Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
Patient safety Sharon Gondodiputro dr., MARS, MH
Department of Public Health,Faculty of Medicine UNPAD

2
Topics Definition patient safety Definition of error
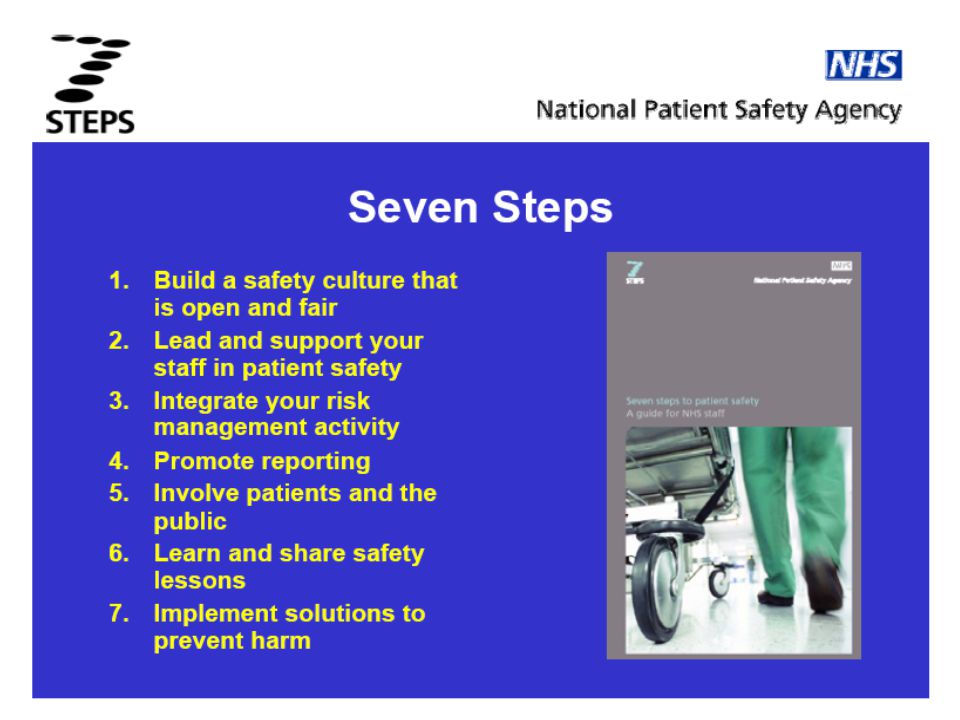
Human factors in patient safety Problem solving cycle in patient safety 7 steps of patient safety

3
Definition WHO, A discipline in the health-care sector that :
applies safety science methods towards the goal of achieving a trustworthy system of health-care delivery an attribute of health-care systems it minimizes the incidence and impact of and maximizes recovery from adverse events Permenkes 1691 : suatu sistem dimana rumah sakit membuat asuhan pasien lebih aman yang meliputi: asesmen risiko, identifikasi dan pengelolaan hal yang berhubungan dengan risiko pasien, pelaporan dan analisis insiden, kemampuan belajar dari insiden dan tindak lanjutnya serta implementasi solusi untuk meminimalkan timbulnya risiko dan mencegah terjadinya cedera yang disebabkan oleh kesalahan akibat melaksanakan suatu tindakan atau tidak mengambil tindakan yang seharusnya diambil.

4
Definisi Insiden (Permenkes 1691)
setiap kejadian yang tidak disengaja dan kondisi yang mengakibatkan atau berpotensi mengakibatkan cedera yang dapat dicegah pada pasien Kejadian Tidak Diharapkan, (KTD) : insiden yang mengakibatkan cedera pada pasien Kejadian Nyaris Cedera (KNC) : terjadinya insiden yang belum sampai terpapar ke pasien. Kejadian Tidak Cedera (KTC ): insiden yang sudah terpapar ke pasien, tetapi tidak timbul cedera. Kondisi Potensial Cedera (KPC): kondisi yang sangat berpotensi untuk menimbulkan cedera, tetapi belum terjadi insiden Kejadian sentinel : KTD yang mengakibatkan kematian atau cedera yang serius.
 : insiden yang mengakibatkan cedera pada pasien. Kejadian Nyaris Cedera (KNC) : terjadinya insiden yang belum sampai terpapar ke pasien. Kejadian Tidak Cedera (KTC ): insiden yang sudah terpapar ke pasien, tetapi tidak timbul cedera. Kondisi Potensial Cedera (KPC): kondisi yang sangat berpotensi untuk menimbulkan cedera, tetapi belum terjadi insiden. Kejadian sentinel : KTD yang mengakibatkan kematian atau cedera yang serius.")
5
Human factors design principles
Psychomotor Hands Input Devices Buttons INTERFACE Senses - Vision Hearing Output - Display Sound This slide illustrates how we interact with equipment - and indeed human factors engineering is in part the study of the human machine interaction. But actually this slide represents how we interact with everything - using our eyes, ears, fingers, hands … Our senses take in inputs, then we rely on our memory and knowledge to process the information and then make decisions and formulate a response HFE recognizes that we can make errors at each step of this process … US Department of Veteran affairs

6
Traps in health care? look-alike and sound-alike pharmaceuticals
equipment design e.g. infusion pumps

17
Ruang ICU

21
What is an error? A definition that may be easier to remember is:
the failure of a planned action to achieve its intended outcome a deviation between what was actually done and what should have been done Reason A definition that may be easier to remember is: “Doing the wrong thing when meaning to do the right thing.” All common situations for inexperienced staff.

22
Situations associated with an increased risk of error
unfamiliarity with the task* inexperience* shortage of time inadequate checking poor procedures poor human equipment interface Vincent All common situations for inexperienced staff. * Especially if combined with lack of supervision

23
Individual factors that predispose to error
limited memory capacity further reduced by: fatigue stress hunger illness language or cultural factors hazardous attitudes

24
Don’t forget …. If you’re H ungry A ngry L ate or T ired ….. H A L T

25
A performance-shaping factors “checklist”
Here is a useful acronym to consider prior to entering the workplace each day. It is borrowed (surprise, surprise) from the aviation industry! Jensen, 1987
 from the aviation industry! Jensen,")
26
Sistem Pelayanan Kesehatan di Rumah Sakit
Comsumption of resources How the process of health services Who receive health care Who provide health care Feedback dan TQM

27
1. Measuring harm (mengukur insiden)
2. Understanding causes (mengerti/mencari penyebab) 3.Identify solution (Identifikasi solusi) 4.Evaluating Impact (evaluasi impact) 5.Translating Evidence into safer care (pelaksanaan dan perencanaan kembali)
 3.Identify solution (Identifikasi solusi) 4.Evaluating Impact (evaluasi impact) 5.Translating Evidence into safer care (pelaksanaan dan perencanaan kembali)")
28
1. Measuring harm Sasaran Keselamatan Pasien
Ketepatan identifikasi pasien: dua identitas atau penggunaan gelang pasien Peningkatan komunikasi yang efektif: persentase kelengkapan rekam medik,audit klinik/keperawatan Peningkatan keamanan obat yang perlu diwaspadai: persentase pemberian obat yang salah Kepastian tepat-lokasi, tepat-prosedur, tepat-pasien operasi: persentase penandaan lokasi operasi Pengurangan risiko infeksi terkait pelayanan kesehatan: persentase tertusuk jarum, ILO, ISK, pneumonia, cuci tangan yang benar Pengurangan risiko pasien jatuh: lantai licin,penggunaan tempat tidur berpagar, asessment pasien risiko jatuh

29
Reason’s swiss model: Multiple factors usually involved
2. Understand causes Reason’s swiss model: Multiple factors usually involved

30
Vincent funnel : Multiple factors usually involved
environmental factors team factors technology and tool task factors provider patient organizational factors

31
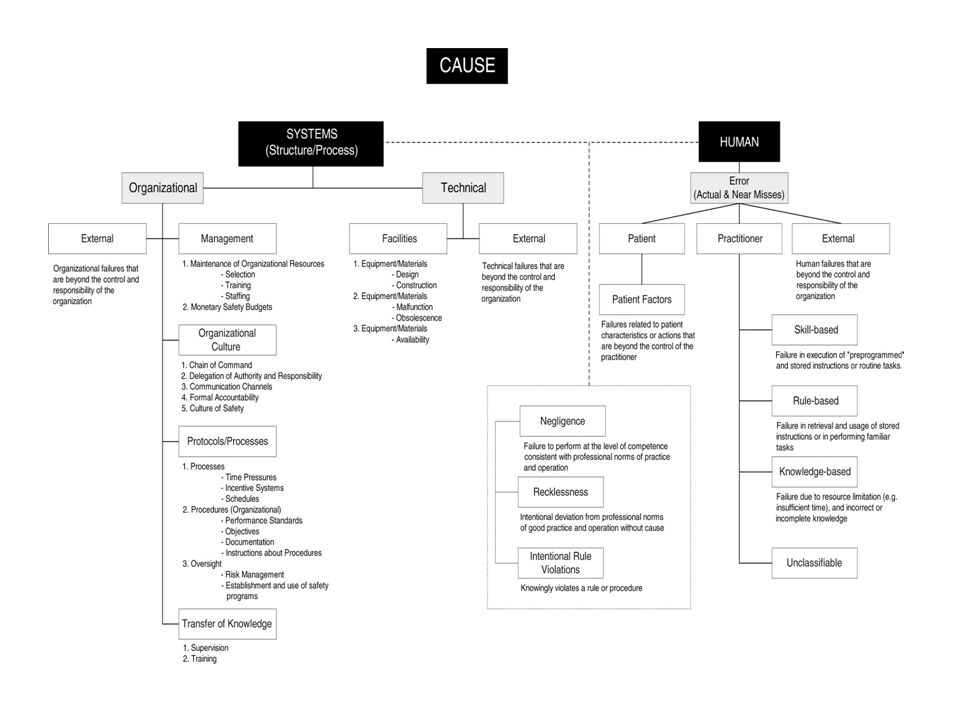
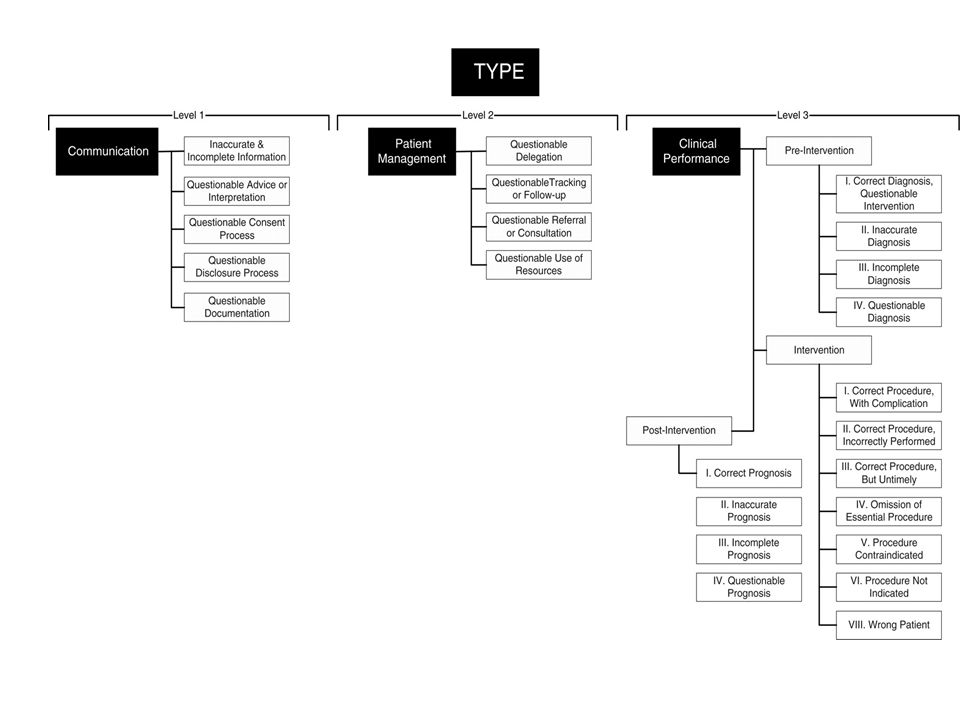
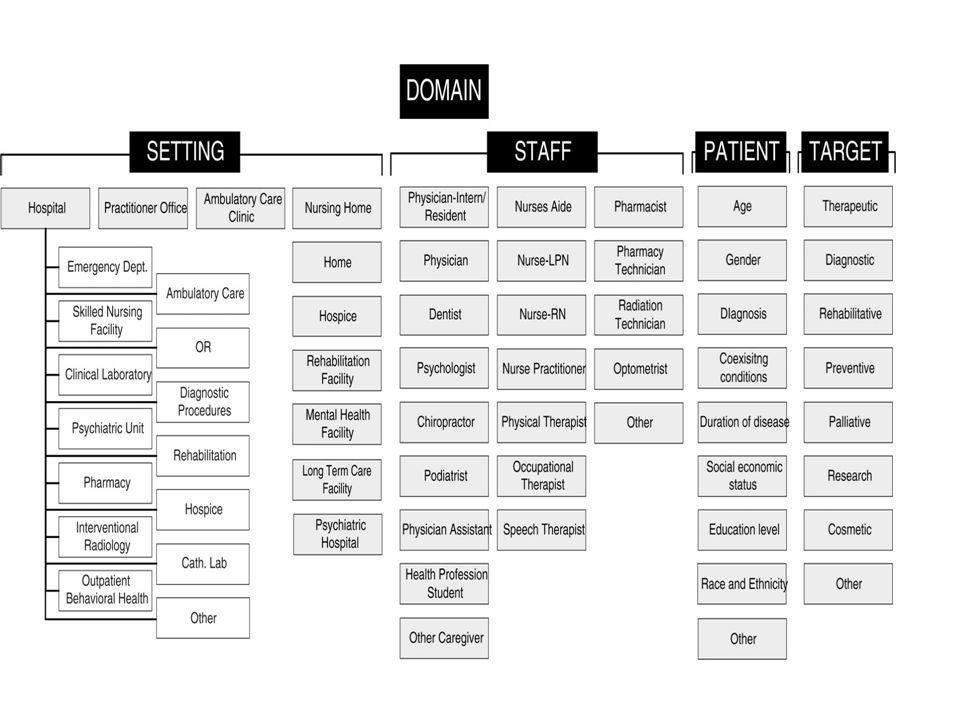
Cause Type Domain Impact Level 1: communication
Level 2: patient management Level 3: Clinical performance pra, durante dan post intervention Cause Type Impact Domain Organizational/technical factor Human factor Medical :fisik,psikis Nonmedical: legal, economy,social Setting/location Staff Patient Target

36
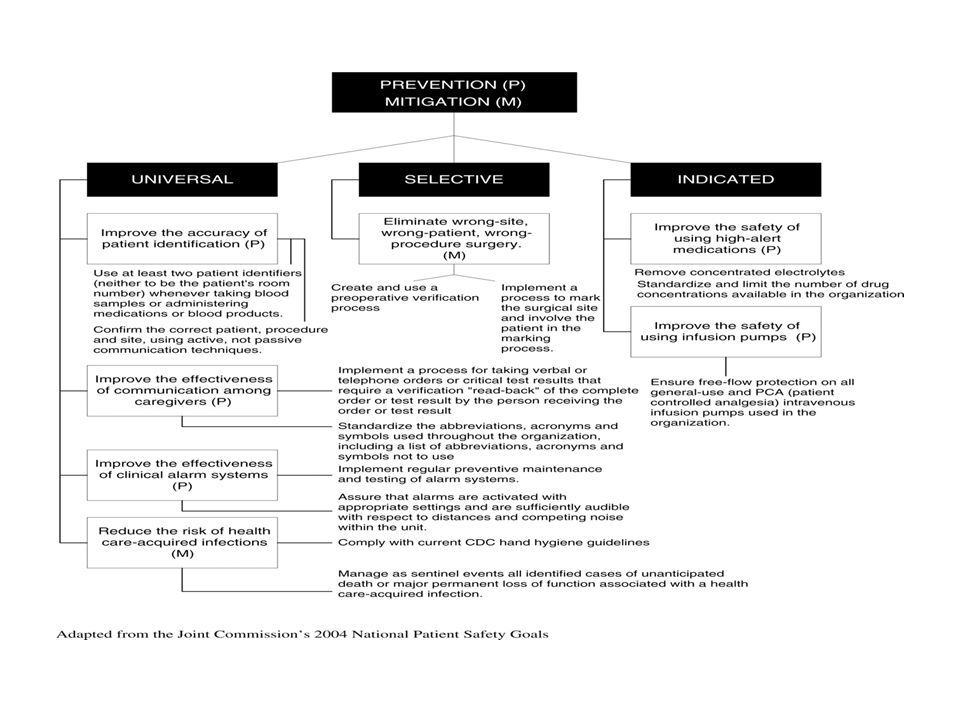
Preventive/Mitigation
3. Identify Solution Causes Type Impact Domain Preventive/Mitigation Universal Selective Indication

38
1. Measuring harm (mengukur insiden)
2. Understanding causes (mengerti/mencari penyebab) 3.Identify solution (Identifikasi solusi) 4.Evaluating Impact (evaluasi impact) 5.Translating Evidence into safer care (pelaksanaan dan perencanaan kembali)
 3.Identify solution (Identifikasi solusi) 4.Evaluating Impact (evaluasi impact) 5.Translating Evidence into safer care (pelaksanaan dan perencanaan kembali)")
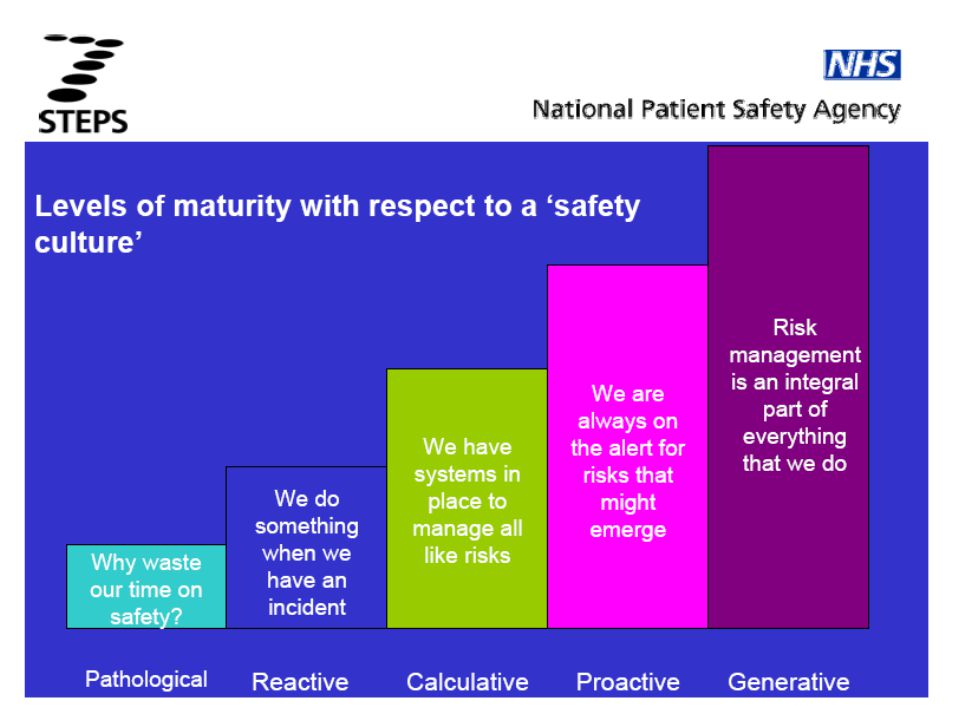
41
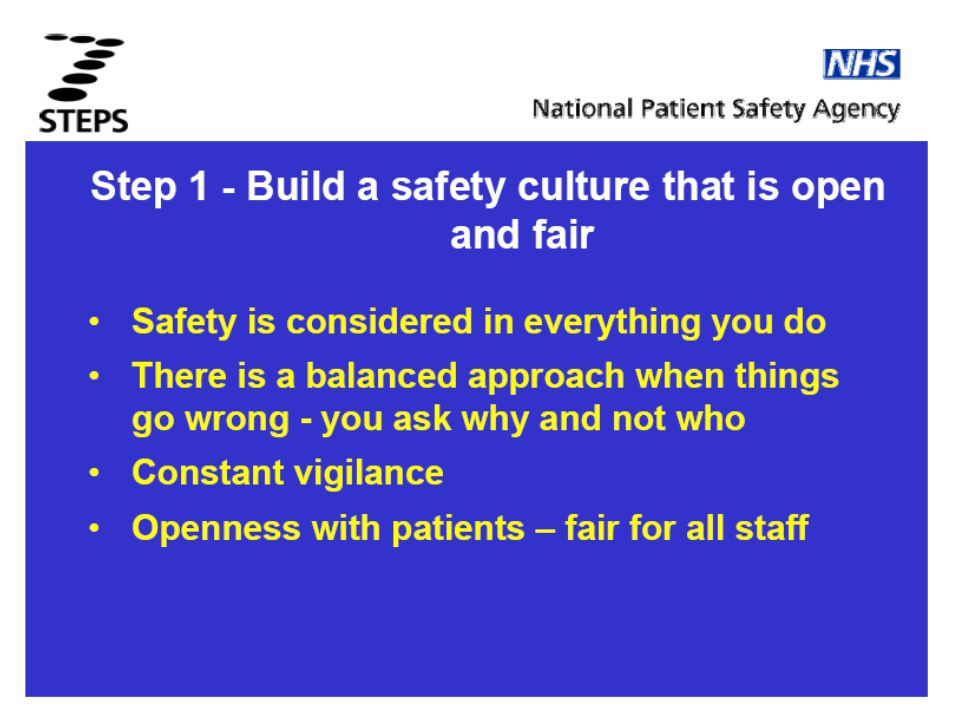
A safety culture is where organisations, practices, teams and individuals have a constant and active awareness of the potential for things to go wrong. Both the individuals and the organisation are able to acknowledge mistakes, learn from them, and take action to put things right. Being open and fair means sharing information openly and freely with patients and their families, balanced by fair treatment for staff when an incident happens. This is vital for both the safety of patients and the wellbeing of those who provide their care.

Presentasi serupa


















>")
>")
 pada Radiology Information System (RIS)>")











