiac output. Kontraindikasi: Gout, karena mempengaruhi ekskresi asam urat

29
Vasodilator Bekerja pada otot polos vaskuler, menyebabkan relaksasi sehingga terjadi vasodilatasi Biasanya digunakan kombinasi dengan diuretik dan beta-bloker, karena efek samping vasodilator: Retensi cairan, nausea, sakit kepala, hipotensi, dan refleks takikardi Learning Outcomes 26.5 Describe the mechanism of action of the vasodilator drugs. The vasodilator drugs act directly on vascular smooth muscle to cause relaxation. This results in vasodilation and a reduction in BP. Vasodilators are often used in combination with diuretics and beta-blockers. This is necessary because vasodilators often cause fluid retention and reflex tachycardia. Hydralazine is an arteriolar dilator used in moderate to severe hypertension in combination with both diuretics and beta-blockers (triple therapy). The main adverse effects are nausea, headache, hypotension, and reflex tachycardia. Long-term use may produce rheumatoid arthritis or a systemic lupus erythematosus–like syndrome. Minoxidil is a more potent arteriolar dilator than hydralazine, and it is indicated for patients who do not respond to triple therapy with other drug combinations. Minoxidil has the potential to produce a number of serious adverse effects, including myocardial ischemia and pericardial effusion. The primary action of calcium channel blockers in the treatment of hypertension is arteriolar vasodilation. This lowers peripheral resistance and blood pressure. These drugs are indicated for the treatment of hypertension and patients with CAD, particularly the variant or Prinzmetal form of angina pectoris.
. The main adverse effects are nausea, headache, hypotension, and reflex tachycardia. Long-term use may produce rheumatoid arthritis or a systemic lupus erythematosus–like syndrome. Minoxidil is a more potent arteriolar dilator than hydralazine, and it is indicated for patients who do not respond to triple therapy with other drug combinations. Minoxidil has the potential to produce a number of serious adverse effects, including myocardial ischemia and pericardial effusion. The primary action of calcium channel blockers in the treatment of hypertension is arteriolar vasodilation. This lowers peripheral resistance and blood pressure. These drugs are indicated for the treatment of hypertension and patients with CAD, particularly the variant or Prinzmetal form of angina pectoris.")
30
Vasodilator Calcium channel blockers efeknya adalah vasodilatasi arteriolar Mempengaruhi influx kalsium pada jantung & otot polos vaskuler menyebabkan depolarisasi lambat pada AV & SA node di jantung, menurunkan kontraktilitas otot jantung, relaksasi otot polos & vasodilatasi Verapamil dan Diltiazem efeknya langsung pada jantung

31
Vasodilators Learning Outcomes
26.5 Describe the mechanism of action of the vasodilator drugs. The vasodilator drugs act directly on vascular smooth muscle to cause relaxation. This results in vasodilation and a reduction in BP. Vasodilators are often used in combination with diuretics and beta-blockers. This is necessary because vasodilators often cause fluid retention and reflex tachycardia. Hydralazine is an arteriolar dilator used in moderate to severe hypertension in combination with both diuretics and beta-blockers (triple therapy). The main adverse effects are nausea, headache, hypotension, and reflex tachycardia. Long-term use may produce rheumatoid arthritis or a systemic lupus erythematosus–like syndrome. Minoxidil is a more potent arteriolar dilator than hydralazine, and it is indicated for patients who do not respond to triple therapy with other drug combinations. Minoxidil has the potential to produce a number of serious adverse effects, including myocardial ischemia and pericardial effusion. The primary action of calcium channel blockers in the treatment of hypertension is arteriolar vasodilation. This lowers peripheral resistance and blood pressure. These drugs are indicated for the treatment of hypertension and patients with CAD, particularly the variant or Prinzmetal form of angina pectoris.
. The main adverse effects are nausea, headache, hypotension, and reflex tachycardia. Long-term use may produce rheumatoid arthritis or a systemic lupus erythematosus–like syndrome. Minoxidil is a more potent arteriolar dilator than hydralazine, and it is indicated for patients who do not respond to triple therapy with other drug combinations. Minoxidil has the potential to produce a number of serious adverse effects, including myocardial ischemia and pericardial effusion. The primary action of calcium channel blockers in the treatment of hypertension is arteriolar vasodilation. This lowers peripheral resistance and blood pressure. These drugs are indicated for the treatment of hypertension and patients with CAD, particularly the variant or Prinzmetal form of angina pectoris.")
32
Kalsium antagonis Menurunkan tahanan perifer
Meningkatkan aliran darah ke ginjal Tidak mempengaruhi RAA sistem Macam : Nifedipin, dosis 3 x 5 – 10 mg / hari Amlodipin, dosis 1 x 2,5 – 10 mg / hari Diltiazem, dosis 3 x 30 – 60 mg / hari Verapamil, dosis 2 x 40 – 80 mg / hari

33
Obat yang menurunkan aktivitas Angiotensin
Renin inhibitors: Inhibisi aktivitas enzimatik renin ACE inhibitors: Inhibisi pembentukan angiotensin II Menurunkan rilis aldosterone dan hormon antidiuretik ARBs: Mem-blok reseptor angiotensin II

35
Renin Inhibitor Obat baru Aliskiren (Tekturna)
Menurunkan konversi Angiotensinogen menjadi Angiotensin I

36
Angiotensin Converting Enzyme Inhibitor
Angiotensin converting enzyme dirilis oleh paru Inhibisi konversi Angiotensin I menjadi Angiotensin II Menyebabkan penurunan rilis aldosterone dan ADH

37
ACE inhibitor Vasodilator Meningkatkan fungsi jantung Renoprotektif
Macam : Captopril, dosis 3 x 12,5 – 50 mg /hari Lisinopril, dosis 1 – 2 x 5 – 10 mg /hari Ramipril, dosis 1 x 2,5 – 10 mg /hari

38
Angiotensin Receptor Blockers
Angiotensin receptor blockers (ARBs) Berikatan dengan reseptor AT 1 dan mengantagonis efek angiotensin II secara kompetitif Aktivitas inhibisi ini merupakan mekanisme RAA yang menyebabkan vasodilatasi dan meningkatkan ekskresi sodium dan cairan Efeknya sama dengan ACEI
 Berikatan dengan reseptor AT 1 dan mengantagonis efek angiotensin II secara kompetitif. Aktivitas inhibisi ini merupakan mekanisme RAA yang menyebabkan vasodilatasi dan meningkatkan ekskresi sodium dan cairan. Efeknya sama dengan ACEI.")
39
Aktivitas Simpatis Pada hipertensi sering terjadi peningkatan aktivitas simpatis NE dan EPI menstimulasi reseptor alpha-1 dan beta-1, menyebabkan vasokonstriksi dan meningkatkan cardiac output. Learning Outcomes 26.4 Compare the pharmacologic actions of the different classes of drugs that reduce sympathetic nervous system activity. The sympathetic division of the autonomic nervous system has a vital function in the control of blood pressure. In hypertension there is often increased sympathetic activation. The adrenergic neurotransmitters norepinephrine and epinephrine stimulate alpha-1 and beta-1 receptors to cause vasoconstriction and increased cardiac output. Alpha-blockers, beta-blockers, adrenergic neuronal blockers, and drugs that act on the vasomotor center in the brain reduce sympathetic activity and lower BP.

40
Alpha-1 blockers Memblok reseptor pada otot polos vaskuler
Vasodilatasi dan menurunkan resistensi perifer Doxazosin, Prazosin, Terazosin Learning Outcomes 26.4 Compare the pharmacologic actions of the different classes of drugs that reduce sympathetic nervous system activity. The alpha-blockers doxazosin, prazosin, and terazosin selectively block the alpha-1 receptors located on vascular smooth muscle. The main antihypertensive effects are vasodilation and decreased peripheral resistance. The beta-blockers produce two actions that are of benefit in the treatment of hypertension. First, they block beta-1 receptors in the heart, lowering blood pressure by decreasing CO, especially when there is increased sympathetic activity. Second, they block the release of renin from the kidneys, which reduces activation of the renin-angiotensin-aldosterone (RAA) mechanism. Guanethidine and guanadrel are adrenergic neuronal blockers that cause a significant inhibition of sympathetic activity. First, these drugs prevent the release of NE from adrenergic nerve endings. Second, they deplete the storage vesicles of NE. Adrenergic neuronal blockers are only indicated for the treatment of severe hypertension that is unresponsive to other preferred drugs.
 mechanism. Guanethidine and guanadrel are adrenergic neuronal blockers that cause a significant inhibition of sympathetic activity. First, these drugs prevent the release of NE from adrenergic nerve endings. Second, they deplete the storage vesicles of NE. Adrenergic neuronal blockers are only indicated for the treatment of severe hypertension that is unresponsive to other preferred drugs.")
41
Alfa bloker Terutama untuk menurunkan tekanan darah diastolik
Sering dikombinasi dengan diuretik / betabloker Macam : Prasosin, dosis 1 – 3 x 1 – 4 mg / hari Doksasosin, dosis 1 x 1 – 6 mg / hari Terazosin, dosis 1 x 1 – 6 mg / hari

42
Beta bloker Menurunkan aktifitas simpatis
Kardioprotektif dan antiangina Macam : Propranolol, dosis 2 x 20 – 40 mg / hari Atenolol, dosis 1 x 25 – 100 mg / hari Bisoprolol, dosis 1 x 5 – 10 mg / hari dll

43
Obat yang efeknya pada Simpatolitik sentral
Bekerja langsung pada SSP untuk menurunkan tekanan darah Clonidine: (methyldopa, guanabenz, guanfacine) Menstimulasi inhibisi reseptor alfa-2 Menurunkan aktivitas saraf pada jantung, ginjal, dan pembuluh darah Menurunkan tekanan darah Efek samping: mulut kering, konstipasi, dan mengantuk Bila dihentikan mendadak akan timbul gejala putus obat (Withdrawal), jadi harus tapering Learning Outcomes 26.4 Compare the pharmacologic actions of the different classes of drugs that reduce sympathetic nervous system activity. There are several drugs that decrease sympathetic activity and BP by an action in the central nervous system. These drugs include clonidine (Catapres), guanabenz (Wytensin), guanfacine (Tenex), and methyldopa (Aldomet). Clonidine is the preferred drug of this group and will be used to describe the actions of this drug class. Clonidine is a centrally acting drug used in the treatment of hypertension. The main action of clonidine is exerted on the vasomotor center located in the medulla oblongata. Clonidine and the other centrally acting drugs stimulate inhibitory alpha-2 receptors. This reduces the activity of the sympathetic nerves that travel from the vasomotor center to the heart (decrease heart rate and cardiac output), kidneys (decrease release of renin), and blood vessels (vasodilation), resulting in a reduction of blood pressure. The adverse effects of clonidine include dry mouth, constipation, and drowsiness. If clonidine is abruptly discontinued, a withdrawal reaction may occur, with patients experiencing rebound sympathetic activity and hypertensive crisis. To avoid withdrawal symptoms of clonidine, the dose should be reduced gradually over a 2-week period.
 Menstimulasi inhibisi reseptor alfa-2. Menurunkan aktivitas saraf pada jantung, ginjal, dan pembuluh darah. Menurunkan tekanan darah. Efek samping: mulut kering, konstipasi, dan mengantuk. Bila dihentikan mendadak akan timbul gejala putus obat (Withdrawal), jadi harus tapering. Learning Outcomes Compare the pharmacologic actions of the different classes of drugs that reduce sympathetic nervous system activity. There are several drugs that decrease sympathetic activity and BP by an action in the central nervous system. These drugs include clonidine (Catapres), guanabenz (Wytensin), guanfacine (Tenex), and methyldopa (Aldomet). Clonidine is the preferred drug of this group and will be used to describe the actions of this drug class. Clonidine is a centrally acting drug used in the treatment of hypertension. The main action of clonidine is exerted on the vasomotor center located in the medulla oblongata. Clonidine and the other centrally acting drugs stimulate inhibitory alpha-2 receptors. This reduces the activity of the sympathetic nerves that travel from the vasomotor center to the heart (decrease heart rate and cardiac output), kidneys (decrease release of renin), and blood vessels (vasodilation), resulting in a reduction of blood pressure. The adverse effects of clonidine include dry mouth, constipation, and drowsiness. If clonidine is abruptly discontinued, a withdrawal reaction may occur, with patients experiencing rebound sympathetic activity and hypertensive crisis. To avoid withdrawal symptoms of clonidine, the dose should be reduced gradually over a 2-week period.")
44
Alfa 2 agonis Bekerja di sentral Menghambat aktifitas eferen simpatis
Macam : Clonidin, dosis 1 – 2 x 0,1 – 0,8 mg / hari Metildopa, dosis 2 x 125 – 250 mg / hari Untuk HT pada kehamilan

45
JNC 7 Express. NIH publication No 03-5233. http://www. nhlbi. nih
JNC 7 Express. NIH publication No May, 2003.

46
JNC 7 Recommends Lower BP Goals for Patients at Higher Risk for CVD
For the general population, BP goal remains unchanged (<140/90 mm Hg) Patient type Goal Patients with diabetes <130/80 mm Hg Patients with chronic kidney disease JNC 7 provides new guidelines for prevention and management of hypertension. The BP goal for individuals without substantial comorbidity is <140/90 mm Hg. Patients with diabetes or chronic renal failure should aim for a BP <130/80 mm Hg. JNC 7. JAMA. 2003;289:
 Patient type. Goal. Patients with diabetes. <130/80 mm Hg. Patients with chronic kidney disease. JNC 7 provides new guidelines for prevention and management of hypertension. The BP goal for individuals without substantial comorbidity is <140/90 mm Hg. Patients with diabetes or chronic renal failure should aim for a BP <130/80 mm Hg. JNC 7. JAMA. 2003;289:")
47
Algoritma terapi Hipertensi
Lifestyle Modifications Not at Goal BP Initial Drug Choices Stage 2 HTN 2-drug combination for most (usually thiazide-type diuretic & ACEI, or ARB, or BB, or CCB) Stage 1 HTN Thiazide-type diuretics for most. May consider ACEI, ARB, BB, CCB, or combination. Without Compelling Indications Drug(s) for the compelling indications Other antihypertensive drugs (diuretics, ACEI, ARB, BB, CCB) With Compelling Indications Not at Goal BP Optimize dosages or add additional drugs until goal BP is achieved. Consider consultation with hypertension specialist.
 Stage 1 HTN Thiazide-type diuretics for most. May consider ACEI, ARB, BB, CCB, or combination. Without Compelling Indications. Drug(s) for the compelling indications. Other antihypertensive drugs (diuretics, ACEI, ARB, BB, CCB) With Compelling Indications. Not at Goal BP. Optimize dosages or add additional drugs until goal BP is achieved. Consider consultation with hypertension specialist.")
48
Algoritma terapi (lanjutan)
Initial Drug Choices Not at Goal Blood Pressure (< 140/90 mm Hg) No response or troublesome side effects Inadequate response but well tolerated Substitute drug from different class Add second agent from different class (diuretic if not already used)
 No response or troublesome side effects. Inadequate response but well tolerated. Substitute drug from different class. Add second agent from different class (diuretic if not already used)")
49
Identifikasi penyebab Hipertensi
Sleep apnea Obat CKD Primary aldosteronism Penyakit Renovascular Penggunaan steroid kronis Cushing’s syndrome Pheochromocytoma Coarctation of the aorta Penyakit Thyroid atau parathyroid

50
Penyebab Hipertensi Resisten
Pengukuran Tekanan Darah yang salah Intake sodium berlebihan Terapi diuretik inadekuat Obat Dosis inadekuat Efek dan interaksi obat: NSAIDs, simpatomimetik, OCP Obat bebas dan herbal Minum alkohol

51
Obat yang menyebabkan Hipertensi
Steroids Estrogens NSAIDS Phenylpropanolamines Cyclosporine/tacrolimus Erythropoietin Sibutramine Methylphenidate Ergotamine Ketamine Desflurane Carbamazepine Bromocryptine Metoclopramide Antidepressants Venlafaxine Buspirone Clonidine

52
Kombinasi obat HT Keuntungan Kombinasi yang rasional
Mempunyai efek sinergis Mempunyai sifat aditif Saling mengisi Efek samping masing-masing obat diminimalkan Kombinasi yang rasional ACE inhibitor dengan diuretik ACE inhibitor dengan kalsium antagonis Beta bloker dengan kalsium antagonis Beta bloker dengan diuretik

53
Kombinasi obat Apabila pemberian obat tunggal dengan dosis maksimum masih belum mencapai target TD Tambahkan obat kedua Pemberian dua macam obat akan meniadakan efek sampingnya Pemberian obat “ fixed dose combination” akan menurunkan jumlah tablet obat Pemberian obat sekali sehari akan meningkatkan kepatuhan pasien Sediaan ‘sustained release’ atau ‘lepas lambat’ efeknya 24 jam Apabila menggunakan 3 macam obat masih tidak menurunkan TD hipertensi resisten

54
Drug Combinations

55
Target Terapi Targetnya adalah Tekanan darah Sistolik dan Diastolik <140/90 mmHg Pasien dengan diabetes atau penyakit ginjal, target TD <130/80 mmHg Fokus primer adalah target TD sistolik Untuk menurunkan morbiditas dan mortalitas kardiovaskuler dan renal

56
Perjalanan penyakit dan Komplikasi
Tanpa komplikasi Menjadi accelerated – malignant Kerusakan target organ : Penyakit jantung Hipertrofi ventrikel kiri Infark miokard Gagal jantung Stroke : iskemi / perdarahan Aneurisma / aorta diseksi Nefrosklerosis / GGK Retinopati

57
Komplikasi Hipertensi Kronis tak terkontrol
Perubahan dinding pembuluh darah yang menyebabkan trauma pemb darah dan arteriosklerosis di sepanjang vasculature Komplikasi timbul karena disfungsi dan kegagalan “target organ” Kerusakan pembuluh darah dapat dilihat dengan fundoscopy.

58
Target Organ CVS (Jantung dan Pembuluh Darah) Ginjal Sistem saraf Mata
 Ginjal Sistem saraf Mata")
59
Efek pada Jantung dan Pembuluh Darah
Hipertrofi Ventricular, disfungsi dan kegagalan Aritmia Coronary artery disease, Acute MI Arterial aneurysm, dissection, and rupture.

60
Efek pada Ginjal Glomerular sclerosis menyebabkan kegagalan fungsi ginjal dan akhirnya end stage kidney disease. Ischemic kidney disease terutama bila terjadi renal artery stenosis adalah penyebab hipertensi

61
Sistem Saraf Stroke, intracerebral dan subaracnoid hemorrhage.
Cerebral atrophy dan dementia

62
M a t a Retinopathy, retinal hemorrhages dan gangguan penglihatan
Vitreous hemorrhage, retinal detachment Neuropathy of the nerves leading to extraoccular muscle paralysis and dysfunction

63
Krisis Hipertensi Definisi :
Peningkatan TD diastolik yang sangat tinggi, dimana TD diastolik > 120 mmHg Dibagi 2 : Hipertensi emergensi Sudah ada kerusakan target organ Hipertensi urgensi Belum ada kerusakan target organ

64
Penanganan HT Emergensi
Harus dilakukan di RS / Ruang ICU Menurunkan tekanan arteri rata-rata kurang lebih 25% dari TD awal Waktu terapi < 2 jam Menggunakan obat intravena / infussion Macam obat : Sodium nitroprussid, dosis 0,25-10 mcg/kgBB/men. Nitrogliserin, dosis 0,5 – 8 mcg / kg BB / menit. Diassoksid , dosis 50 – 100 mg bolus.

65
Penanganan HT urgensi Penurunan TD secara bertahap dalam 24 – 48 jam
Dengan obat oral , atau IV : Captopril mg, sublingual Nifedipin mg, sublingual Labetalol , 200 – 400 mg, IV Furosemid 40 mg, IV Clonidin 0,1 – 0,4 mg / jam, IV

66
Terima Kasih

Presentasi serupa

>")


>")














 “>")
