Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
Burn Injury : WHATS NEW IN BURN RESUSCITATION
Lisa Hasibuan Divisi Bedah Plastik Dept. Bedah RS Hasan Sadikin/FK UnPad BANDUNG Disampaikan pada Acute Care Surgery- Februari Bandung

2
WHATS NEW IN BURN RESUSCITATION
GAMBARAN SAAT INI MASALAH YANG TIMBUL KEMAJUAN YANG SUDAH DITEMUKAN UNTUK MENGATASI MASALAH-MASALAH TERSEBUT

3
GAMBARAN RESUSITASI SAAT INI
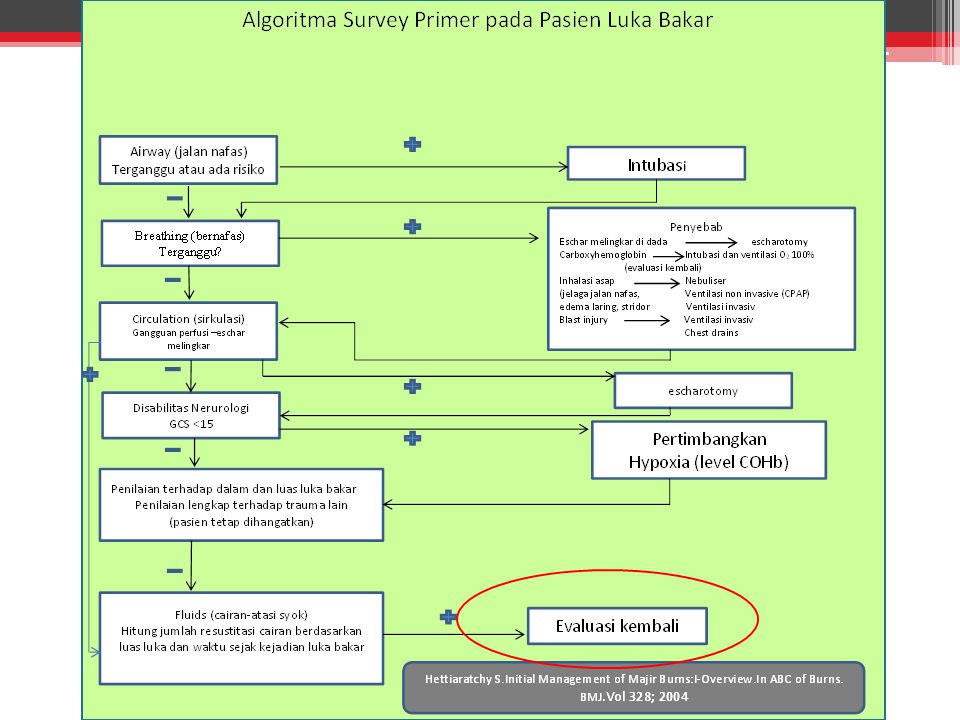
AIRWAY INTUBASI DINI UNTUK PASIEN DENGAN KECURIGAAN TRAUMA INHALASI BREATHING PEMBERIAN OKSIGEN 100% VIA NRM CIRCULATION RESUSITASI CAIRAN

4
AIRWAY DAN BREATHING MASALAH YANG TIMBUL SAAT INI
INTUBASI DINI PADA PASIEN DENGAN KECURIGAAN TRAUMA INHALASI Ching J, et al (2014) meneliti 47 pasien dengan temuan singed nasal hair, carbonaceous sputum, facial burns yang diintubasi dengan bronkoskopi. Hasil bronkoskopi normal ditemukan pada 66% (31 pasien), sehingga ketiga temuan tersebut bukanlah indikasi kuat untuk dilakukan intubasi.
 meneliti 47 pasien dengan temuan singed nasal hair, carbonaceous sputum, facial burns yang diintubasi dengan bronkoskopi. Hasil bronkoskopi normal ditemukan pada 66% (31 pasien), sehingga ketiga temuan tersebut bukanlah indikasi kuat untuk dilakukan intubasi.")
5
Cancio LC (2009) merekomendasikan fiberoptic/direct laryngoscope untuk visualisasi dini sebelum dilakukan intubasi Mackie DP (2013) penggunaan ventilator meningkatkan resiko terjadinya ARDS dan ventilator-associated pneumonia Eastman AL (2010) meneliti dalam jangka waktu 23 tahun, dari pasien yang datang sudah terintubasi, 26,3% diintubasi karena kecurigaan trauma inhalasi dan terbukti dengan bronkoskopi pada 88,6% pasien tersebut. Dari 879 pasien luka bakar (survivors) yang diintubasi, 28% pasien diintubasi sebagai profilaksis, 34,1 % diintubasi karena pembengkakan jalan nafas, 13,2 % diintubasi untuk keperluan ventilasi dan oksigenasi.
 penggunaan ventilator meningkatkan resiko terjadinya ARDS dan ventilator-associated pneumonia. Eastman AL (2010) meneliti dalam jangka waktu 23 tahun, dari pasien yang datang sudah terintubasi, 26,3% diintubasi karena kecurigaan trauma inhalasi dan terbukti dengan bronkoskopi pada 88,6% pasien tersebut. Dari 879 pasien luka bakar (survivors) yang diintubasi, 28% pasien diintubasi sebagai profilaksis, 34,1 % diintubasi karena pembengkakan jalan nafas, 13,2 % diintubasi untuk keperluan ventilasi dan oksigenasi.")
6
Apabila jelas kecurigaan trauma inhalasi dari anamnesis, pemeriksaan fisik, bila mungkin bronkoskopi/direct laryngoscope maka harus dilakukan intubasi, walaupun belum ada tanda respiratory distress

7
AIRWAY DAN BREATHING PEMBERIAN 100% O2 VIA NON-REBREATHING MASK / ETT
TARGET : SpO2 >92% COHb <5%

8
CIRCULATION RESUSITASI CAIRAN

9
RESUSITASI CAIRAN PADA LUKA BAKAR
Resusitasi cairan akut merupakan aspek mendasar pada perawatan luka bakar modern important shift Menimbulkan banyak komplikasi yang berkaitan dengan edema Fluid resusitation pada burn adalah suatu hal yang sangat fundamental. Akhir-akhir ini terdapat perubahan penting dalam pengertian dan pendekatan resusitasi cairan pada burn yang berasal dari temuan2 komplikasi yg berhubungan dgn edema. Seringkali sudah dapat memenuhi kebutuhan cairan BERLEBIHAN

10
In recent years, however, there has been an important shift in the understanding of and approach to fluid resuscitation, fueled largely by increasing recognition that modern crystalloid resuscitation frequently provides substantial volumes of fluid, often in excess of that predicted by current formulas, resulting in numerous edema- related complications

11
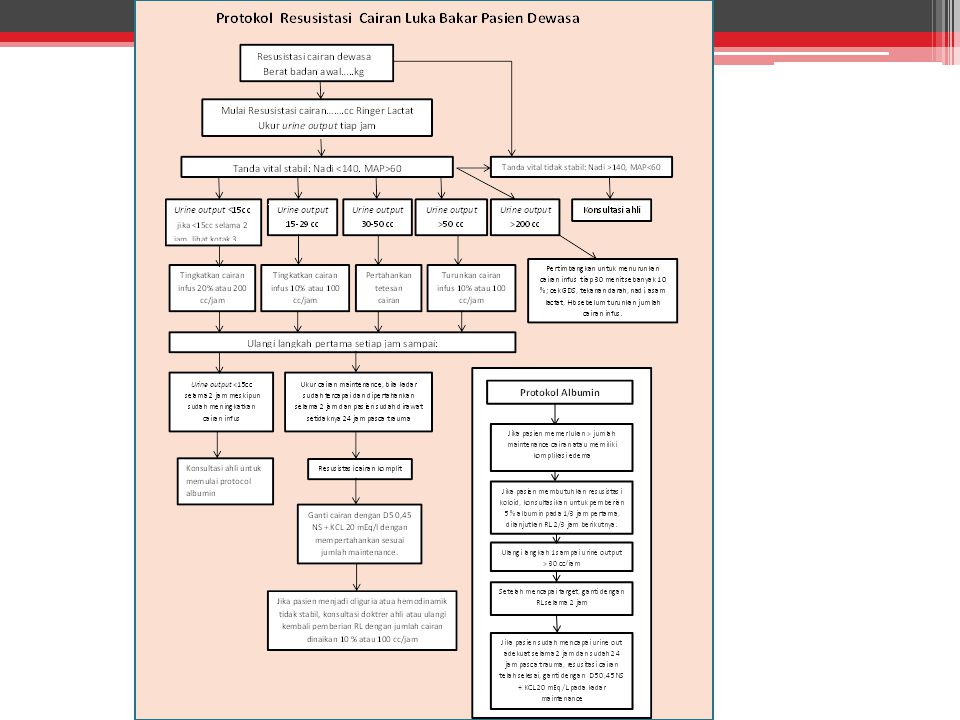
PERKIRAAN KEBUTUHAN CAIRAN: Parkland Formula
Dewasa : 3-4 cc kristaloid x kg BB x % luka bakar untuk 24 jam Anak : 3-4 cc kristaloid x kg BB x % luka bakar ditambah maintenance : 5% Glucose in 0,45%(½ normal) saline (D5½NS) 100 ml/kg untuk 10 kg pertama 50 ml/kg untuk 10 kg kedua 20 ml/kg selebihnya Cairan maintenance untuk anak diberikan dalam kecepatan tetap selama 24 jam
 saline (D5½NS) 100 ml/kg untuk 10 kg pertama. 50 ml/kg untuk 10 kg kedua. 20 ml/kg selebihnya. Cairan maintenance untuk anak diberikan dalam kecepatan tetap selama 24 jam.")
12
PENILAIAN KECUKUPAN RESUSITASI CAIRAN Urine Output
Dewasa : 0,5 ml/kg/jam = 30 – 50 ml/jam Anak (< 30 kg) : 1,0 ml/kg/jam (range 0,5-2 ml/kg/jam) mL/kg/jam (dewasa) dan mL/kg/jam (anak) Guidelines of the American Burn Association : 24 jam kedua = koloid 0,5 ml albumin 5% x kg BB x % luka bakar
 : 1,0 ml/kg/jam (range 0,5-2 ml/kg/jam) mL/kg/jam (dewasa) dan mL/kg/jam (anak) Guidelines of the American Burn Association : 24 jam kedua = koloid. 0,5 ml albumin 5% x kg BB x % luka bakar.")
13
RESUSITASI CAIRAN TAMBAHAN PADA KASUS:
Anak Trauma inhalasi Trauma listrik Resusitasi terlambat/ tertunda Dehidrasi : pemadam kebakaran, pasien keracunan Bayi, usia lanjut, dan pasien dengan penyakit jantung harus dimonitor ketat karena resusitasi cairan dapat memperberat overload

14
MASALAH YANG TIMBUL

15
KONSEKUENSI PEMBERIAN CAIRAN TAMBAHAN
Pembengkakan jalan nafas intubasi profilaksis Abdominal Compartment Syndrome sekunder Edema jaringan lunak di ekstremitas tindakan eskarotomi, bahkan fasiotomi Meningkatkan tekanan intraokular Secara keseluruhan: meningkatkan resiko kematian

16
Abdominal Compartment Syndrom Edema Larynx ARDS Anasarca
Orbital Compartment Syndrome Extremity Compartment Syndrome Bila > 237 ml/kg sepanjang fase akut Fluid Creep

17
Fluid Creep

18
Gambar 1. pasien usia lanjut dengan “fluid creep”.
25% TBSA luka bakar full-thickness tanpa inhalasi asap 16 jam sebelumnya 15 jam setelah terjadi luka bakar pasien menerima total cairan 7901 cc (62% lebih besar dari perhitungan Parkland) Namun urine output hanya rata-rata 48 cc/jam (0,7 cc/kg/jam) Pasien mulai menunjukkan tanda awal obstruksi jalan nafas atas karena edema dan membutuhkan intubasi profilaksis
 Namun urine output hanya rata-rata 48 cc/jam (0,7 cc/kg/jam) Pasien mulai menunjukkan tanda awal obstruksi jalan nafas atas karena edema dan membutuhkan intubasi profilaksis.")
19
JADI PADA RESUSITASI CAIRAN
Seberapa banyak “cukup” (tidak lebih tidak kurang)? Menggunakan perhitungan yang mana? Jenis cairan apa? Kapan memberikannya? Bagaimana cara memonitor? Adakah peralatan memadai untuk resusitasi akurat? Atiyeh BS, Dibo SA. Acute Burn Resuscitation and Fluid Creep: it is time for Colloid Rehabilitation. Annuals of Burns and Fire Disaster. Vol XXV (2). June 2012
 Menggunakan perhitungan yang mana Jenis cairan apa Kapan memberikannya Bagaimana cara memonitor Adakah peralatan memadai untuk resusitasi akurat Atiyeh BS, Dibo SA. Acute Burn Resuscitation and Fluid Creep: it is time for Colloid Rehabilitation. Annuals of Burns and Fire Disaster. Vol XXV (2). June")
20
RESUSITASI YANG SUDAH ADA
Penelitian terkini mengenai resusitasi cairan difokuskan pada pendekatan untuk mencegah fluid creep, termasuk di dalamnya: Kontrol ketat kecepatan infus cairan, penggunaan koloid awal dan secara liberal, dan penggunaan hypertonic saline (HTS) RE-EVALUASI RESUSITASI YANG SUDAH ADA
 RE-EVALUASI. RESUSITASI YANG SUDAH ADA.")
22
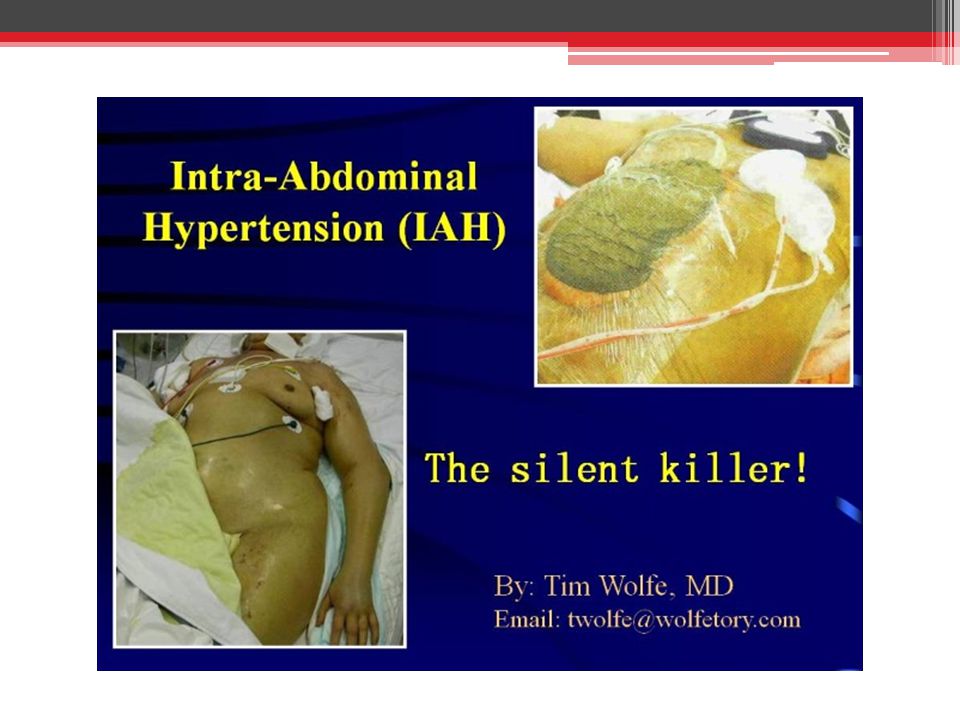
Intra Abdominal Hypertension
IAH merupakan kelainan patologik dengan tekanan intra abdominal >12 mmHg Klasifikasi: - Tekanan - Jenis - Onset ______________________________________ Sugrue. Abdominal compartment syndrome. Curr Opin Crit Care. 2005; 11 ;

23
Faktor predisposisi Intra- Abdominal Hypertension (IAH)
Hipotermia Transfusi Masif Sepsis Ventilasi mekanik Pneumonia Acidosis Resusitasi cairan berlebihan

24
Abdominal Compartment Syndrome
Definisi ACS = nilai puncak tekanan intraabdomen >20 mmHg yang tercatat minimal dua kali menggunakan pengukuran terstandar dengan interval 1-6 jam Disertai dengan kegagalan organ multipel yang sebelumnya belum ada (The International ACS Consensus Definitions Conference (2006) Tidak ada sistem 'grading' (klasifikasi)
 Tidak ada sistem grading (klasifikasi)")
25
ACS Primer Cedera atau penyakit di abdomen atau pelvis
Penanganan non-operatif pada cedera organ padat Muncul setelah operasi abdomen Damage control Fraktur pelvis Transplantasi hepar

26
ACS Sekunder Dari luar abdomen Luka bakar luas Sepsis
Kondisi yang membutuhkan resusitasi cairan masif

27
Efek Kardiovaskuler dari ACS
↑ tekanan intra toraks ditransmisikan melalui diafragma Penekanan Vena Cava Inferior ↑ CVP ↓ Preload ↑ Afterload dengan ↑ PVR

28
Efek Pulmonal dari ACS ↑ Peak airway pressure Poor compliance
↑ End-inspiratory pressure Gangguan mekanis diafragma Penurunan aliran darah pulmonalflow V/Q mismatch PaO2 Intractable hypercarbia

29
Efek Renal dari ACS Kompresi vena renalis Kompresi parenkim ginjal
Mengalihkan aliran dari korteks dan glomeruli yang berfungsi ↑ produksi Anti-Diuretic Hormone Oliguria/Anuria

30
IAH dan ACS Grading of IAP as determined by intravesical pressure, & summary of clinical effects _____________________________________________________________________________________________________________________________ Grade IAP (mmHg/ cmH20) Clinical I (10-15) None IIa (16-25) Oliguria, splanchnic hypoperfusion IIIb (26-35) Anuria, ↑ ventilation pressure Ivb >25.7 (>35) As above & ↓ p02 _______________________________________________________________________________ a = initial therapy aims to restore splanchnic & renal hypoperfusion by volume replacement b = these pts will probably require urgent abdominal decompression _____________________________________________________ Meldrum DR, Moore FA, Moore FE, et al. Am J Surg174:667; 1997
 Clinical. I (10-15) None. IIa (16-25) Oliguria, splanchnic hypoperfusion. IIIb (26-35) Anuria, ↑ ventilation pressure. Ivb >25.7 (>35) As above & ↓ p02. _______________________________________________________________________________. a = initial therapy aims to restore splanchnic & renal hypoperfusion by volume replacement. b = these pts will probably require urgent abdominal decompression. _____________________________________________________ Meldrum DR, Moore FA, Moore FE, et al. Am J Surg174:667;")
31
Diagnosis Insiden 5%-15% pada pasien kritis
Angka mortalitas 63% - 72%. ____________________________________ IAP Normal (Sanchez NC dkk, 2001) : 0-5 mmHg Obesitas dan hamil (IAP kronik) : mmHg Critically III (Malbrain ML dkk, 2006) : 5-7 mmHg _________________________________________________________________ Insiden pada luka bakar 2 – 7% Angka mortalitas pada luka bakar > 80%
 : 0-5 mmHg. Obesitas dan hamil (IAP kronik) : mmHg. Critically III (Malbrain ML dkk, 2006) : 5-7 mmHg. _________________________________________________________________. Insiden pada luka bakar 2 – 7% Angka mortalitas pada luka bakar > 80%")
32
Diagnosis IAH Distensi abdomen Compliance paru ↓ (PIP↑) Oliguria
Hipotensi dan cardiac output ↓ Tek vena sentral (CVP) ↑
 ↑")
33
Penatalaksanaan ACS* Bladder Pressure Treatment 10-15 mmHg Monitor
26-35 mmHg Dekompresi > 35 mmHg Dekompresi dan reeksplorasi * Meldrum et al, Am J Surg 1997

34
The Problems The "Standard of Care” untuk ACS adalah LAPAROTOMI
Additional morbidity of laparotomy Operating Room vs. Bedside Surgery Temporary closures are temporary percutaneous decompression before decompressive laparotomy The "Standard of Care” untuk ACS adalah LAPAROTOMI DEKOMPRESI

35
Sasaran Penutupan Sementara (Temporary Closure)
Waktu yang dibutuhkan singkat Minimalisasi kehilangan panas dan cairan Minimalisasi kehilangan abdominal domain

36
Bogota Bag + lebih murah + lebih mudah tersedia
+ mengurangi kehilangan cairan - kehilangan abdominal domain - mudah robek - wajib dilakukan tindakan selanjutnya (definitif)
")
37
Penutupan Vacuum-Assisted
Mengurangi insidensi ACS Mencegah kehilangan abdominal domain ↓ kebutuhan untuk dialisis peritoneal

39
Eskarotomi dan Paracentesis pada pasien luka bakar dengan IAH
Jika pada pasien terdapat luka bakar di batang tubuh (torso), tatalaksana pertama untuk peningkatan tekanan intraabdomen mungkin eskarotomi, supaya rongga abdomen dapat meregang dan mengurangi tekanan intraabdomen Paracentesis/ drainase perkutaneus : untuk mengeluarkan kebocoran cairan dari kapiler dan sitokin proinflamasi dari rongga abdomen mengurangi tekanan intraabdomen
, tatalaksana pertama untuk peningkatan tekanan intraabdomen mungkin eskarotomi, supaya rongga abdomen dapat meregang dan mengurangi tekanan intraabdomen. Paracentesis/ drainase perkutaneus : untuk mengeluarkan kebocoran cairan dari kapiler dan sitokin proinflamasi dari rongga abdomen mengurangi tekanan intraabdomen.")
41
Kapan KOLOID digunakan?
Parkland formula : 0.3 to 0.5 mL/kg/%TBSA 5% albumin selama 24 jam kedua dalam resusitasi Pendekatan terkini adalah pemberian koloid sebagai teknik “rescue” ketika kebutuhan kristaloid menjadi berlebihan. start albumin pada 12 jam pertama postburn jika kebutuhan cairan lebih dari 120% dari prediksi.(Yowler and Fratienne) albumin untuk oliguria atau kecepatan infus lebih dari dua kali dari perhitungan selama lebih dari 2 jam.(Saffle) 5% albumin pada jam pertama, jika perkiraan kebutuhan 24 jam melebihi 6 mL/kg/%TBSA (Chung et al).
 albumin untuk oliguria atau kecepatan infus lebih dari dua kali dari perhitungan selama lebih dari 2 jam.(Saffle) 5% albumin pada jam pertama, jika perkiraan kebutuhan 24 jam melebihi 6 mL/kg/%TBSA (Chung et al).")
43
KESIMPULAN Perhitungan menggunakan formula Parkland dapat digunakan sebagai acuan untuk menentukan kecepatan awal infus cairan pada resusitasi luka bakar Kecepatan dan jumlah cairan harus terus disesuaikan dengan respon pasien. Resusitasi cairan harus menggunakan jumlah cairan yang paling sedikit (antara 2-4cc/kgBB/%TBSA) yang dibutuhkan untuk mencapai urine output yang cukup dan mencegah kegagalan organ dan mencegah komplikasi.
 yang dibutuhkan untuk mencapai urine output yang cukup dan mencegah kegagalan organ dan mencegah komplikasi.")
44
KESIMPULAN Pasien dengan resiko tinggi harus selalu dimonitor untuk hipertensi abdomen Pengukuran berulang IAP (Intra Abdominal Pressure) harus dilakukan pada pasien resiko tinggi Dekompresi perkutaneus adalah salah satu pilihan untuk mencegah progresi ke laparotomi dekompresi pada kasus luka bakar abdominal/batang tubuh, diikuti dengan dialisis peritoneal Tatalaksana definitif untuk ACS adalah laparotomi dekompresi
 harus dilakukan pada pasien resiko tinggi. Dekompresi perkutaneus adalah salah satu pilihan untuk mencegah progresi ke laparotomi dekompresi pada kasus luka bakar abdominal/batang tubuh, diikuti dengan dialisis peritoneal. Tatalaksana definitif untuk ACS adalah laparotomi dekompresi.")
45
THANK YOU Hatur nuhun

47
ACS as an intra-abdominal pressure greater than 20 mm Hg with evidence of new organ dysfunction (typically manifested as oliguria, impaired mechanical ventilation with high peak airway pressures, worsening metabolic acidemia, and hemodynamic instability). When cumulative volumes reach 250 mL/kg or more intra-abdominal pressure measurements (by bladder pressure transduction) should be performed every 2 jams and conservative measures to reduce intra- abdominal pressure should be considered
 should be performed every 2 jams and conservative measures to reduce intra- abdominal pressure should be considered.")
48
penting IAH and possibly early ACS may be reversed by the insertion of peritoneal dialysis catheters to remove peritoneal fluid, but this does not treat the edema of the intra-abdominal tissues and organs, and with more severe ACS, particularly with massive burn injury, definitive treatment by decompressive laparotomy may be required. Mortality following surgical decompression for ACS is reported to be between 50% and100%.

49
ACS is defined as a peak IAP value of ≥ 20 mACS is defined as a peak IAP value of ≥ 20 mmHg recorded during a minimum of 2 standardized measurements that are performed 1-6 jams apart with associated single or multiple organ system failure which was not previously present

50
Bladder pressure is not routinely measured by 22 (69%) burn physicians, and staff at 17 centers (53%) wait until the abdomen is tense to measure abdominal pressure. Tense abdomen, along with elevated peak inspiratory pressures (PIP), is used in most centers (94%) to determine IAH/ACS, followed by oliguria (88%), and difficulty ventilating (78%). Resuscitation formulae used are primarily the Parkland/modified Parkland in 24 (75%) burn centers
, is used in most centers (94%) to determine IAH/ACS, followed by oliguria (88%), and difficulty ventilating (78%). Resuscitation formulae used are primarily the Parkland/modified Parkland in 24 (75%) burn centers.")
51
Other Techniques for Temporary Closure
Running nylon and/or towel clips Absorbable (Dexon/Vicryl) mesh Plastic sheet (loban) Wound VAC
 mesh. Plastic sheet (loban) Wound VAC.")
52
Excessive Fluid Resuscitation
Post-resuscitation pulmonary edema Conversion of superficial -> deep burn Need for unburned limb fasciotomies Abdominal compartment syndrome

53
After more than four decades of acceptance of the Parkland formula as a cornerstone of burn
care, and despite the fact that this approach has provided effective resuscitation that has markedly reduced the incidence of burn shock-induced acute renal failure, several reports have recently surfaced that show that modern burn Setelah lebih dari empat dekade penggunaan formula Parkland dalam penanganan luka bakar, terbukti bahwa resusitasi yg efektif dg formula ini telah secara bermakna mengurangi angka kejadian acute renal failure yg di-induced oleh burn shock.

54
Currently, some experts recommend maintenance of UO of 30 to 50 mL/h in adults and 1 to 2 mL/kg/h in children weighing less than 30 kg,49whereas current Practice Guidelines of the American Burn Association advise maintenance of UO at approximately 0.5 to 1 mL/kg/h in adults and 1 to 1.5 mL/kg/h in children.50

55
This increase in capillary permeability is most profound acutely and may remain elevated for several days postburn. The severity and duration of the leak is directly proportional to the extent of the burn. When the burn size approaches 25% to 30% TBSA or larger, edema in the unburned skin and soft tissues develops.24 Acutely, within the first few jams postburn, there is an increase in capillary permeability (s), which may be caused by the systemic dissemination of inflammatory mediators.
, which may be caused by the systemic dissemination of inflammatory mediators.")
56
The more pressing problem for the modern burn clinician is fluid creep, which is the unpredictable trend toward provision of larger and larger resuscitation fluid volumes to burn patients who do not fit into the well- defined subgroups identified previously. A number of recent studies have found that crystalloid fluid resuscitation volumes for the initial 24 jams postburn among burn patients have ranged between 4.8 and 6.7 mL/kg/ %TBSA,13–18 in many instances independent of the presence of a documented inhalation injury. The consequences of this increased fluid administration are similarly well characterized, and include airway swelling requiring prophylactic intubation58 (see Fig. 1), secondary ACS,59 soft tissue edema in the extremities necessitating more frequent escharotomies and even fasciotomies,58 elevated intraocular pressures,60 and an overall increased risk of death.18 The development
, secondary ACS,59 soft tissue edema in the extremities necessitating more frequent escharotomies and even fasciotomies,58 elevated intraocular pressures,60 and an overall increased risk of death.18 The development.")
57
Rigid adherence to a fluid infusion rate prescribed by a formula is potentially harmful. Rather, the clinician should continually adjust the infusion rate based on the patient’s response. Practically, this is based on evaluation of the UO at 1- to 2- jam intervals. A protocol, such as that describedby Saffle,69 is one of several ways to achieve this goal. In this strategy, an jam of UO less than 15 mL calls for an increase in the infusion rate by 20% or 200 mL/h, whichever is greater; an jam with UO 15 to 30 mL gets an increase of 10% or 100 mL/h, whichever is greater; and jam with UO 30 to 50 mL prompts no change in the infusion rate. Conversely, for UO greater than 50 mL/h the infusion rate for the next jam is decreased by 10% or 100 mL/h, whichever is greater. Within this particular protocol, persistent oliguria or escalating fluid infusion rates are managed by institution of albumin, described next.

58
Not surprisingly, as a consequence of these large resuscitation volumes, complications related to edema formation led chiefly by secondary abdominal compartment syndrome (ACS), have also appeared. Current research in fluid resuscitation now concentrates on approaches to minimize fluid creep, including tighter control of fluid infusion rates, earlier and more liberal use of colloids, and the use of hypertonic saline (HTS). Sebagai konsekuensi dari volume cairan resusitasi yang begitu besar, komplikasi2 yg terjadi mulai bermunculan, a.l abdominal compartment sindrom (ACS). Penelitian2 terakhir mengemukakan pendekatan2 utk meminimalisir fenomena fluid creep, termasuk di dlmnya kontrol ketat kecepatan infus, penggunaan koloid yang lebih awal dan penggunaan hipertonic saline.
. Sebagai konsekuensi dari volume cairan resusitasi yang begitu besar, komplikasi2 yg terjadi mulai bermunculan, a.l abdominal compartment sindrom (ACS). Penelitian2 terakhir mengemukakan pendekatan2 utk meminimalisir fenomena fluid creep, termasuk di dlmnya kontrol ketat kecepatan infus, penggunaan koloid yang lebih awal dan penggunaan hipertonic saline.")
59
Systemic Changes

60
Correction of the hypoproteinemic state with infusions of albumin or plasma hinders the development of nonburn soft tissue edema.25,38 The most important consequence of the aforementioned fluid shifts is a reduction in circulating plasma volume. Cardiac output (CO) falls, largely because of hypovolemia and reduced preload,but interestingly in larger burns (R40% TBSA), an immediate fall in CO has been repeatedly observed before any measurable decrease in the plasma volume, suggesting that depressed myocardial contractility plays a role. Earlier literature suggested that an uncharacterized ‘‘myocardial depressant factor’’ was responsible,39–42 and it is now thought that inflammatory mediators from the burn wound, distributed systemically, are responsible
 falls, largely because of hypovolemia and reduced preload,but interestingly in larger burns (R40% TBSA), an immediate fall in CO has been repeatedly observed before any measurable decrease in the plasma volume, suggesting that depressed myocardial contractility plays a role. Earlier literature suggested that an uncharacterized ‘‘myocardial depressant factor’’ was responsible,39–42 and it is now thought that inflammatory mediators from the burn wound, distributed systemically, are responsible.")
61
Simultaneous with the acute reductions in plasma volume and CO, systemic vascular resistance increases because of sympathetic-mediated peripheral vasoconstriction and the effects of increased viscosity of the blood because of hemoconcentration. The elevation in systemic vascular resistance is an additional factor that contributes to the acute depression of CO.45 Organ perfusion, particularly renal blood flow, is compromised as a result of the hypovolemic state, depressed CO, and peripheral vasoconstriction, especially if fluid resuscitation is delayed. As resuscitation proceeds, CO slowly climbs back to normal and in patients with major burn injuries, a hyperdynamic picture with supranormal CO develops by 36 to 72 jams postburn as part of the hypermetabolic response. The intended goal of fluid resuscitation is to re-expand the plasma volume, restore CO, and improve organ and tissue perfusion. It should be evident from the foregoing discussion that crystalloid resuscitation fluids, although necessary to achieve the goal of restoring tissue perfusion, are also subject to the altered Starling forces and as such, large amounts of the resuscitation fluid necessarily end up as interstitial and cellular edema fluid.

62
The development of intra-abdominal hypertension (IAH) and the ACS deserve special mention because these are perhaps the most dangerousand frequently reported consequences of fluid creep in association with massive burn resuscitation (Fig. 4).59,61–64 The most recent Consensus Guidelines define IAH as an intra-abdominal pressure (obtained by transduction of bladder pressure) greater than or equal to 12 mm Hg and
.59,61–64 The most recent Consensus Guidelines define IAH as an intra-abdominal pressure (obtained by transduction of bladder pressure) greater than or equal to 12 mm Hg and.")
63
ACS as an intra-abdominal pressure greater than 20 mm Hg with evidence of new organ dysfunction (typically manifested as oliguria, impaired mechanical ventilation with high peak airway pressures, worsening metabolic acidemia, and hemodynamic instability).65 ACS is considered secondary when there is no demonstrable intraabdominal pathology,65 as in the case of a burn where bowel and mesenteric edema and increased peritoneal fluid are the cause of the raised intra- abdominal pressures. Left untreated, ACS is invariably fatal, and probably was the cause of early ‘‘death due resuscitation failure’’

64
When cumulative volumes reach 250 mL/kg or more intra-abdominal pressure measurements (by bladder pressure transduction) should be performed every 2 jams and conservative measures to reduce intra- abdominal pressure should be considered.62,66 These include use of neuromuscular relaxants and increased sedation in mechanically ventilated patients; extension of escharotomies on any anterior trunk burns (Fig. 5); and possible judicious use of diuretics if adequate intravascular volume can be confirmed by placement of a pulmonary artery catheter, which demonstrates pulmonary capillary wedge pressures greater than 18 mm Hg.62,66,6
; and possible judicious use of diuretics if adequate intravascular volume can be confirmed by placement of a pulmonary artery catheter, which demonstrates pulmonary capillary wedge pressures greater than 18 mm Hg.62,66,6.")
65
The trend toward abandonment of colloids over the past two or three decades may also have contributed to the subtle advance of fluid creep.69 Baxter’s original approach included use of plasma at 24 jams, and two well-conducted randomized prospective studies both demonstrated that early use of colloids significantly reduced 24-jam resuscitation volumes, compared with use of crystalloids alone.70,71 An intriguing theory on fluid creep has been described by Saffle,69 who suggests that

66
jamly urine output is still the cornerstone of monitoring of burn resuscitation despite the emergence in the past decade of more sophisticated approaches, such as the use of malperfusion markers (arterial base deficit and serum lactate); cardiac index determinations; measurements of oxygen delivery and uptake variables; and intrathoracic blood volume estimations. The fluid infusion rate should be adjusted to achieve a UO of 0.5 to 1 mL/kg/h in adults and 1 to 1.5 mL/kg/h in children. 50 It has never been specified whether this should be based on actual or predicted weight, but in heavier and obese patients, aiming for a UO at the lower end of the range seems to make sense to use the least amount of fluid possible. The arterial base deficit and serum lactate are well-recognized markers of tissue malperfusion that have been used to monitor resuscitation in trauma and critically ill populations.

67
Criteria for abdominal decompression is based on bladder pressures alone in 25 centers (78%); 16/32 (50%) use PIP, and 10/32 (31%) staff use other criteria including organ dysfunction or increased lactate. Eleven physicians (34%) advocate percutaneous decompression before decompressive laparotomy.
 advocate percutaneous decompression before decompressive laparotomy..")
68
Research Questions Asked at the University of Iowa
What is the etiology of the ACS in acute thermal injury ? Is decompressive laparotomy the only method of treatment?

69
Criteria for abdominal decompression is based on bladder pressures alone in 25 centers (78%); 16/32 (50%) use PIP, and 10/32 (31%) staff use other criteria including organ dysfunction or increased lactate. Eleven physicians (34%) advocate percutaneous decompression before decompressive laparotomy.
 advocate percutaneous decompression before decompressive laparotomy..")
70
Materials & Methods Intra-abdominal pressure measurement
(bladder transducer) for >40% TBS A burns Percutaneous peritoneal lavage catheter placement if pressure >25 mmHg Decompressive laparotomy if PD failed
 for >40% TBS A burns. Percutaneous peritoneal lavage catheter. placement if pressure >25 mmHg. Decompressive laparotomy if PD failed.")
71
Resuscitation Fluid Standard: Modified Parkland Formula - 4ml/kg/%TBSA
- 6mi/kg/%TBSA if Inhalation injury also Study Patients - 3.7 cc/kg/%TBSA - (range =2-5 cc/kg/%TBSA)
")
72
PD vs PD+Laparotomy N=6 Dead: PD n=10 Dead:PD+Lap Age (yrs) 40 54 37
%TBSA Vent/LOS Bladder

73
Nonsurvivors had: ↑ ............../............ - ↑ bladder pressure
- ↓ peritoneal drainage - ↑ fluid intake - Lower Pa02/Fi02 ratios, p<0.02

74
Findings Patients with < 80%TBSA & inhalation
injury responded to PD Patients with >8Q%TBSA & inhalation injury tailed PD Autopsy: no intra-abdominal sepsis or bowel complications seen

75
Secondary ACS Non-abdominal conditions -Major burns -Sepsis
-Conditions requiring massive fluid resuscitation

76
Tertiary ACS • Also known as recurrent ACS
• Develops after treatment of 1o • or 2o ACS • Recurrent or new episode • after definitive abdominal wall • closure

77
Measuring Methods Direct Direct needle puncture and transducer
Intermittent Indirect Bladder pressure transducer Continuous Indirect Continuous bladder irrigation method

78
This phenomenon, coined ‘‘fluid creep’’ by Pruitt
It is increasingly recognized that fluid resuscitation is anything but a rote, standardized process, and that there is an urgent need for re-evaluation of existing resuscitation approaches to avoid fluid creep. The more pressing problem for the modern burn clinician is fluid creep, which is the unpredictable trend toward provision of larger and larger resuscitation fluid volumes to burn patients who do not fit into the well- defined subgroups identified previously.

79
Predisposition for ACS in Burns
Large volume fluid resuscitation Circumferential torso burns Inhalation Injury

80
How Do We Define Abdominal Compartment Syndrome?
IAP > 20 mm Hg AND new onset single/multiple organ failure There is no grading system

Presentasi serupa














 Spine>")


>")


