Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
ERITROPAPULO SKUAMOSA DERMATOSIS

2
ERITROPAPULOSKUAMOSA DERMATOSIS
Golongan penyakit kulit Effloresensi terutama : eritema, papula, skuama Penyebab diketahui : Dermatomikosis superfisialis Lues II MH Penyebab tak diketahui : Psoriasis vulgaris Pytiriasis rosea Dermatitis seboroik Lichen planus Pityriasis Rubra Pilaris

3
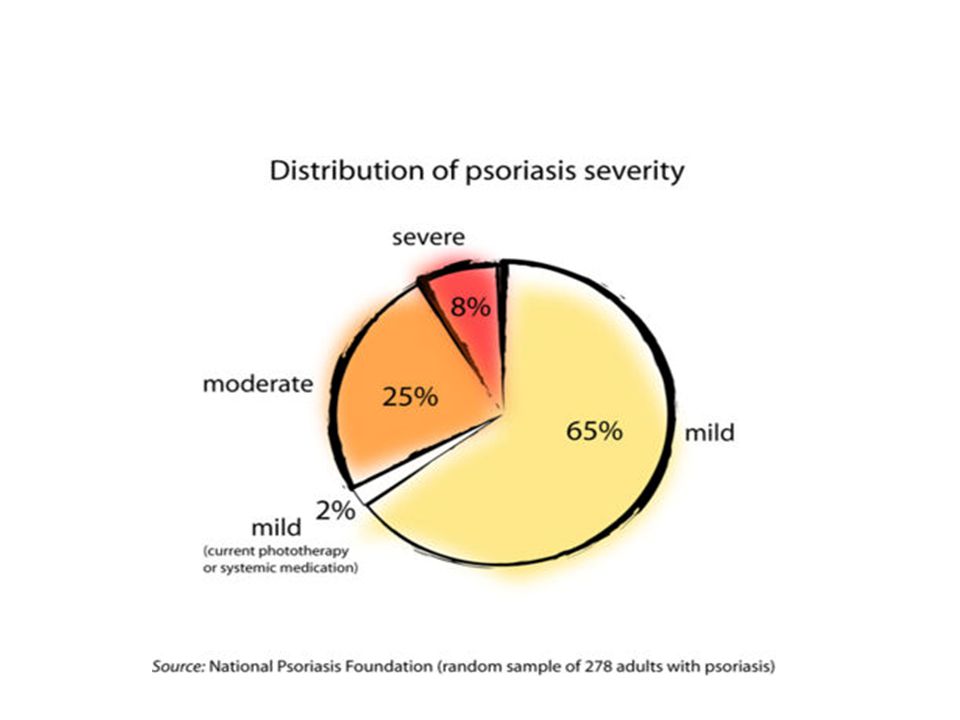
PSORIASIS VULGARIS DEFINISI : penyakit kulit, kronis dan residif
makula eritematus bulat / lonjong skuama tebal, transparan/putih keabu-abuan

4
ETIOLOGI DAN PATOFISIOLOGI
Penyebab pasti tak diketahui Faktor-faktor : Pemendekan turn over epidermis Predisposisi genetik Faktor pencetus : - infeksi - obat tertentu - stres - perubahan iklim trauma EPIDEMIOLOGI Semua usia, dewasa >> Pria = wanita

5
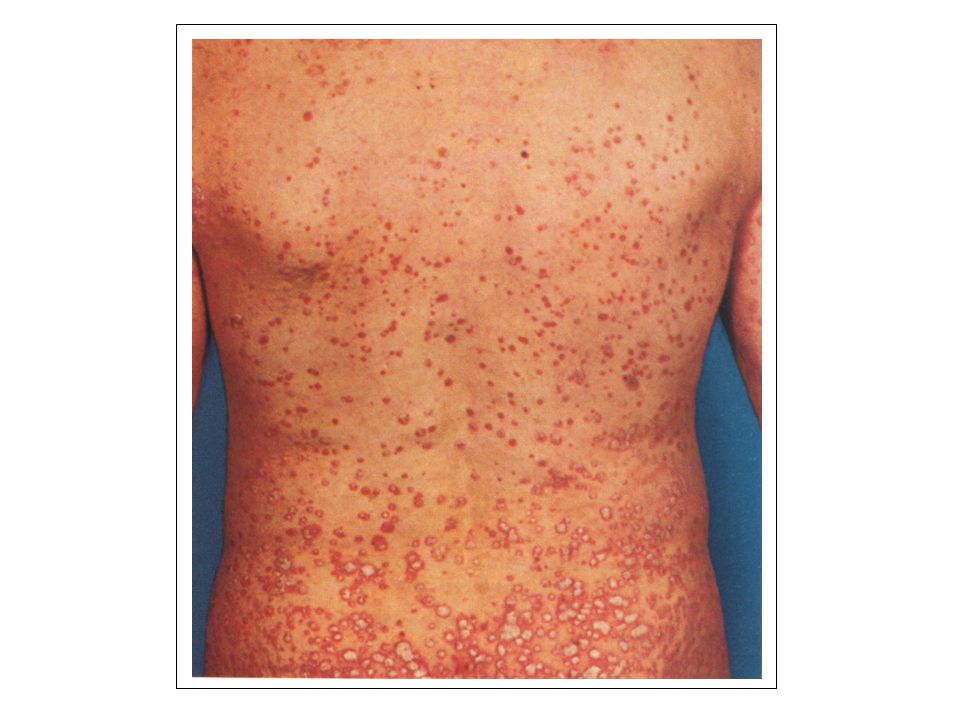
GEJALA KLINIS Keluhan - sedikit gatal (panas / burning sensation)
- kosmetik. Kulit Makula eritematus, batas jelas, tertutup skuama tebal, transparan, lepas dibagian tepi, lekat dibagian tengah. Kaarsvlek phen (+), Austpitz sign (+), Koebner phen (+) Bentuk makula bisa berubah anular, gyrata, folikular, gutata, punctata
, Austpitz sign (+), Koebner phen (+) Bentuk makula bisa berubah anular, gyrata, folikular, gutata, punctata.")
6
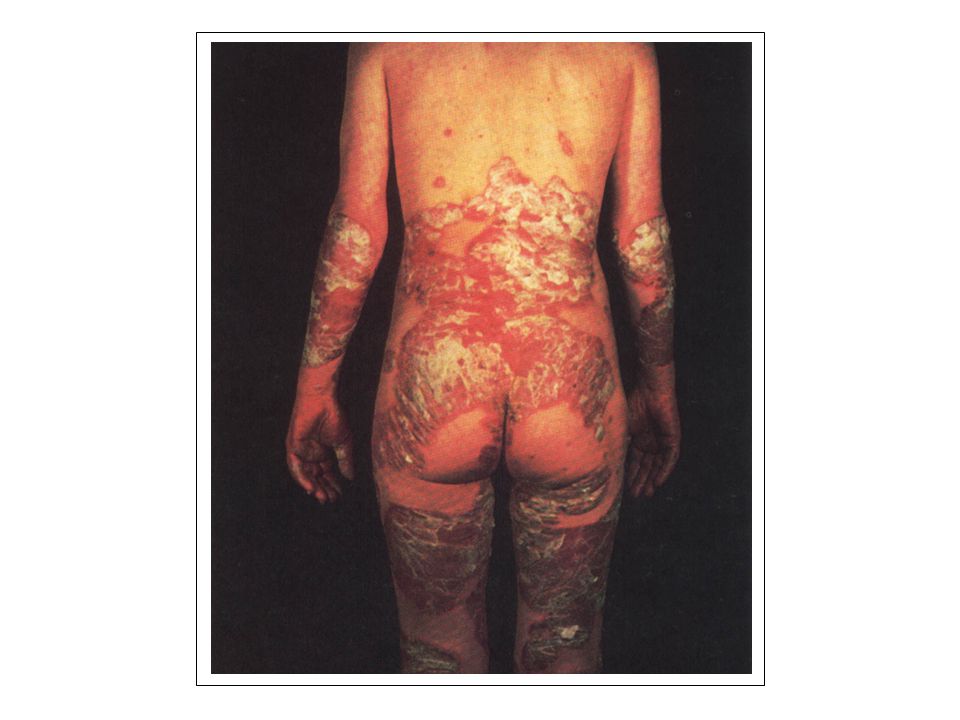
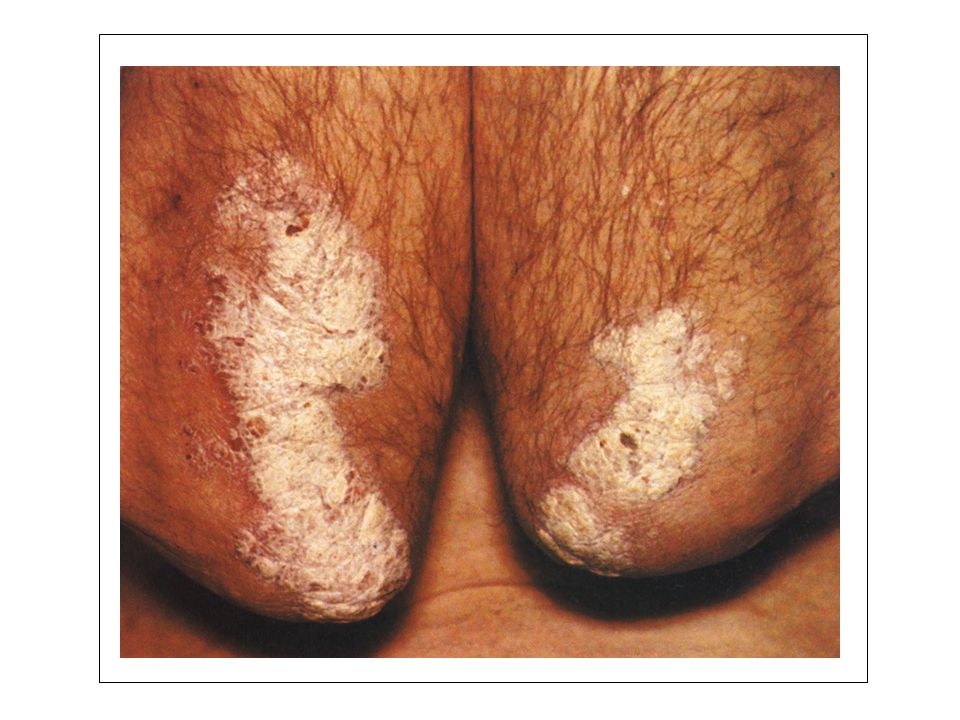
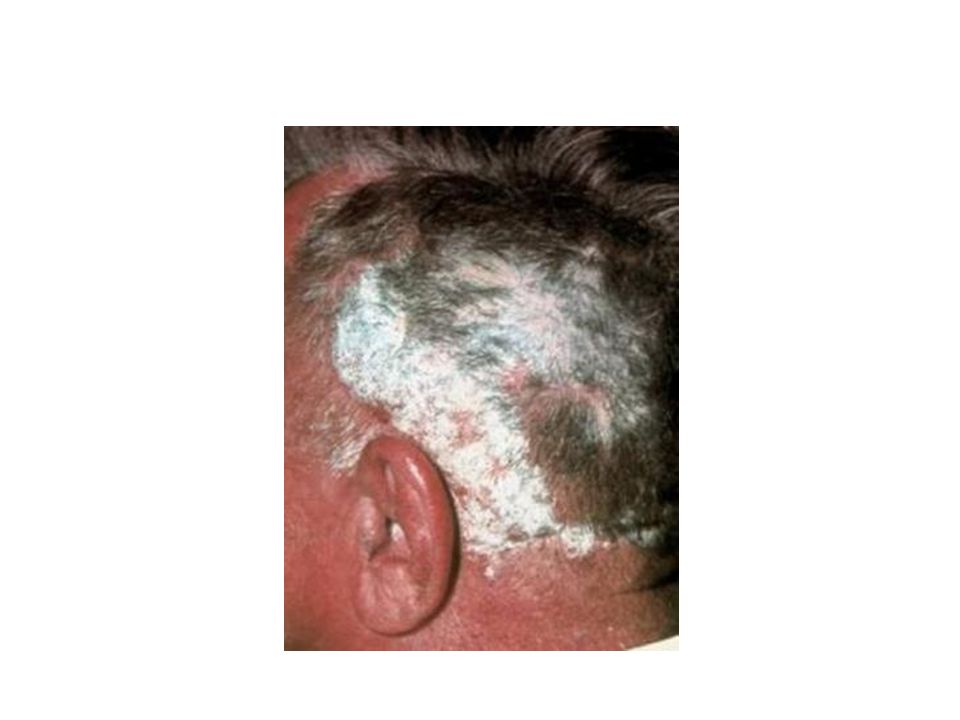
PREDILEKSI Tempat mudah kena trauma ( siku, lutut, sakrum, kepala, genitalia)
")
7
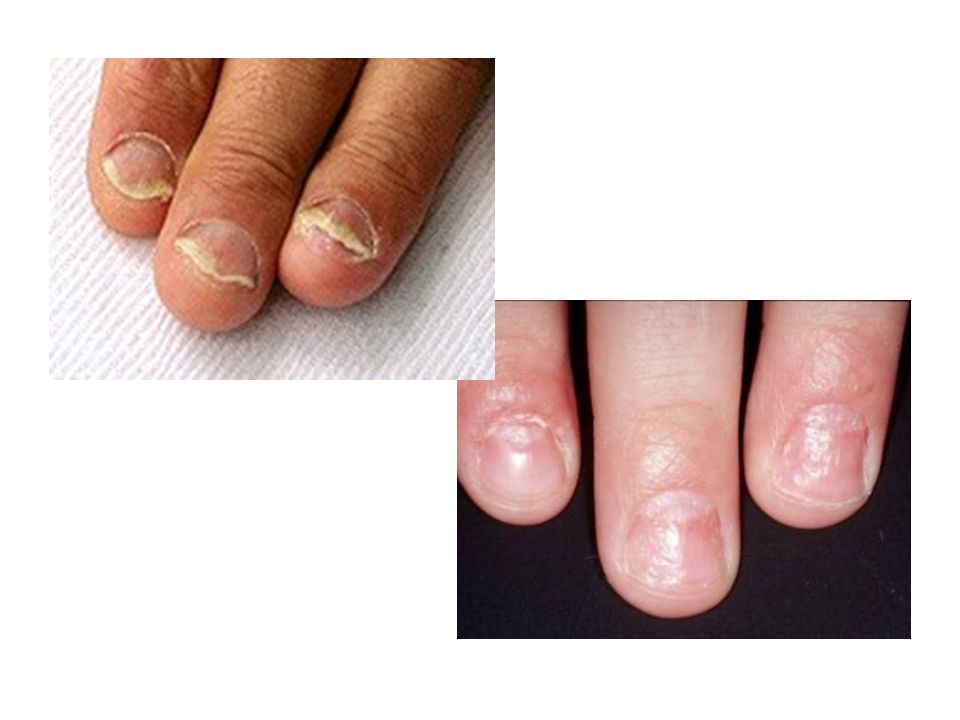
Kuku : keruh, pitting, punctate subungual hiperkeratosis kuku tangan >> Mukosa : geographic tongue Sendi : Psoriasis arthropatica (interphalang dan lumbosacral)
")
9
HISTOPATOLOGI - Khas, diagnosis pasti
Hiperkeratosis, parakeratosis,akantosis, pemanjangan Rete ridges, permanjangan papila dermis, mitosis dari stratum basalis, mikro abses Munro

10
DIAGNOSIS DIAGNOSIS BANDING klinis dan histoPA MH type T Lues II
DIAGNOSIS BANDING MH type T Lues II Dermatomikosis superfisialis Dermatitis seboroik Pytiriasis Rosea

25
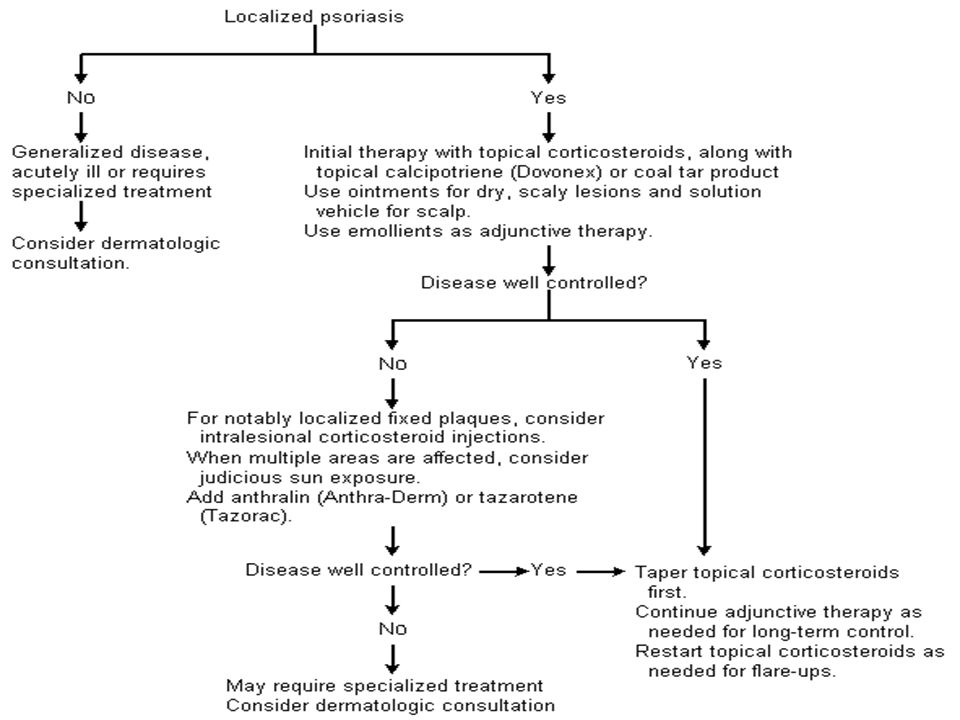
PENYULIT PENATALAKSANAAN Eritrodermi kausal (-)
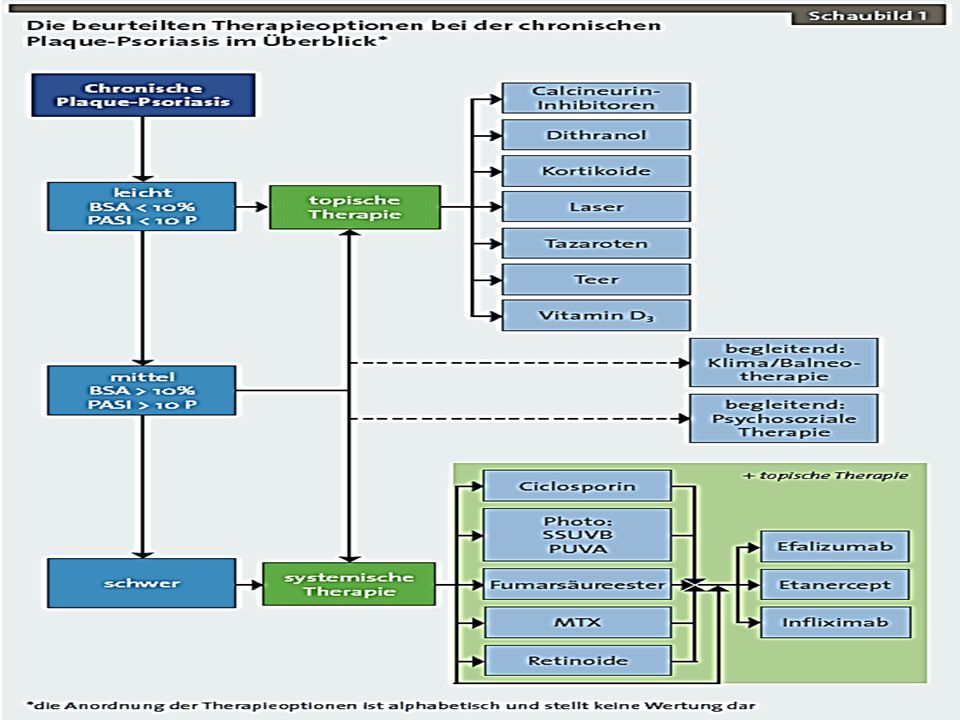
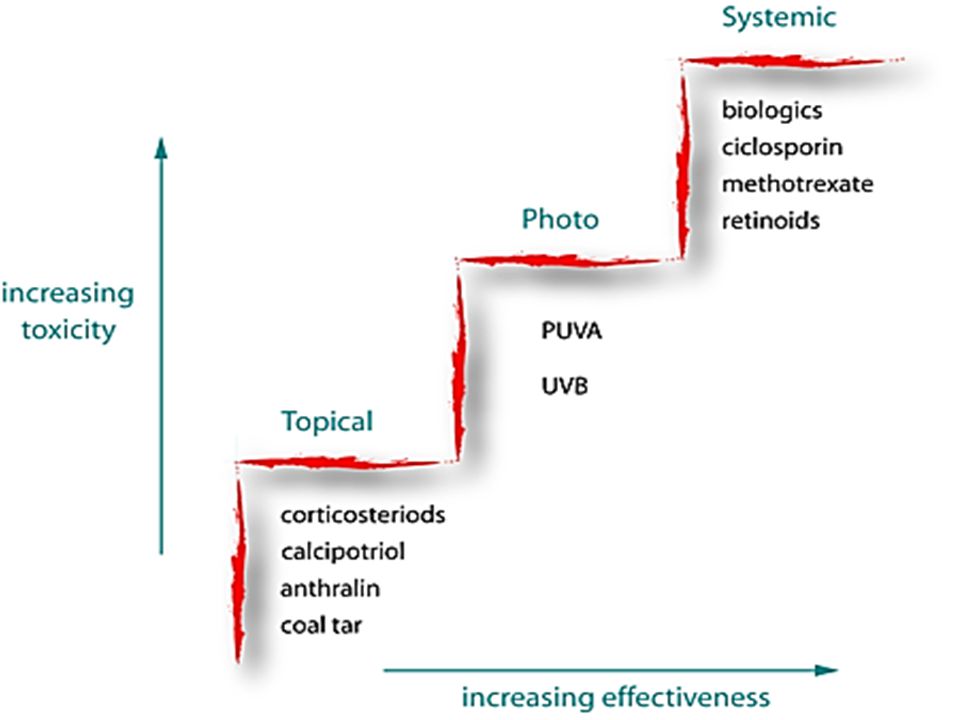
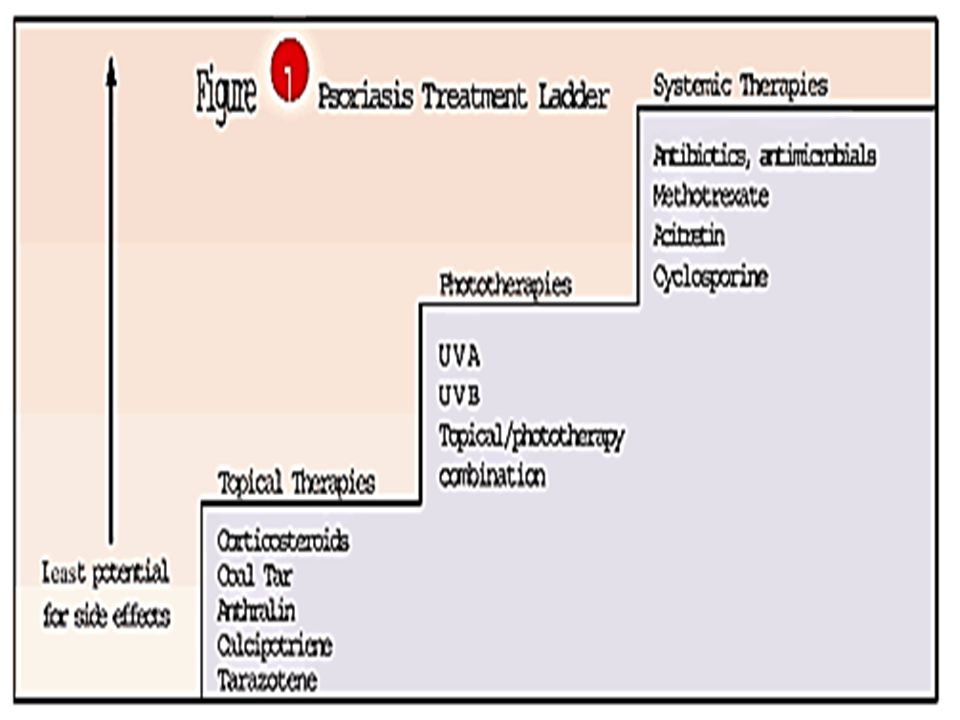
PENATALAKSANAAN kausal (-) tujuan : menghilangkan faktor pencetus/lesi topikal : kortikosteroid, tar, anthralin, vit D, asidum salisilikum. sistemik : metotrexate, retinoid, fototerapi
 tujuan : menghilangkan faktor pencetus/lesi. topikal : kortikosteroid, tar, anthralin, vit D, asidum salisilikum. sistemik : metotrexate, retinoid, fototerapi.")
29
Generalisata (von Zumbusch)
PSORIASIS PUSTULOSA Dibagi 2 : Palmo plantar Generalisata (von Zumbusch) Dengan atau tanpa didahului Psoriasis Vulgaris Klinis : Febris tingi, KU lemah Eritema menyebar luas ditumpangi adanya pustule steril. Pustule bisa bergabung membentuk danau-danau yang berisi pus. Laboratorium : Leukositosis (DL) PMN >> dan pustule steril tidak didapatkan bakteri (Gram) Terapi : MTX, Siklosporin, Asitretin, Kosrtikoseroid oral
 Dengan atau tanpa didahului Psoriasis Vulgaris. Klinis : Febris tingi, KU lemah. Eritema menyebar luas ditumpangi adanya pustule steril. Pustule bisa bergabung membentuk danau-danau yang berisi pus. Laboratorium : Leukositosis (DL) PMN >> dan pustule steril tidak didapatkan bakteri (Gram) Terapi : MTX, Siklosporin, Asitretin, Kosrtikoseroid oral.")
31
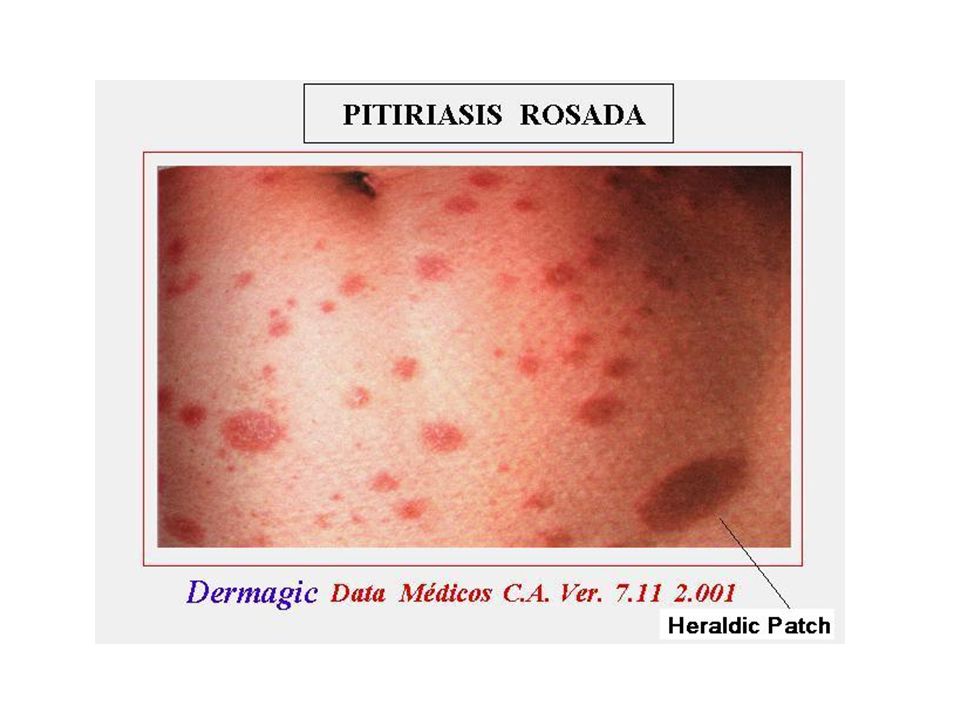
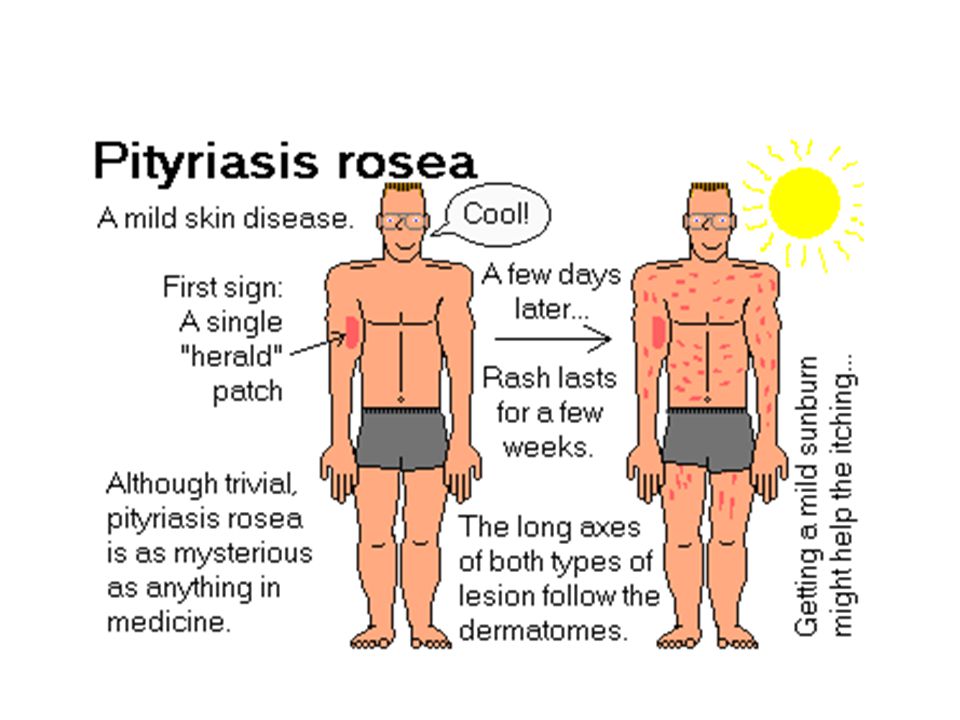
PITYRIASIS ROSEA DEFINISI penyakit kulit, ringan, swasirna
makulae eritematus, oval, papulae, plak skuama disekeliling tepinya ETIOLOGI DAN PATOFISIOLOGI penyebab pasti belum diketahui diduga ~ infeksi virus

32
Pityriasis rosea is common self-limited benign papulosquamous dermatosis associated with distinctive clinical features. "Herald patch" followed by a widespread oval scaly red eruptions. A viral etiology has been suggested ( human herpesvirus-7 and 6).
.")
33
usia remaja, dewasa muda >> pria = wanita PREDILEKSI
PITYRIASIS ROSEA EPIDEMIOLOGI usia remaja, dewasa muda >> pria = wanita PREDILEKSI bagian tubuh tertutup pakaian, leher – dagu kadang bagian tubuh terbuka Pityriasis Rosea Inversa

34
gatal ringan - sedang / asimtomatik
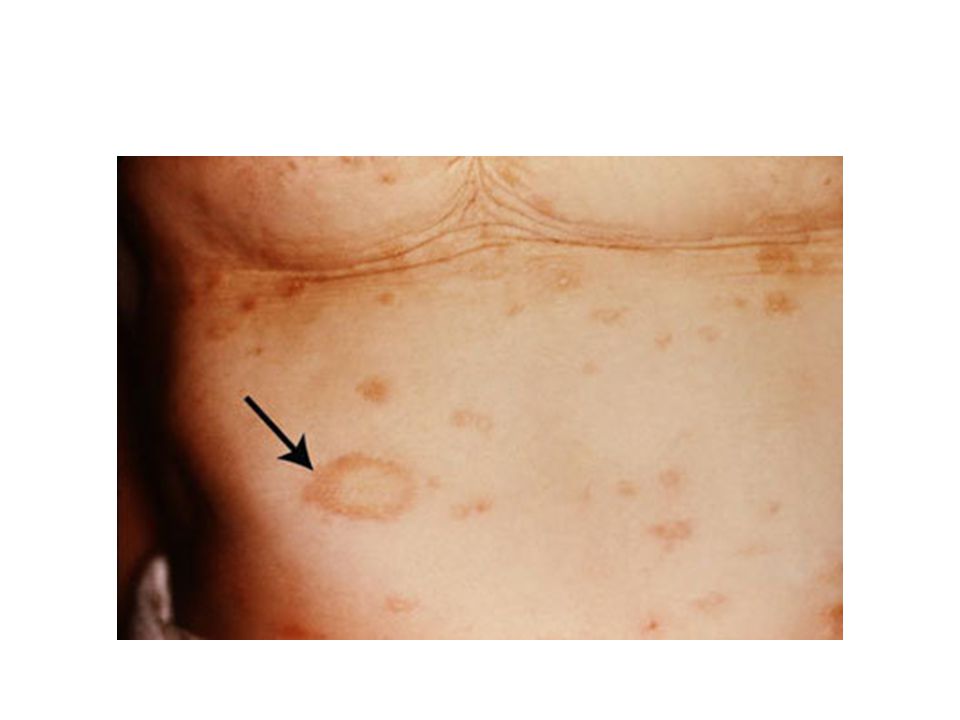
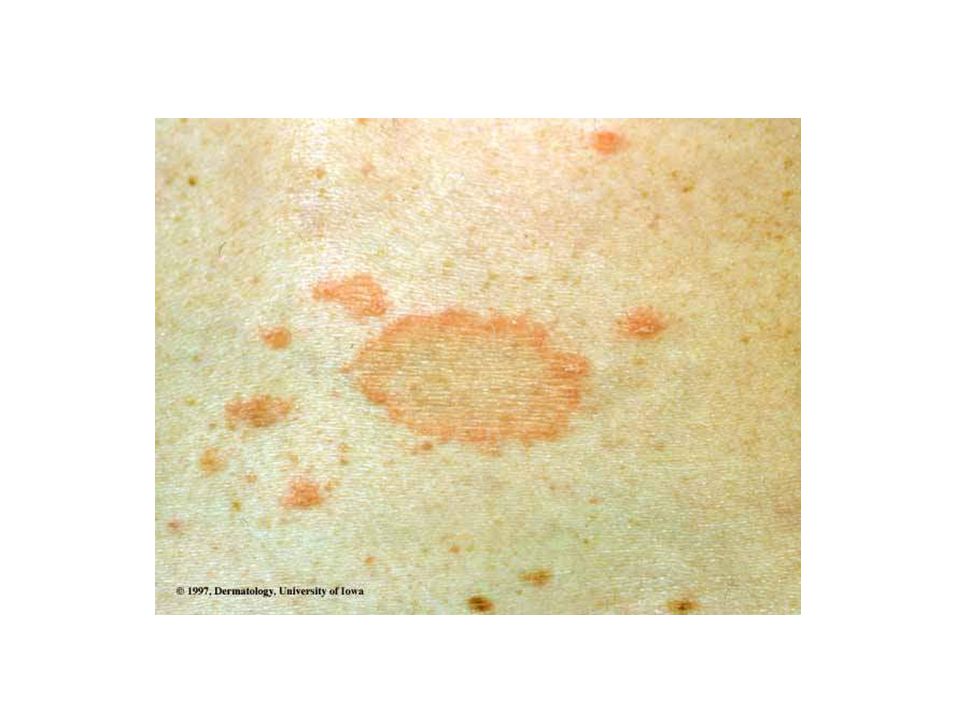
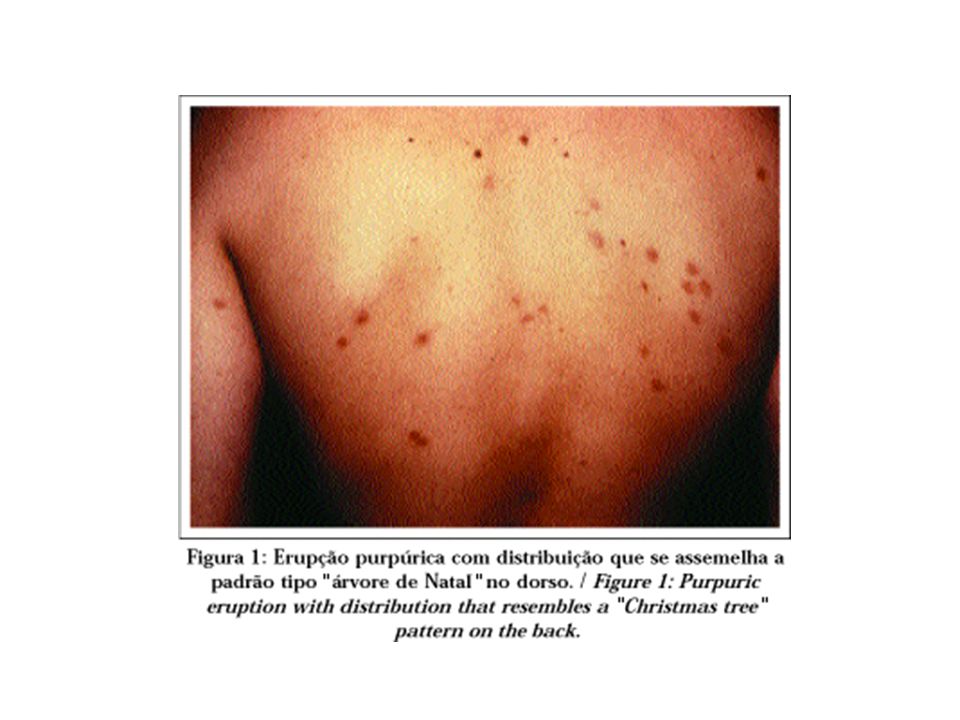
PITYRIASIS ROSEA GEJALA KLINIS gejala konstitusi gatal ringan - sedang / asimtomatik herald patch / mother plaque / medalion makulae bulat lonjong, tepi meninggi, lekat pd tepi sumbu panjang sejajar pelipatan kulit dipunggung ~ gambaran pohon cemara. HISTOPATOLOGI akantosis ringan, parakeratosis fokal infiltrat limfosit, perivaskular ringan

35
DIAGNOSIS Klinis khas DIAGNOSIS BANDING Psoriasis vulgaris
PITYRIASIS ROSEA DIAGNOSIS Klinis khas DIAGNOSIS BANDING Psoriasis vulgaris Dermatitis seboroik Lues II Tinea corporis - MH

36
Bedak mengandung asidum salicilikum
PITYRIASIS ROSEA PENATALAKSANAAN Tx spesifik (-) Antihistamin Bedak mengandung asidum salicilikum Steroid topikal / sistemik bila parah Konseling
 Antihistamin. Bedak mengandung asidum salicilikum. Steroid topikal / sistemik bila parah. Konseling.")
46
Pityriasis Rosea, or "PR" for short, is a skin problem of unknown origin. It behaves somewhat like a virus, since most people get it once in their lives and never again. No one has been able to find an infection agent in most cases studied. Several years ago, some researchers found a virus-like particle in some skin biopsies. Pityriasis rosea is: A. A NUISANCE B. SELF-LIMITING C. NON-SCARRING (as long as you don't scratch a lot) D. NOT SERIOUS E. NOT DUE TO SOMETHING YOU ATE F. NOT AIDS G. NOT VITAMIN DEFICIENCY H. NOT ANY FORM OF CANCER I. NOT CONTAGIOUS There is no need to sterilize your dishes or glasses. You do not have to wash your towels and linens separately from everyone else, and you do NOT have to isolate yourself from anyone else. Typical "PR" is characterized by 1-2 centimeter sized oval spots, usually somewhat pink to red, with a little "collar" or scaling. A "herald patch" that is larger than all the rest comes first in around 50% of cases, and is usually followed by a shower of smaller ones in several days. They are usually located on your trunk in the folds of the skin. They do NOT usually involve the face, palms or soles. Unusual cases of "PR" have fine red bumps, about the size of a mosquito bite, in clusters and patches on the body, face, under arms, in the groin, and sometimes on your palms. These bumps also develop those little collars of scale over time. TREATMENT: Typically, a course of "PR" will take 2-3 months to clear if no therapy is used. Erythromycin seems to help in some cases, may be prescribed and may shorten your course to weeks instead of months. Topical cortisones also help for symptomatic relief of your itching. Sometimes cortisone injections are given in the buttocks to shorten the course. Going to the beach and getting into the cool water, and simultaneously getting some sun may also help. Ultraviolet light does shorten the course. Heat aggravates the itching, so stay cool. Good old- fashioned calamine lotion also seems to help. Apply it with a paint brush. © 2006 Pacific Monograph
 D. NOT SERIOUS E. NOT DUE TO SOMETHING YOU ATE F. NOT AIDS G. NOT VITAMIN DEFICIENCY H. NOT ANY FORM OF CANCER I. NOT CONTAGIOUS There is no need to sterilize your dishes or glasses. You do not have to wash your towels and linens separately from everyone else, and you do NOT have to isolate yourself from anyone else. Typical PR is characterized by 1-2 centimeter sized oval spots, usually somewhat pink to red, with a little collar or scaling. A herald patch that is larger than all the rest comes first in around 50% of cases, and is usually followed by a shower of smaller ones in several days. They are usually located on your trunk in the folds of the skin. They do NOT usually involve the face, palms or soles. Unusual cases of PR have fine red bumps, about the size of a mosquito bite, in clusters and patches on the body, face, under arms, in the groin, and sometimes on your palms. These bumps also develop those little collars of scale over time. TREATMENT: Typically, a course of PR will take 2-3 months to clear if no therapy is used. Erythromycin seems to help in some cases, may be prescribed and may shorten your course to weeks instead of months. Topical cortisones also help for symptomatic relief of your itching. Sometimes cortisone injections are given in the buttocks to shorten the course. Going to the beach and getting into the cool water, and simultaneously getting some sun may also help. Ultraviolet light does shorten the course. Heat aggravates the itching, so stay cool. Good old- fashioned calamine lotion also seems to help. Apply it with a paint brush. © 2006 Pacific Monograph.")
47
Pityriasis Rosea My Diary ~Jim Spence ~If you are reading this, more than likely you have just found you that you have Pityriasis Rosea, or you know someone that does. You've probably been searching web sites, trying to find out anything you can about it, and you've noticed that there's a lot of information, some of it contradictive, but no clear cut ideas on what you can actually do about it. Of course, it's impossible to diagnose a disease on line; however, you can make informed decisions on the information that's available and try some things yourself to make this disease easier to deal with. You've probably seen the following information but, just in case you haven't, I'm going to go over some of the basics. Please know that I'm not a doctor; all I'm doing is compiling the information that I've gotten from dozens of web sites, a few books, and my own doctor. If you heed any advice that I give you and harm comes to you … shame on you. You should have known better. The main reason I'm compiling this information is … I had Pityriasis Rosea and cured it much quicker than the norm, in part, I think, because I did my homework. If you're lucky, you can cheat off of me. Pityriasis Rosea (pit' - e - RYE' - uh - sis RO' - sha) is caused by a virus. What kind of virus is unknown. A few web sites don't agree with this, but the overwhelming majority (and my personal physician) do, so that's what I'm going with. The virus enters your body in some unknown manner and manifests itself in a single spot, usually the size of a nickel, somewhere on your torso, though it can start other places on your body. In my case, it started on the back of my right thigh. This spot is called the herald patch. The entire rash that will take place over your body in the next few months comes from this spot. Sometime between one and 30 days later, you'll notice a rash forming on the trunk of your body. This rash takes the initial form of a typical bumpy rash, then changes to larger, wrinkled, pinker spots. The rash usually follows the creases in your skin … under your arms, the crease in your neck, around your navel, on your ribs. The disease, and it's referred to as a disease because it's viral in nature, is truncated … meaning that it usually stays on your torso, down to the shirt sleeve line on your arms, and to the shorts line on your pants. It reacts differently to different people, of course, but it usually is a thick covering of your torso, front and back.
 is caused by a virus. What kind of virus is unknown. A few web sites don t agree with this, but the overwhelming majority (and my personal physician) do, so that s what I m going with. The virus enters your body in some unknown manner and manifests itself in a single spot, usually the size of a nickel, somewhere on your torso, though it can start other places on your body. In my case, it started on the back of my right thigh. This spot is called the herald patch. The entire rash that will take place over your body in the next few months comes from this spot. Sometime between one and 30 days later, you ll notice a rash forming on the trunk of your body. This rash takes the initial form of a typical bumpy rash, then changes to larger, wrinkled, pinker spots. The rash usually follows the creases in your skin … under your arms, the crease in your neck, around your navel, on your ribs. The disease, and it s referred to as a disease because it s viral in nature, is truncated … meaning that it usually stays on your torso, down to the shirt sleeve line on your arms, and to the shorts line on your pants. It reacts differently to different people, of course, but it usually is a thick covering of your torso, front and back.")
48
Pityriasis Rosea (pit' - e - RYE' - uh - sis RO' - sha) is caused by a virus. What kind of virus is unknown. A few web sites don't agree with this, but the overwhelming majority (and my personal physician) do, so that's what I'm going with. The virus enters your body in some unknown manner and manifests itself in a single spot, usually the size of a nickel, somewhere on your torso, though it can start other places on your body. In my case, it started on the back of my right thigh. This spot is called the herald patch. The entire rash that will take place over your body in the next few months comes from this spot. Sometime between one and 30 days later, you'll notice a rash forming on the trunk of your body. This rash takes the initial form of a typical bumpy rash, then changes to larger, wrinkled, pinker spots. The rash usually follows the creases in your skin … under your arms, the crease in your neck, around your navel, on your ribs. The disease, and it's referred to as a disease because it's viral in nature, is truncated … meaning that it usually stays on your torso, down to the shirt sleeve line on your arms, and to the shorts line on your pants. It reacts differently to different people, of course, but it usually is a thick covering of your torso, front and back. The rash can itch, as all rashes do. There is no cure for the disease. All you can do is treat the symptoms and let it run its course. The disease is not fatal. The disease is also not communicable … no one can catch it from you. Now, here's the real kicker … the disease can last from six weeks to six months. My doctor prescribed a cream and told me there wasn't much else I could do about it. He told me to check web sites … even he knew there was some good information out there. At least my doctor had a sense of humor about it. After he let me know what it was, he told me that they call it Pityriasis Rosea because "we pity the poor son of a bitch that gets it". So, he sent me home with a cream, and a rash that was beginning to cover over half of my body. If you read anything about this disease, you'll notice that it predominately stays on your trunk, rarely going down your arms or legs, or much further than your neck. In my case, the rash spread all the way down to my wrists, almost getting on the palms of my hands, and down my legs just above my ankles. It also ran up the back of my neck into my hair and up the front of my neck to my chin. I was covered with it. I had to have a layer of cream applied over virtually my entire body twice a day.

49
There are three things that aggravate the rash, besides scratching it … sweat, hot water, and soap. Hot water, in fact, is painful. The first days of your disease, if you take hot showers or baths, you'll notice pain in areas where you seem to have no rash. This is a good precursor to the rash appearing in these spots soon. The worst part is at night. During the day, you can at least give yourself temporary relief with over the counter creams. At night, you wake up at 2:00 am, itching all over, and can't sleep. A few of the web sites said some studies were being done, and that they'd had limited success with ultraviolet light. They said if you have ultraviolet light treatments, make sure they're prescribed by a physician. So, you have a disease the stays under your clothes and is killed by ultraviolet light. Since I caught this disease in early spring, I was still wearing long sleeves and long pants … which is why, I believe, the disease spread as far as it did on my body. Again, I do not recommend or in any way represent that what I did to rid myself of this disease should be tried by anyone else. I read the information, made a decision, and tried it … and it worked. DAY 1: I woke up and noticed that I had a sore on the back of my right thigh … a small scaly patch about the size of a penny. It itched a bit, but wasn't overly troublesome. In fact, by the next day I didn't really think about it. DAY 4: My butt started to itch a bit. You could see the beginnings of a rash. DAY 5: The rash had become a bit worse, and had spread around my body to the crease between my thighs and my torso on the front of my body. I called my doctor, but he was booked. I agreed to see a nurse practitioner. My best guess was that I'd gotten this rash from wearing clothing with some kind of mites (since I'd worn a pair of shorts that I hadn't worn in months a few days before). The nurse agreed with my assessment, gave me a shot of steroids, a prescription for some cream, and a handful of antihistamines which, I found out, can relieve itching a bit. DAY 8: The rash had spread to my shoulder blades, and was beginning to make its way under my arms. It also was appearing on my chest, and had become much thicker on my butt and above my thighs. DAY 9: This rash obviously wasn't caused by mites so I saw my physician at 9:00 in the morning. I told him about the rash, what the nurse had thought it was, and took off my shirt to show him how far it had spread on my body. His first question was "did you have one spot that you noticed itched before all the others?" The herald spot. I showed him, he looked at it, and told me about Pityriasis Rosea.
. The nurse agreed with my assessment, gave me a shot of steroids, a prescription for some cream, and a handful of antihistamines which, I found out, can relieve itching a bit. DAY 8: The rash had spread to my shoulder blades, and was beginning to make its way under my arms. It also was appearing on my chest, and had become much thicker on my butt and above my thighs. DAY 9: This rash obviously wasn t caused by mites so I saw my physician at 9:00 in the morning. I told him about the rash, what the nurse had thought it was, and took off my shirt to show him how far it had spread on my body. His first question was did you have one spot that you noticed itched before all the others The herald spot. I showed him, he looked at it, and told me about Pityriasis Rosea..")
50
DAY 11: I'd spent the last two days getting covered from head to toe with a particular cream that was a bit stronger than the normal prescription. The rash continued to cover my body and was now making its way up the back of my neck, through my arm pits, and down my arms. Also, I started to get a low grade fever that would last for the next five days. DAY 13: I finally discovered the correlation between hot water and the disease. I started taking the coldest showers possible, using soap only on my face and my hair. DAY 16: My back was completely covered. My chest was showing signs of complete coverage within a few days, my stomach was starting to get the small bumps, and the rash had made its way to the bend in both elbows. The worst itching came from my navel; the rash had it covered. For the past week, I hadn't slept more than three hours at a time. I woke up, itching badly. I would apply some over the counter medicine to various spots that itched, but I'd be back up in three hours or less doing the same thing again. I was still taking cold showers with no soap, but this time I broke down and used soap on my entire body. The rash was redder than ever before, and itched worse than it had previously. DAY : The rash continued to grow. I was covered from head to toe twice a day with prescription itch cream. During the day I would cover particularly itchy spots with over the counter medicine. I was still waking up two or three times a night, applying over the counter medicine to spots that itched so badly they woke me up. DAY 19: The rash still had my entire back covered, by now in large, pink wrinkled masses. The rash was completely under both arms, all the way down both arms to my wrists; in fact, my wrists were the worst spot on both arms. The rash had also made its way down my legs, well past my knees, and looked a lot like my wrists. A huge rash was growing up the front of my neck, and had made its all the way to my chin. It had grown up the back of my neck, well into my hair. Luckily, the rash didn't find its way to my "sensitive areas", but I was afraid that it would soon. It was itching tremendously, and showed no signs of slowing down. By this time I'd gone 10 days without much sleep and nothing but cold showers. I felt like the elephant man. I was embarrassed to go out in public because the rash was becoming quite visible. This was when I made up my mind to try something. I went to a tanning salon and bought a month's pass. I spent 15 minutes on a tanning bed that evening (completely naked, save for my … well, my manhood).
..")
51
DAY 20: The rash looked no better, but no worse
DAY 20: The rash looked no better, but no worse. It was a warm sunny day, so I mowed the grass with no shirt on. The sweat, and the grass trimmings and pollen that stuck to the sweat, made me itch worse than I had so far. A cold shower helped that. DAY 21: I spent 20 minutes on a tanning bed (as naked as the first day). The rash was beginning to show signs of stopping its forward advance. One spot, the huge rash that was growing up my neck to my chin, had in fact begun to dwindle away. DAY 23: I spent another 20 minutes on a tanning bed, this time wearing just my briefs. The heaviest part of the rash on my back was diminishing. The rash on my neck was just a small mark. The rash itched less than it had in two weeks. The rash on my butt, the original rash, was now nothing more than small dark bumps, and didn't itch much at all. Same as the rash that was on the front crease of my thighs. For the first night, I went to bed without using any cream. I still got up once during the night to apply some over the counter medicine, but after falling back to sleep, I slept for six hours … the longest stretch of sleep I'd had in two weeks. DAY 24: I didn't use cream again this morning. The rash under my arms now looked like the rash on my butt the previous day; small, dark spots that don't particularly itch. The rash on my lower thighs, below my knees, was thinning out. The largest spots, on my back over my shoulder blades, were now just blotchy red spots, and itched less than usual. The rash that was making its way up the front of my neck just five days before was almost completely gone. The rash was almost gone from my hair, but was still hanging on; I reasoned that was because the tanning bed couldn't get through my hair completely. I took a warm shower, and used soap on my entire body, for the first time in 12 days. DAY 25: Three weeks ago today I noticed the first rash on my butt. Since all of the information I'd gotten said the rash would last from six weeks to six months, I should be, at best, halfway through the disease; meaning that the disease should, as of today, be at just about it's worst point. It was obvious that the rash, and the disease, was subsiding much faster than it should have been. I took another warm shower with soap, and didn't have to apply any cream to what was left of the rash. It itched a bit, but nowhere near as badly as it did just a week before. Eventually you get used to minor itching and pay it no mind. I spent another 20 minutes on the tanning bed.
. The rash was beginning to show signs of stopping its forward advance. One spot, the huge rash that was growing up my neck to my chin, had in fact begun to dwindle away. DAY 23: I spent another 20 minutes on a tanning bed, this time wearing just my briefs. The heaviest part of the rash on my back was diminishing. The rash on my neck was just a small mark. The rash itched less than it had in two weeks. The rash on my butt, the original rash, was now nothing more than small dark bumps, and didn t itch much at all. Same as the rash that was on the front crease of my thighs. For the first night, I went to bed without using any cream. I still got up once during the night to apply some over the counter medicine, but after falling back to sleep, I slept for six hours … the longest stretch of sleep I d had in two weeks. DAY 24: I didn t use cream again this morning. The rash under my arms now looked like the rash on my butt the previous day; small, dark spots that don t particularly itch. The rash on my lower thighs, below my knees, was thinning out. The largest spots, on my back over my shoulder blades, were now just blotchy red spots, and itched less than usual. The rash that was making its way up the front of my neck just five days before was almost completely gone. The rash was almost gone from my hair, but was still hanging on; I reasoned that was because the tanning bed couldn t get through my hair completely. I took a warm shower, and used soap on my entire body, for the first time in 12 days. DAY 25: Three weeks ago today I noticed the first rash on my butt. Since all of the information I d gotten said the rash would last from six weeks to six months, I should be, at best, halfway through the disease; meaning that the disease should, as of today, be at just about it s worst point. It was obvious that the rash, and the disease, was subsiding much faster than it should have been. I took another warm shower with soap, and didn t have to apply any cream to what was left of the rash. It itched a bit, but nowhere near as badly as it did just a week before. Eventually you get used to minor itching and pay it no mind. I spent another 20 minutes on the tanning bed.")
52
DAY 26: The rash on my neck is completely gone
DAY 26: The rash on my neck is completely gone. The rash in my hair is virtually gone, save for a few small spots. The rash on my butt and the front of my thighs is nothing more than small, dark spots that don't itch. The rash down my thighs is almost gone, save for a few dark red spots, and they don't itch. The rash on my shoulder blades, the worst areas affected, continued to thin out, becoming darker and more pronounced. Another 20 minutes on the tanning bad, and every spot on my body continued to heal; the small amount of rash in my hair was still holding on, but sure wasn't growing. DAY 27: I was winning the battle. I hadn't applied prescription cream in four days, except on the occasional spots that would itch, and those were rare DAY 30: I went an extra day between tanning appointments. I was by now quite dark, and the rash was on the run. Another 20 minutes on the tanning bed. The rash in my hair was almost gone. DAY 32: Four weeks ago today the first rash started. Now … it was totally gone. In four weeks. Six tanning bed sessions in two weeks had killed it. Now, I'm sure there are some in the medical profession that would disagree with me, saying that perhaps I had had a mild case of the disease. To that I say … horse hockey. I was eaten up with it, it was growing by leaps and bounds and, from the second trip to the tanning salon, I noticed it diminishing. I killed it. With a half dozen sun tans. Again, I make no claims or representations that what I did in any way affected this disease. But, in my heart, I know it did. I rid myself of a disease that can last up to six months in four weeks … and got one hell of a tan in the process. Jim Spence

53
DERMATITIS SEBOROIK DEFINISI ETIOLOGI
penyakit kulit, radang superfisialis, kronis predileksi area seboroik remisi dan eksaserbasi ETIOLOGI Penyebab pasti belum diketahui Dugaan : - Pityrosporum ovale >> - stres - kasus parah HIV (AIDS), penyakit neurologis Status seboroika yang diturunkan
, penyakit neurologis. Status seboroika yang diturunkan.")
54
EPIDEMIOLOGI PREDILEKSI Usia bayi dan orang dewasa pria >>
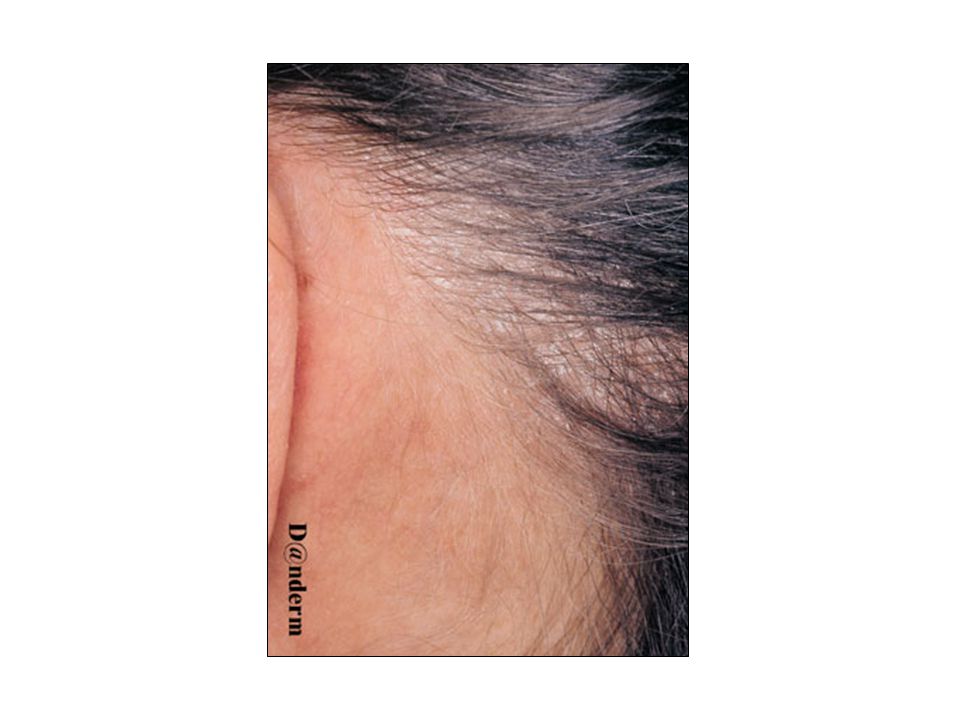
DERMATITIS SEBOROIK EPIDEMIOLOGI Usia bayi dan orang dewasa pria >> PREDILEKSI area seboroik - kelenjar sebasea >> : kepala, wajah, badan atas, pelipatan

55
Akantosis, spongiosis ringan, Infiltrat sel-sel radang, perivaskular
DERMATITIS SEBOROIK HISTOPATOLOGI Akantosis, spongiosis ringan, Infiltrat sel-sel radang, perivaskular DIAGNOSIS Klinis khas DIAGNOSIS BANDING Psoriasis vulgaris Pityriasis rosea Tinea corporis

56
PENYULIT Rambut rontok Infeksi sekunder Eritroderma PENATALAKSANAAN
DERMATITIS SEBOROIK PENYULIT Rambut rontok Infeksi sekunder Eritroderma PENATALAKSANAAN Diit rendah lemak Faktor pencetus dihindari Topikal Kepala : shampo selenium sulfide 1,8%, Zn pirithion, ketokonazole scalp solution 1%/2%, losio steroid Lokasi lain : krim kortikosteroid, Imidasol

57
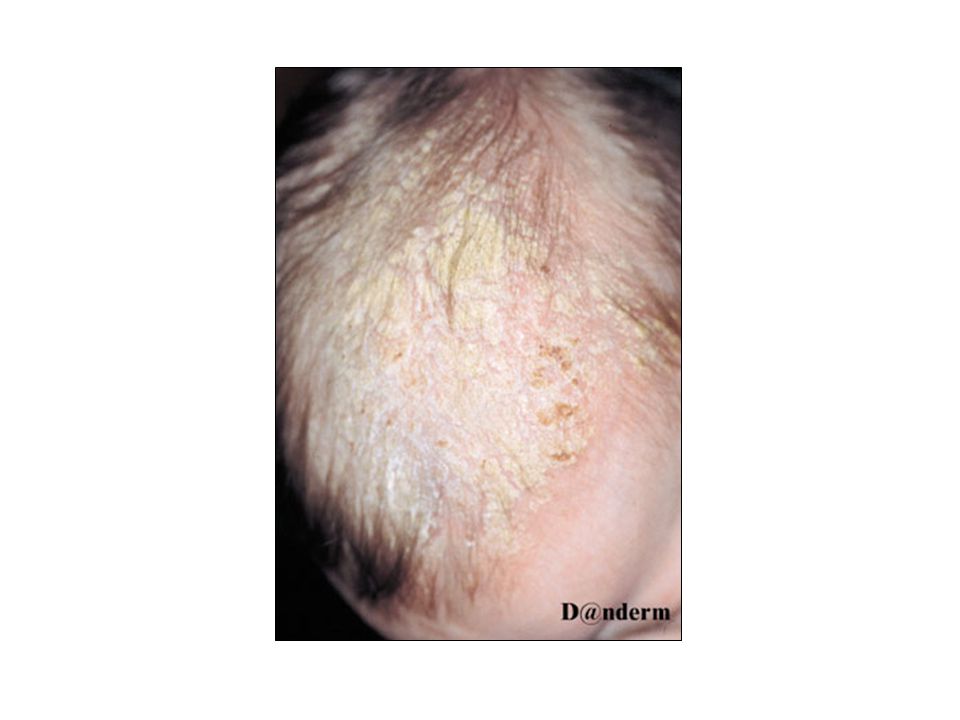
Cradle Cap pada scalp bayi

63
LICHEN PLANUS (LP) DEFINISI :
- inflamasi kulit, folikel rambut, membrana mukosa, gatal ETIOLOGI DAN PATOFISIOLOGI penyebab belum diketahui dengan pasti diduga : - kelainan imunologi - ~ infeksi bakteri, virus, jamur - paparan obat, bahan kimia tertentu

64
penyembuhan hiperpigmentasi
LICHEN PLANUS (LP) GEJALA KLINIS Gatal Kulit : papulae ( 1-4 mm) permukaan rata, kering, berkilat, poligonal, keunguan, sedikit skuama Wicham's Striae (+) penyembuhan hiperpigmentasi ekstremitas bawah >> Koebner phen (+), bilateral simetris Kuku : pterygeum, onikolisis proksimal & distal, lekukan longitudinal
 GEJALA KLINIS. Gatal. Kulit : papulae ( 1-4 mm) permukaan rata, kering, berkilat, poligonal, keunguan, sedikit skuama Wicham s Striae (+) penyembuhan hiperpigmentasi. ekstremitas bawah >> Koebner phen (+), bilateral simetris. Kuku : pterygeum, onikolisis proksimal & distal, lekukan longitudinal.")
65
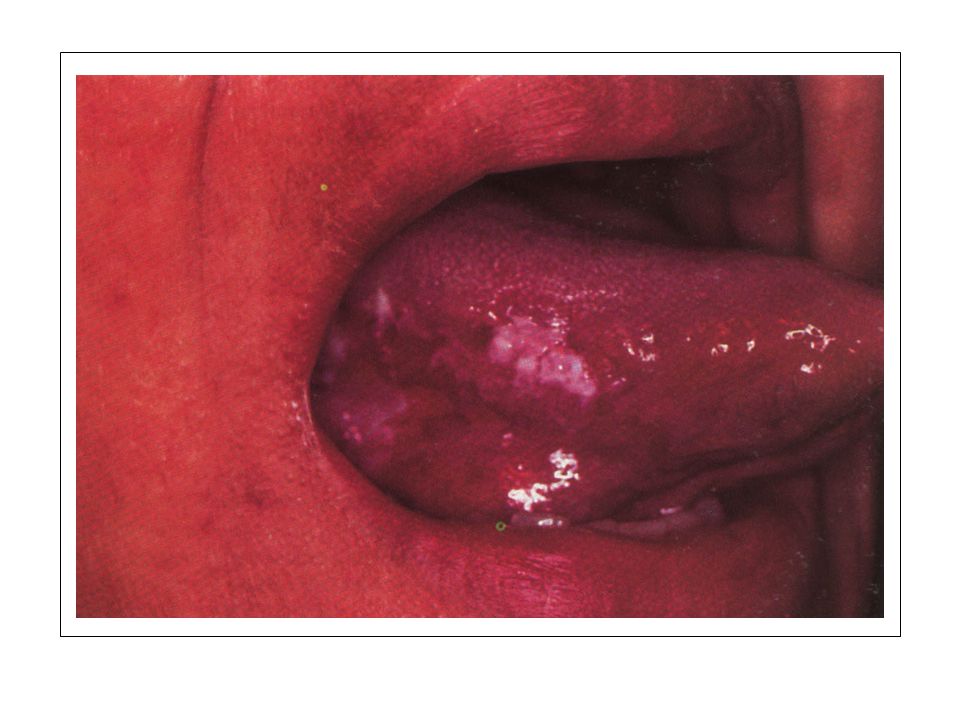
Mukosa : oral >> bentuk : - Ulseratif >>
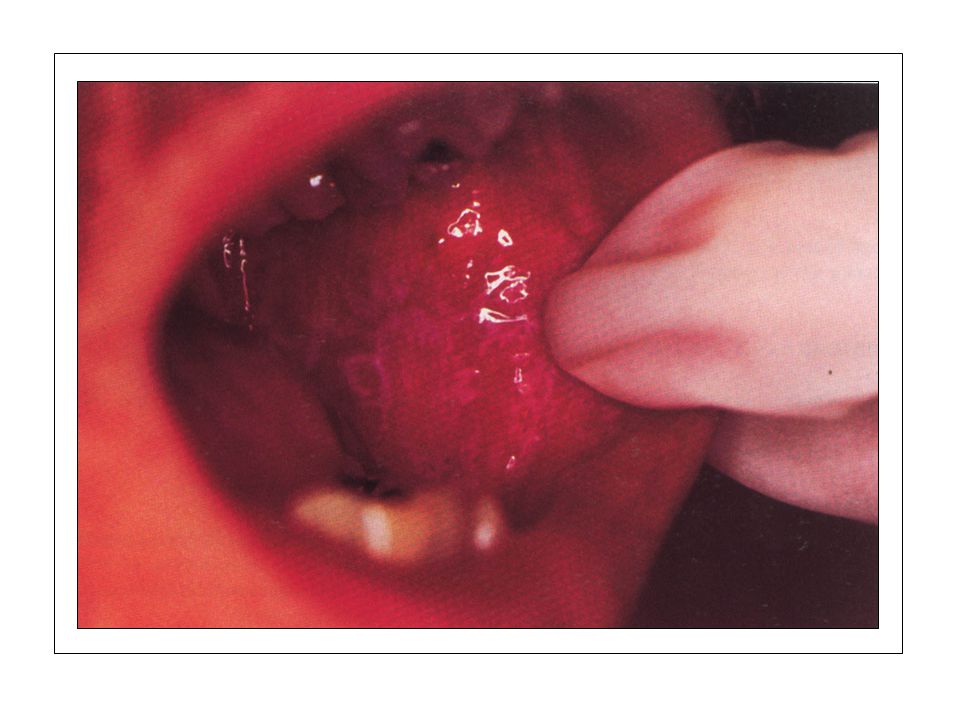
LICHEN PLANUS (LP) GEJALA KLINIS Mukosa : oral >> bentuk : - Ulseratif >> - Reticulate : pipi bagian dalam >> - Atropik Genitalia : glans penis, labia, anus papulae poligonal - Vulvovaginal erosif / ulseratif - Varian : Linear, Anular, Folikular, Hipertropik, Ulseratif, Bollous
 GEJALA KLINIS. Mukosa : oral >> bentuk : - Ulseratif >> - Reticulate : pipi bagian dalam >> - Atropik. Genitalia : glans penis, labia, anus papulae poligonal. - Vulvovaginal erosif / ulseratif. - Varian : Linear, Anular, Folikular, Hipertropik, Ulseratif, Bollous.")
66
LICHEN PLANUS (LP) DIAGNOSIS klinis DIAGNOSIS BANDING - Psoriasis vulgaris - Candidiasis - Lues II - Pityriasis Rosea
 DIAGNOSIS klinis DIAGNOSIS BANDING - Psoriasis vulgaris - Candidiasis - Lues II - Pityriasis Rosea")
67
topikal steroid superpoten / injeksi intralesi Lesi tersebar :
LICHEN PLANUS (LP) PENATALAKSANAAN Lesi terbatas : topikal steroid superpoten / injeksi intralesi Lesi tersebar : sistemik steroid, PUVA, retinoid Lesi oral : steroid in orabase, injeksi intralesi
 PENATALAKSANAAN. Lesi terbatas : topikal steroid superpoten / injeksi intralesi. Lesi tersebar : sistemik steroid, PUVA, retinoid. Lesi oral : steroid in orabase, injeksi intralesi.")
68
awal dermatitis pada taut dermoepidermal
LICHEN PLANUS (LP) HISTOPATOLOGI awal dermatitis pada taut dermoepidermal selanjutnya : hiperplasia epidermis, pola saw tooth orthokeratosis, hipergranulosis lapisan basal : keratinosit nekrotik(+) dermis : civatte bodies (+)
 HISTOPATOLOGI. awal dermatitis pada taut dermoepidermal. selanjutnya : hiperplasia epidermis, pola saw tooth. orthokeratosis, hipergranulosis. lapisan basal : keratinosit nekrotik(+) dermis : civatte bodies (+)")
74
Ada dua jenis manusia di dunia ini, seorang realis dan pemimpi.
Mereka yang realis tahu kemana akan pergi. Mereka yang pemimpi telah tiba di sana… Robert Orben

75
PITYRIASIS RUBRA PILARIS (PRP)
DEFINISI Kelainan menahun dengan : - Plak eritematus - Berskuama - Papul keratotik folikuler ETIOLOGI - HEREDITER - Autosomal dominan - Permulaan pada masa anak - DIDAPAT - Semua umur - Riwayat keluarga (-) - Diduga defisiensi vitamin A
 - Diduga defisiensi vitamin A.")
76
PITYRIASIS RUBRA PILARIS (PRP)
KLASIFIKASI Herediter - Meluas bertahap dan perlahan - Menetap Didapat - Meluas dengan cepat - Remisi

77
PITYRIASIS RUBRA PILARIS (PRP)
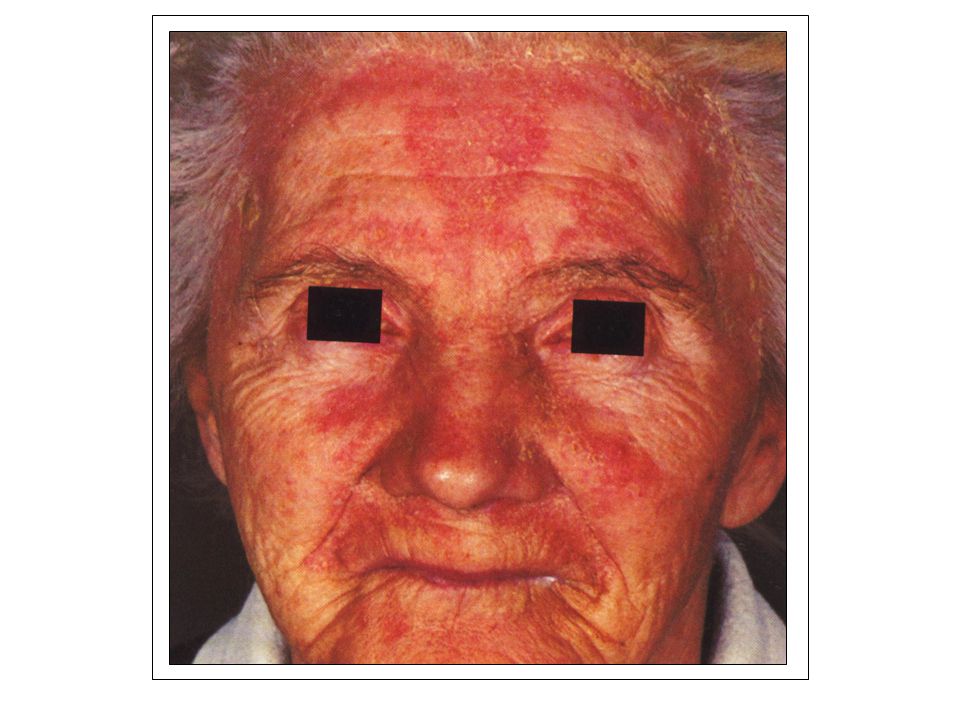
GEJALA KLINIS Eritema dan skuama pada permulaan di muka dan kulit kepala yang bisa meluas ke seluruh permukaan kulit, dilanjutkan eritema dan penebalan di telapak tangan dan kaki. Kelainan kulit batas tegas dengan pulau-pulau kulit normal. Kuku menunjukkan penebalan. Kelainan sistemik (-).
.")
78
PITYRIASIS RUBRA PILARIS (PRP)
HISTOPATOLOGIS Hiperkeratosis Parakeratosis Akantosis Sebukan sel radang menahun pada dermis atas.

79
PITYRIASIS RUBRA PILARIS (PRP)
TERAPI Vit A unit per hari. Asam retinoat 0,05% Kortkosteroid topikal + Asidum salisilikum 3 – 20%

80
PITYRIASIS RUBRA PILARIS (PRP)
PROGNOSIS Herediter : buruk Didapat : baik

85
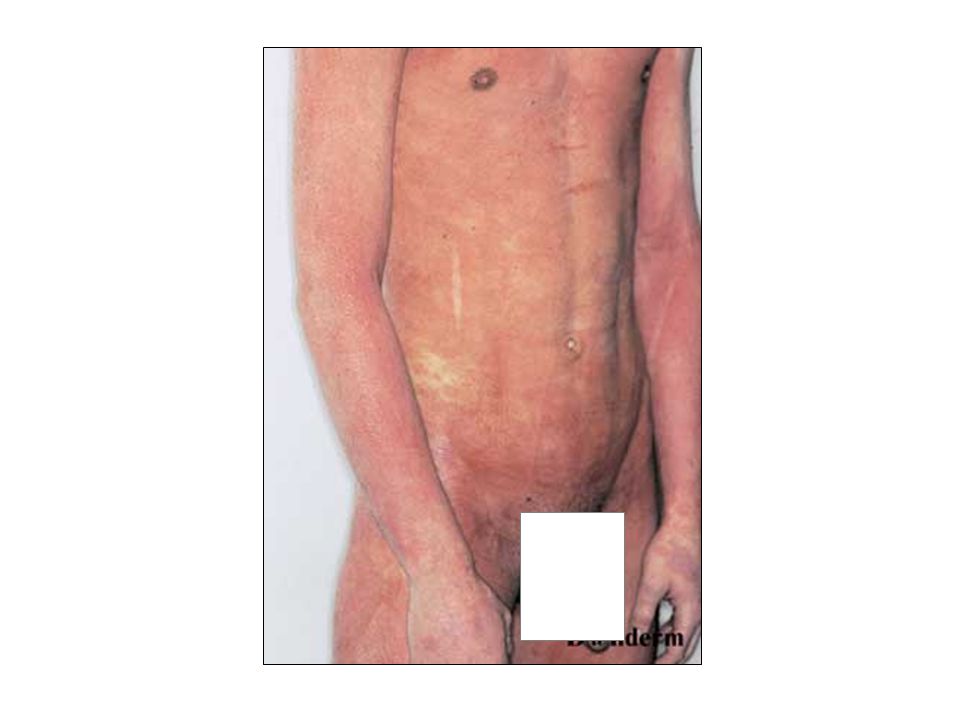
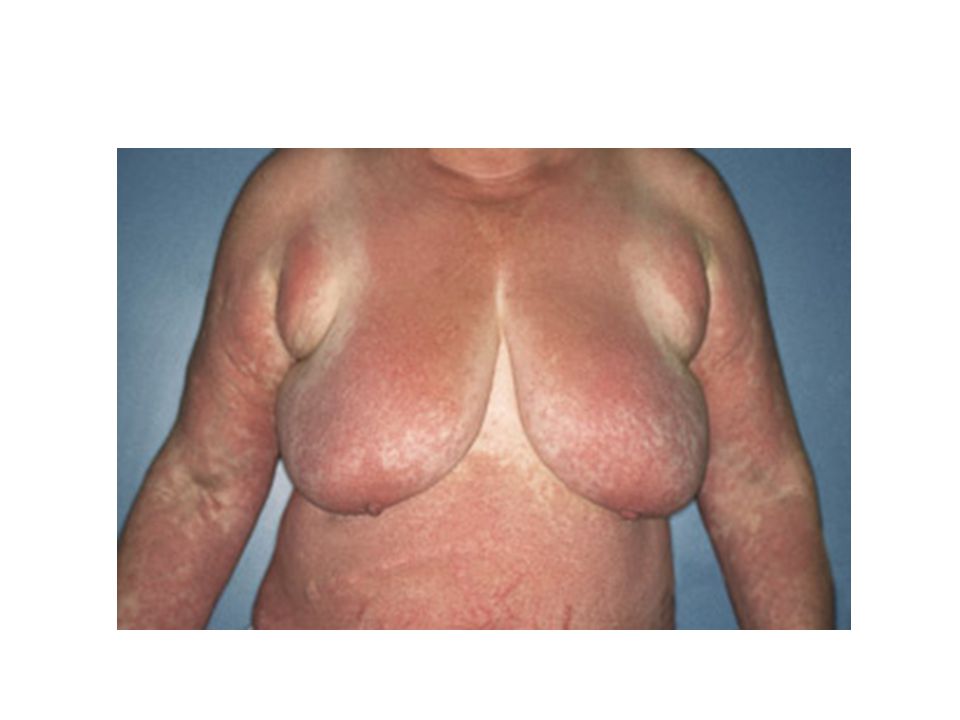
ERITRODERMA DEFINISI SINONIM
Kelainan kulit ditandai adanya eritema di hampir seluruh tubuh, biasanya disertai skuama. SINONIM Dermatitis Eksfoliativa

87
Tergantung faktor penyebab.
ERITRODERMA PATOFISIOLOGI Tergantung faktor penyebab. Pada Eritroderma terjadi peningkatan epidermal turn over, sehingga terbentuk skuama berlebihan. Skuama terutama mengandung protein, asam nukleat dan asam amino bebas.

88
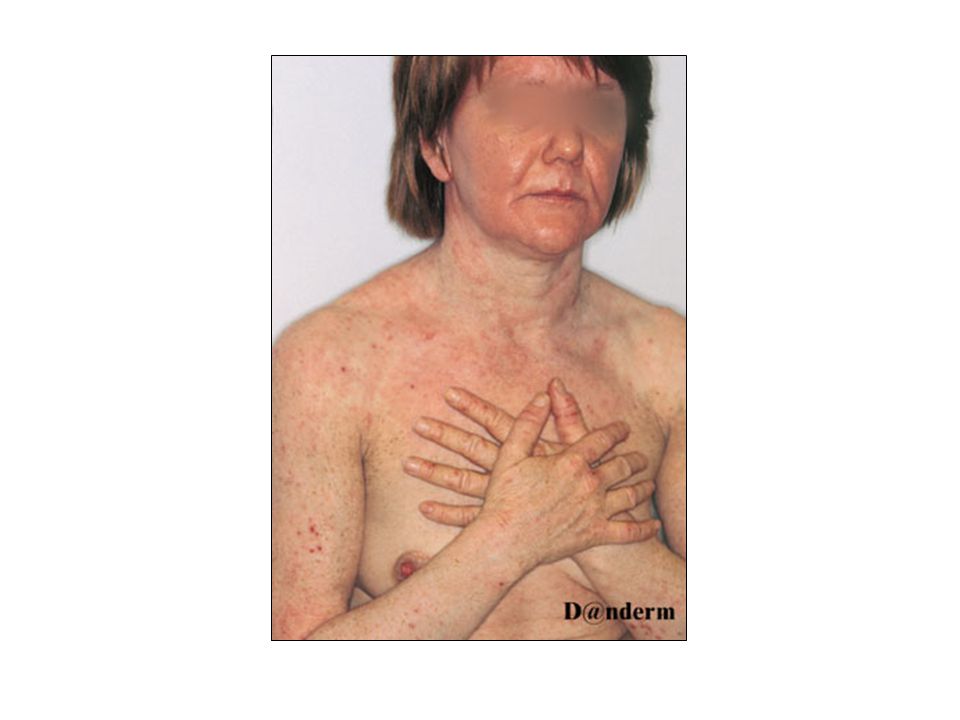
GEJALA KLINIS ERITRODERMA Timbul dalam waktu singkat Cepat meluas
Demam, menggigil,malaise Seluruh kulit tampak eritematus, mengkilap, mengelupas, teraba panas, gatal, kasar dan menebal.

90
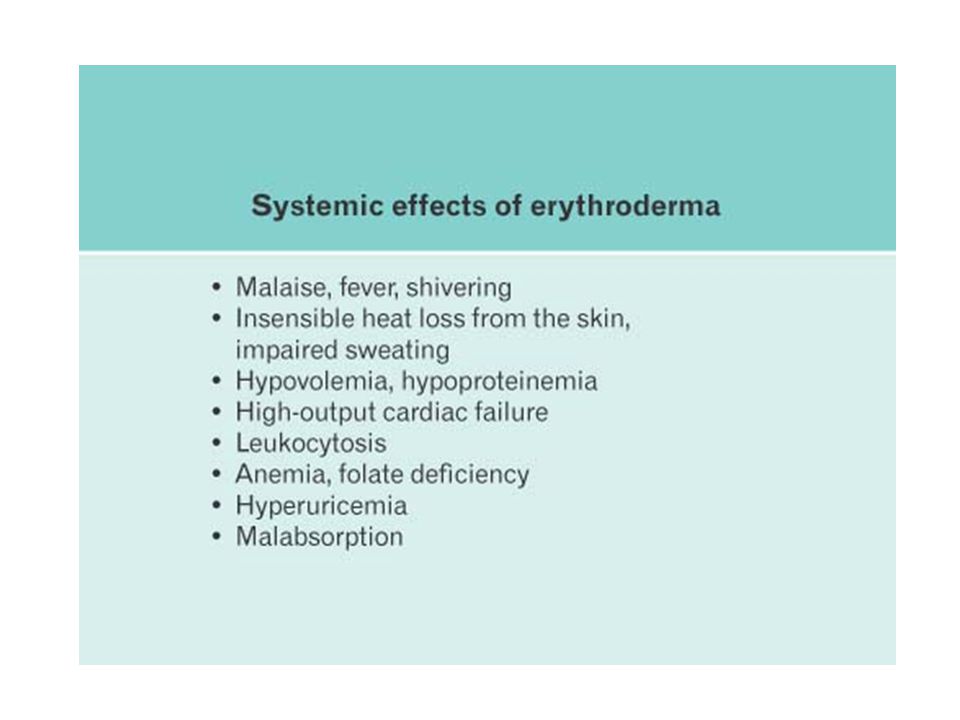
PATOFISIOLOGI ERITRODERMA Eritema : pelebaran pembuluh darah →
aliran darah ke kulit meningkat → kehilangan panas bertambah : Penderita kedinginan / menggigil Hipotermi (akibat peningkatan perfusi kulit) Dehidrasi (akibat penguapan cairan yang meningkat) Pengaturan suhu terganggu. Kehilangan skuama dapat menyebabkan kehilangan protein (hipoproteinemia) dan oedema.
 Dehidrasi (akibat penguapan cairan yang meningkat) Pengaturan suhu terganggu. Kehilangan skuama dapat menyebabkan kehilangan. protein (hipoproteinemia) dan oedema.")
91
GEJALA KLINIS ERITRODERMA Alergi obat secara sistemik
- Anamnesis : riwayat minum obat/jamu. - Alergi timbul secara akut (kurang lebih 10 hari). - Berupa eritema universal tanpa skuama, setelah sembuh baru timbul eritema. Perluasan penyakit kulit Psoriasis : - Karena penyakitnya sendiri atau pengobtan yang terlalu kuat. - Eritema yang tidak merata. (Eritema meninggi pada tempat predileksi psoriasis)
. - Berupa eritema universal tanpa skuama, setelah sembuh baru timbul eritema. Perluasan penyakit kulit. Psoriasis : - Karena penyakitnya sendiri atau pengobtan yang terlalu kuat. - Eritema yang tidak merata. (Eritema meninggi pada tempat predileksi psoriasis)")
92
ERITRODERMA Penyakit sistemik termasuk keganasan
Dermatitis Seboroika pada bayi (Leiner’s disease) - Dermatitis seboroika yang meluas - Etiologi belum diketahui dengan jelas - Usia : >>> 4 – 20 minggu. - KU penderita baik. - Eritema universal disertai skuama kasar. Penyakit sistemik termasuk keganasan - Digolongkan dalam CTCL (Cutaneous T-Cell Lymphoma) - >>> pada manula. - Eritema universal meah membara + skuama dan sangat gatal. - Pada 1/3 penderita : splenomegali, limfadenopati superfisial, alopesia, hiperpigmentasi, hiperkeratotik palmoplantar, kuku distrofia. - Laboratorium : Limfoma atipik disebut sel sezary
 - Dermatitis seboroika yang meluas. - Etiologi belum diketahui dengan jelas. - Usia : >>> 4 – 20 minggu. - KU penderita baik. - Eritema universal disertai skuama kasar. Penyakit sistemik termasuk keganasan. - Digolongkan dalam CTCL (Cutaneous T-Cell Lymphoma) - >>> pada manula. - Eritema universal meah membara + skuama dan sangat gatal. - Pada 1/3 penderita : splenomegali, limfadenopati. superfisial, alopesia, hiperpigmentasi, hiperkeratotik. palmoplantar, kuku distrofia. - Laboratorium : Limfoma atipik disebut sel sezary.")
93
ERITRODERMA DIAGNOSIS Klinis ditemukan keradangan kulit yang eritematus disertai deskuamasi hingga ≥ 90% luas permukaan tubuh. DIAGNOSIS BANDING Dermatitis, Psoriasis vulgaris, Drug Eruption,Limfoma/Leukemia,Pemfigus, Pityriasis Rubra Pilaris,Likhen Planus, Dermatofitosis, Skabies

94
Kegagalan sirkulasi perifer Tromboflebitis
ERITRODERMA PENYULIT Hipotermi Dekompensasi kordis Kegagalan sirkulasi perifer Tromboflebitis Infeksi sekunder pada kulit dan paru

95
PENATALAKSANAAN ERITRODERMA Perbaiki cairan tubuh
Eliminasi faktor-faktor pencetus Kortikosteroid sistemik “tappering off” Antibiotika untuk mencegaf infeksi sekunder Antihistamin/antipruritus Topikal : emolient (oleum coccos, hidrokortison 1%) Diit tinggi protein
 Diit tinggi protein.")
104
Seni yang dilakukan oleh DERMATOLOG adalah “memberi suatu penyakit dengan nama latin yang panjang ….. dan kemudian memberinya steroid topikal.”

Presentasi serupa


































 the RIGHT one for me?” “Should I BUY this? Or SELL that?” “Should I INVEST in.>")

 that is put before original verb, if the words are preceded by: The other verbs To be Examples: Saya.>")






 A ministry of Campus Crusade for Christ Australia.>")


