Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
CRPC : Choosing The Right Treatment for The Right Patient
Ferry Safriadi Department of Urology Hasan Sadikin General Hospital Medical School of Padjadjaran University 7th URO-ONCOLOGY UPDATE, Feb 2016

3
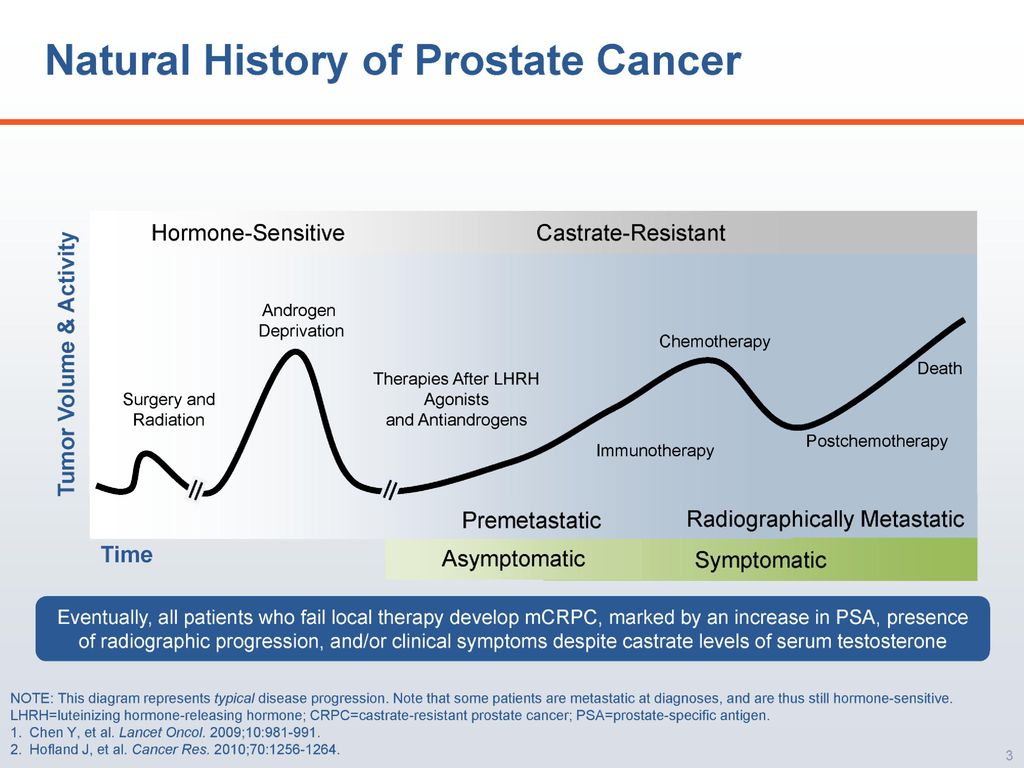
Prostate Cancer is an Androgen-Dependent Disease
Androgens play a critical role in prostate cancer Male sex hormones play a vital role in the development and growth of prostate cancer cells Proliferation and survival of cancerous cells are: Mediated by androgen receptor (AR) responsive pathways Driven by circulating testosterone In 1941, Huggins & Hodges first proved that reducing androgen concentrations in prostate cancer patients leads to: Regression of tumours Relief of cancer symptoms CRPC Is an Androgen-Sensitive Disease Despite castration levels of androgen after Androgen Deprivation Therapy (ADT), prostate cancer tumors can progress and may remain androgen sensitive These tumors utilize additional sources of androgen, including androgen produced by the adrenal glands and the tumor tissue itself Vis AN et al. BJU Int. 2009;104: Chen Y et al. Lancet Oncol 2009; 10(10): Denmeade SR, Isaacs JT. Nat Rev Cancer. 2002;2:
 responsive pathways. Driven by circulating testosterone. In 1941, Huggins & Hodges first proved that reducing androgen concentrations in prostate cancer patients leads to: Regression of tumours. Relief of cancer symptoms. CRPC Is an Androgen-Sensitive Disease. Despite castration levels of androgen after Androgen Deprivation Therapy (ADT), prostate cancer tumors can progress and may remain androgen sensitive. These tumors utilize additional sources of androgen, including androgen produced by the adrenal glands and the tumor tissue itself. Vis AN et al. BJU Int. 2009;104: Chen Y et al. Lancet Oncol 2009; 10(10): Denmeade SR, Isaacs JT. Nat Rev Cancer. 2002;2:")
4
Criteria of CRPC Castrate serum levels of testosterone <50 ng/dL , plus either: Biochemical progression: 3 consecutive ↑ of PSA, 1 week apart, resulting in two 50% increases over the nadir, Radiographic progression: The appearance of ≥ 2 lesions on bone scan or enlargement of a soft tissue lesions using RECIST (Response Evaluation Criteria in Solid Tumours) OR EAU Guidelines 2014
 OR. EAU Guidelines")
5
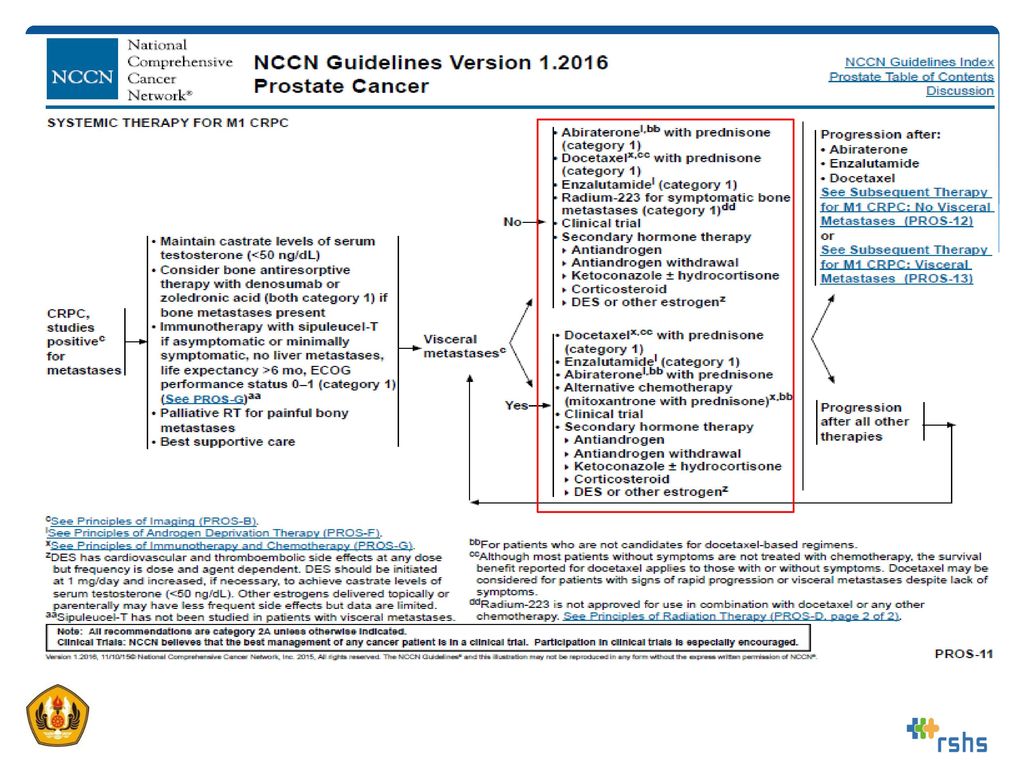
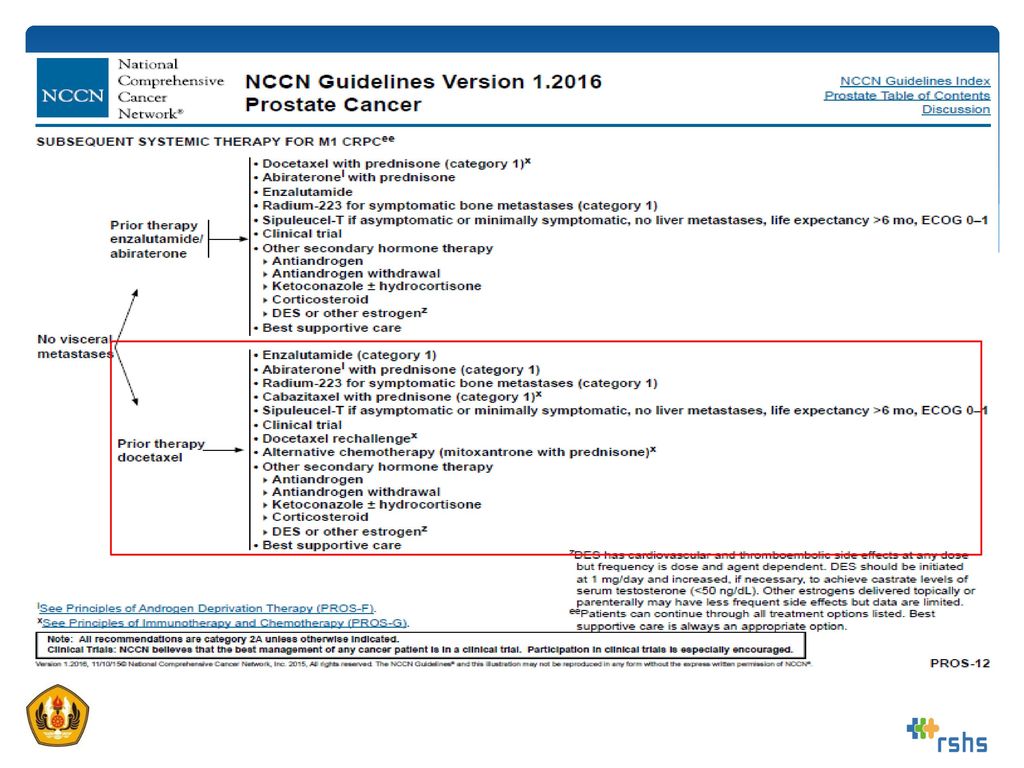
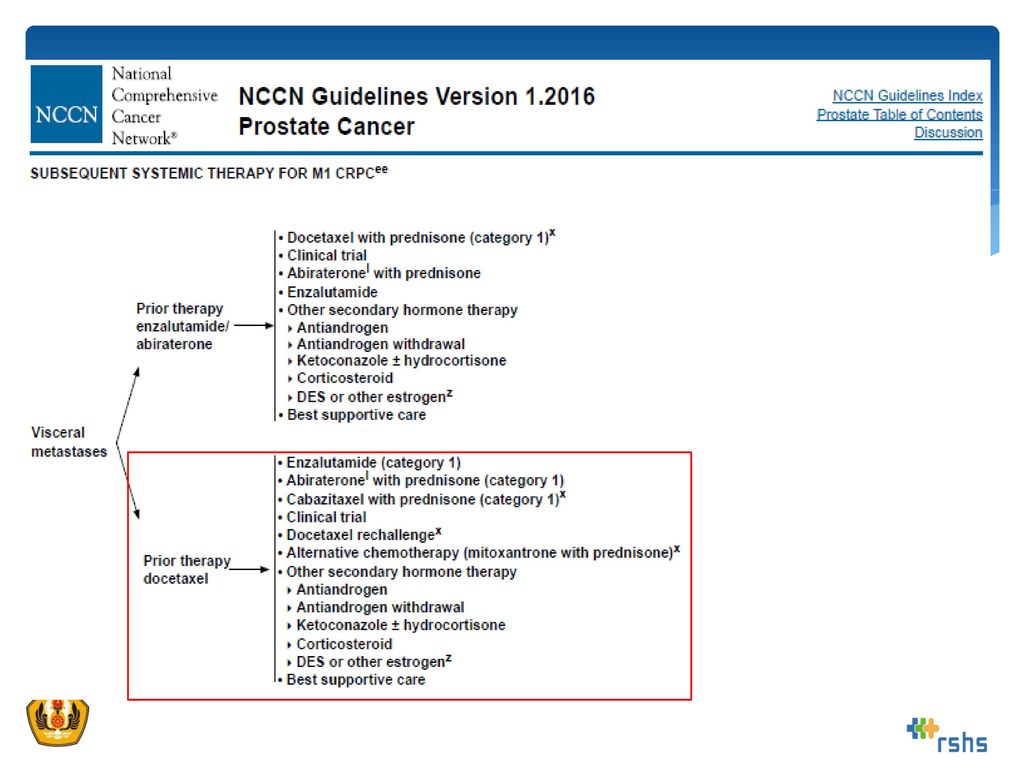
NCCN 2016 V. 1

9
EAU Guidelines of Prostate Cancer 2015

10
EAU Guidelines of Prostate Cancer 2015

11
EAU Guidelines of Prostate Cancer 2015

12
AUA Guidelines 2015

13
AUA Guidelines 2015

14
Panduan Penatalaksanaan CRPC di Indonesia
Kata Sambutan Kata Pengantar Daftar Isi Bab I. Pendahuluan I.1. Definisi Castrate Resistant Prostate Cancer I.2. Epidemiologi Castrate Resistant Prostate Cancer I.3. Patogenesis Castrate Resistant Prostate Cancer Bab II. Langkah Diagnostik Bab III. Klasifikasi Bab IV. Penatalaksanaan IV.1. Androgen Deprivation Therapy (ADT) IV.2. Pilihan Terapi Sistemik IV.3. Petunjuk Penatalaksanaan CRPC di Indonesia IV.4 Kesehatan Tulang Pada CRPC IV.5. Penatalaksanaan Metastasis Tulang IV.6. Terapi Paliatif IV.7. Pendekatan Tim Multidisiplin Spesialistik IV.8. Edukasi Pasien Bab V. Pemantauan V.1. Pemantauan Perkembangan Penyakit V.2. Pemantauan Efek Samping Obat dan Penanganannya KEPUSTAKAAN LAMPIRAN
 IV.2. Pilihan Terapi Sistemik IV.3. Petunjuk Penatalaksanaan CRPC di Indonesia IV.4 Kesehatan Tulang Pada CRPC IV.5. Penatalaksanaan Metastasis Tulang IV.6. Terapi Paliatif IV.7. Pendekatan Tim Multidisiplin Spesialistik IV.8. Edukasi Pasien Bab V. Pemantauan V.1. Pemantauan Perkembangan Penyakit V.2. Pemantauan Efek Samping Obat dan Penanganannya KEPUSTAKAAN LAMPIRAN")
15
Panduan Penatalaksanaan CRPC di Indonesia
Indeks Pasien Gejala Metastatik Kemoterapi Status Performa Penatalaksanaan 1 - Baik Rekomendasi: dilakukan observasi serta tetap diteruskan pemberian terapi ADT 2 -/minimal + Standard: (A) Abiraterone + prednisone, (B) docetaxel 3 Standard : Docetaxel. Rekomendasi: Abiraterone + prednisone 4 Buruk Pilihan: dengan Abiraterone + prednisone, atau Ketoconazole + steroid, atau terapi radionuklida 5 Standard: Abiraterone acetate + prednisone, atau Cabazitaxel 6 Pendapat ahli: terapi paliatif abiraterone + prednisone, atau ketoconazole + steroid, atau terapi radionuklida
 Abiraterone + prednisone, (B) docetaxel. 3. Standard : Docetaxel. Rekomendasi: Abiraterone + prednisone. 4. Buruk. Pilihan: dengan Abiraterone + prednisone, atau Ketoconazole + steroid, atau terapi radionuklida. 5. Standard: Abiraterone acetate + prednisone, atau Cabazitaxel. 6. Pendapat ahli: terapi paliatif abiraterone + prednisone, atau ketoconazole + steroid, atau terapi radionuklida.")
16
Penatalaksanaan untuk kelompok indeks pasien 1
Rekomendasi: dilakukan observasi serta tetap diteruskan pemberian terapi ADT. Pilihan: dengan anti androgen generasi pertama (seperti: flutamide, bicalutamide, dan nilutamide) atau dengan generasi pertama sintesis androgen inhibitor (ketoconazole di tambah steroid) diperuntukkan bagi pasien yang tidak ingin diobservasi saja.
 atau dengan generasi pertama sintesis androgen inhibitor (ketoconazole di tambah steroid) diperuntukkan bagi pasien yang tidak ingin diobservasi saja.")
17
Penatalaksanaan untuk kelompok indeks pasien 2
Standard: (A) Abiraterone + prednisone, (B) docetaxel, atau (B) Sipuleucel-T Pilihan: generasi pertama anti androgen, ketoconazole + steroid atau dilakukan observasi pada pasien yang tidak ingin atau tidak dapat menerima salah satu dari terapi standar.
 Abiraterone + prednisone, (B) docetaxel, atau (B) Sipuleucel-T. Pilihan: generasi pertama anti androgen, ketoconazole + steroid atau dilakukan observasi pada pasien yang tidak ingin atau tidak dapat menerima salah satu dari terapi standar.")
18
Penatalaksanaan untuk kelompok indeks pasien 3
Standard : Docetaxel. Rekomendasi: Abiraterone + prednisone. Pilihan: (C) Ketoconazole + steroid, (B) mitoxantrone atau (C) terapi radionuklida pada pasien yang tidak ingin atau tidak dapat diberi terapi standard.
 Ketoconazole + steroid, (B) mitoxantrone atau (C) terapi radionuklida pada pasien yang tidak ingin atau tidak dapat diberi terapi standard.")
19
Penatalaksanaan untuk kelompok indeks pasien 4
Pilihan: dengan Abiraterone + prednisone, atau Ketoconazole + steroid, atau terapi radionuklida Pendapat ahli: Docetaxel atau kemoterapi mitoxantrone pada pada kasus tertentu,

20
Penatalaksanaan untuk kelompok indeks pasien 5
Standard: Abiraterone acetate + prednisone, atau Cabazitaxel. Pilihan: Ketoconazole + steroid, atau terapi ulang dengan Docetaxel

21
Penatalaksanaan untuk kelompok indeks pasien 6
Pendapat ahli: terapi paliatif abiraterone + prednisone, atau ketoconazole + steroid, atau terapi radionuklida.

22
Consensus recommendation about monitoring and discontinuation of a treatment

23
The panel included 41 prostate cancer experts from 17 countries, covering different specialties involved in research and treatment of men with APC Gillessen S, et al. Annals of Oncol 2015

24
Multidiscplinary specialists as panelist
Gillessen S, et al. Annals of Oncol 2015

25
Highlight of #7 recommendation about monitoring and discontinuation of a treatment
Gillessen S, et al. Annals of Oncol 2015

26
Gillessen S, et al. Annals of Oncol 2015

27
Choose the Right Treatment for the Right Patient at the Right Time
TAKE HOME MESSAGES Choose the Right Treatment for the Right Patient at the Right Time

28
Thank you

Presentasi serupa


 pada Radiology Information System (RIS)>")






. Jenis Perancangan Riset Jenis perancangan mana yg akan digunakan ? Peneliti perlu memikirkan tentang apa yang mereka inginkan.>")
 array stack dan queue>")








