Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
Pharmacovigilance MK Farmasi Komunitas
Bagian Farmasi Klinik dan Komunitas Fak Farmasi Univ Jember

2
Pharmacovigilance is not only a science of adverse drug effects!
Defined by WHO, pharmacovigilance is The science and activities relating to detection, assessment, understanding and prevention of adverse effects or any other drug-related problems. Spontaneous ADR reporting system

3
ADR Definition (WHO 1972) A response to a drug that is noxious and unintended and occurs at doses normally used in man for the prophylaxis, diagnosis or therapy of disease, or for modification of physiological function. Problems: Including minor adverse reactions, e.g.? Excluding error as a source of adverse effects

4
ADR Definition (Laurence & Carpenter, 1998, A dictionary of pharmacology and allied topics)
Exclude minor adverse reactions A harmful or significantly unpleasant effect caused by a drug at doses intended for therapeutic effect (or prophylaxis or diagnosis) which warrants reduction of dose or withdrawal of the drug and/or foretells hazard from future administration. Problems: Excluding error as a source of adverse effects
 which warrants reduction of dose or withdrawal of the drug and/or foretells hazard from future administration. Problems: Excluding error as a source of adverse effects.")
5
ADR Definition (Edwards & Aronson, 2000)
Proposed definition of adverse drug reaction: An appreciably harmful or unpleasant reaction, resulting from an intervention related to the use of a medicinal product, which predicts hazard from future administration and warrants prevention or specific treatment, or alteration of the dosage regimen, or withdrawal of the product.

6
WHO’s Adverse Drug Reaction Terminology (WHO-ART), 1992
An adverse drug reaction (ADR) is ‘a response to a medicine which is noxious and unintended, and which occurs at doses normally used in man’. It concerns: the response of a patient, in which individual factors may play an important role, the phenomenon is noxious (an unexpected therapeutic response, for example, may be a side effect but not an adverse reaction). Currently accepted international terminology of ADR Main goal: improving pharmacovigilance communication, integrated with other WHO’s project: International Classification of Diseases (ICD, 10th version) And, there still have a problems: combining the terminology with bibliographic databases (Uppsala Monitoring Centre) An adverse drug reaction (ADR) is ‘a response to a medicine which is noxious and unintended, and which occurs at doses normally used in man’. In this description it is of importance that it concerns the response of a patient, in which individual factors may play an important role, and that the phenomenon is noxious (an unexpected therapeutic response, for example, may be a side effect but not an adverse reaction). 2. An unexpected adverse reaction is ‘an adverse reaction, the nature or severity of which is not consistent with domestic labelling or market authorisation, or expected from characteristics of the drug’. 3. A drug or medicine is ‘a pharmaceutical product, used in or on the human body for the prevention, diagnosis or treatment of disease, or for the modifi cation of physiological function’. 4. A side effect is ‘any unintended effect of a pharmaceutical product occurring at doses normally used by a patient which is related to the pharmacological properties of the drug’. Essential elements in this defi nition are the pharmacological nature of the effect, that the phenomenon is unintended, and that there is no deliberate overdose. 5. An adverse event or experience is defi ned as ‘any untoward medical occurrence that may present during treatment with a medicine but which does not necessarily have a causal relationship with this treatment’. The basic point here is the coincidence in time without any suspicion of a causal relationship.
 is ‘a response to a medicine which is noxious and unintended, and which occurs at doses normally used in man’. It concerns: the response of a patient, in which individual factors may play an important role, the phenomenon is noxious (an unexpected therapeutic response, for example, may be a side effect but not an adverse reaction). Currently accepted international terminology of ADR. Main goal: improving pharmacovigilance communication, integrated with other WHO’s project: International Classification of Diseases (ICD, 10th version) And, there still have a problems: combining the terminology with bibliographic databases. (Uppsala Monitoring Centre) An adverse drug reaction (ADR) is ‘a response to a medicine which is. noxious and unintended, and which occurs at doses normally used in. man’. In this description it is of importance that it concerns the response. of a patient, in which individual factors may play an important role, and that the phenomenon is noxious (an unexpected therapeutic. response, for example, may be a side effect but not an adverse reaction). 2. An unexpected adverse reaction is ‘an adverse reaction, the nature or. severity of which is not consistent with domestic labelling or market. authorisation, or expected from characteristics of the drug’. 3. A drug or medicine is ‘a pharmaceutical product, used in or on the human. body for the prevention, diagnosis or treatment of disease, or for. the modifi cation of physiological function’. 4. A side effect is ‘any unintended effect of a pharmaceutical product. occurring at doses normally used by a patient which is related to the. pharmacological properties of the drug’. Essential elements in this defi nition are the pharmacological nature. of the effect, that the phenomenon is unintended, and that there is no. deliberate overdose. 5. An adverse event or experience is defi ned as ‘any untoward medical. occurrence that may present during treatment with a medicine but. which does not necessarily have a causal relationship with this treatment’. The basic point here is the coincidence in time without any suspicion. of a causal relationship.")
7
Side Effect and Toxic Effect?
WHO, 1992: A side effect is ‘any unintended effect of a pharmaceutical product occurring at doses normally used by a patient which is related to the pharmacological properties of the drug’. Essential elements the pharmacological nature of the effect, that the phenomenon is unintended there is no deliberate overdose, at normal dose

8
So, the differences are ... Side Effect Toxic Effect
Occured in normal dose Not always dose-dependent Not via therapeutic effect Maybe beneficial E.g. Anaphylaxis of penicillins Anticholinergic activity of tricyclic antidepressants Beta-blocker activity for hypertension and angina Occured in overdose Always dose-dependent Via therapeutic effect Always harmful E.g. a headache due to a calcium antagonist is a toxic effect (vasodilatation)
")
9
ADR, Side Effect, and Toxic Efect
Toxic Effect Adverse Effect from point of view of the drug Adverse Effect Adverse Drug Reaction from point of view of patient

10
But, we have to distinguish ADVERSE EFFECT and ADVERSE EVENT
Adverse Effect: always drug-related Adverse Event: not always drug-related

11
ADR Classification

12
A (Augmented) BCDEF - Mnemonic
Dose dependent Predictable from the known pharmacology of the drug Common and low mortality Case: Digoxin toxicity Serotonine syndrome with SSRIs Anticholinergic effects of tricyclic antidepressants

13
AB (Bizarre) CDEF Non dose dependent
Unpredictable from the known pharmacology of the drug Uncommon and high mortality Case: Penicillin hypersensitivity Acute porphyria Malignant hyperthermia

14
ABC (Chronic) DEF Dose-related and time-related Uncommon
Related to the cummulative dose Case: Hypothalamic-pituitary-adrenal axis supression by corticosteroids

15
ABCD (Delayed) EF Time-related and usually dose-related Uncommon
Occurs or become apparent after some time the use of the drug Case: Vaginal adenocarcinoma with diethylstilbestrol Carcinogenesis Tardive dyskinesia

16
ABCDE (End of Use) F Withdrawal Uncommon
Occurs soon after withdrawal of the drug Case: Opiate withdrawal syndrome Myocardial ischaemia (beta-blocker withdrawal)
")
17
ABCDEF (Failure) Unexpected failure of therapy Common Dose-related
Often caused by drug interactions Case: Inadequate dosage of an oral contraceptive when used with specific enzyme inducers

18
Case Erythromycin and nausea-vomitting

19
The DoTS Classification
ADR Dose Susceptibility Time

20
Do (Dose relatedness) TS
Supratherapeutic doses toxic dose Collateral effects, at standard/ normal therapeutic dose commonly named side effect Hypersusceptibility reactions

21
DoT (Time relatedness) S
Time independent reactions Time dependent reactions Rapid reactions, e.g. the red man syndrome with vancomycin First dose reactions, e.g. Hypotension after the first dose of an ACE-inhibitor Type I hypersensitivity reactions Early reactions, e.g. Nitrate induced headache Intermediate reactions, e.g. Type II-IV hypersensitivity reactions Late reactions, e.g. Adverse effects of corticosteroids, tardive dyskinesia with dopamine receptor antagonists Delayed reactions, e.g. Teratogenesis due to thalidomide

22
DoTS (Susceptibility sources)
Genetic, e.g. Porphyria Malignant hyperthermia CYP isoenzyme polymorphism Age, e.g. Neonates and chloramphenicol Elderly people with hypnotics

23
DoTS (Susceptibility sources)
Sex, e.g. Alcohol intoxication Mefloquine and neuropsychiatric effect ACE-inhibitor and cough Lupus-like syndrome Physiology altered, e.g. Phenytoin in pregnancy

24
DoTS (Susceptibility sources)
Exogenous factors, e.g. Drug interactions Interactions of GJ with drugs metabolized by CYP3A4 Disease, e.g. Renal insufficiency with lithium Hepatic chirrosis with morphine

25
Process in Pharmacovigilance
Signal detection Evaluation and investigation Taking action Communication Crisis management

26
Signal Detection What is signal?
Signal is Reported information on a possible causal relationship between an adverse event and a drug, the relationship being unknown or incompletely documented previously. Usually more than a single report, depending upon: the seriousness of the event and the quality of the information

27
Signal Detection What is signal?
The data source may be associated with: Previously unrecognised hazard Known hazard that may be different from existing knowledge Quantitatively more frequent Qualitatively more serious Tiaprofenic acid and cystitis in mid-1990s

28
Signal Detection Processes for signal detection
Number of reports to generate a signal: When the suspected ADR is a disease which is rare in the general population (e.g. aplastic anaemia, toxic epidermal necrolysis) a very small number of cases associated with a single drug is unlikely to be a chance phenomenon, even if the drug has been used quite widely. Except for certain types of event that are particularly important and likely to be drug related (e.g. anaphylaxis) three cases
 a very small number of cases associated with a single drug is unlikely to be a chance phenomenon, even if the drug has been used quite widely. Except for certain types of event that are particularly important and likely to be drug related (e.g. anaphylaxis) three cases.")
29
Signal Detection Processes for signal detection
“Profiling” to create “ADR profile” and to find the “disproportionality” Profiling Creating the proportions of all ADRs for a particular drug that are of a specific type – perhaps within an organ system class of reactions (e.g. gastrointestinal or cutaneous).
.")
30
Signal Detection Processes for signal detection
Example of profiling process UK Yellow Card, mid-1990s: ± 600,000 suspected reactions in 30 years ± 800 classified as ‘uveitis’ – about 0.13% rifabutin some 41 cases of uveitis from total 55 reactions in that time (i.e. 75% of them were uveitis).
.")
31
Signal Detection Uveitis

32
Signal Detection Processes for signal detection
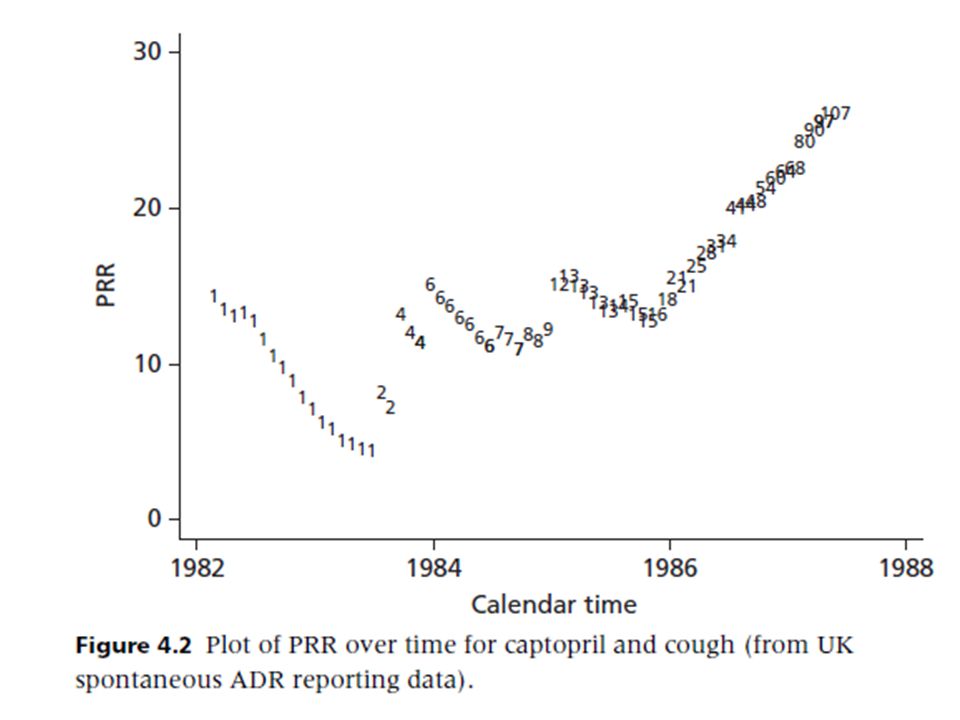
PRR: Proportional Reporting Ratio

33
Signal Detection Processes for signal detection
Example of profiling process Cut-off points for a minimum signal: PRR > 3 Chi-squared > 4 (roughly 5% of statistical significance) N = 3 or more Visualisation of data (ADR profiles)
 N = 3 or more. Visualisation of data (ADR profiles)")
34
Number of reports (N) as the symbol
 as the symbol")
36
Signal Detection Processes for signal detection
Another measure of disproportionality: Reporting Odds Ratio (ROR) Netherlands Information Component (IC, Bayesian) WHO US FDA Multi-Item Gamma Poisson Shrinker (MGPS, Bayesian)
 Netherlands. Information Component (IC, Bayesian) WHO. US FDA Multi-Item Gamma Poisson Shrinker (MGPS, Bayesian)")
37
Overview of Pharmacovigilance Programmes
Tujuh negara yang tidak memiliki program farmakovigilans: Banglades, Ekuador, Liberia, Malawi, Mauritius, Timor Leste, Uni Emirat Arab Kedudukan struktural: Tergabung dalam Drug Regulatory Agency: 70% (n=31) Tergabung dalam Ministry of Health: 20% Tergabung dengan universitas atau lembaga akademis: 10% Pusat kegiatan: 60% (n=28) tersentralisasi 40% (n=20): regional center atau sentinel sites
 Tergabung dalam Ministry of Health: 20% Tergabung dengan universitas atau lembaga akademis: 10% Pusat kegiatan: 60% (n=28) tersentralisasi. 40% (n=20): regional center atau sentinel sites.")
38
Overview of Pharmacovigilance Programmes
Sumber daya manusia pada setiap pusat: 1 petugas : 6 negara 2-4 petugas : 17 negara 5-9 petugas : 14 negara 10-19 petugas: 3 negara 20-29 petugas: 2 negara >30 petugas : 3

39
TI, Dukungan Internet dan Akses thd Referensi
Hampir semua (n=46 dari 48) mengakses komputer Komputer yg didisain spesifik unt farmakovigilans: 11 negara Komputer tdk begitu mendukung kebutuhan farmakovigilans: 11 negara 32 negara mengeklaim memiliki akses cukup thd referensi ttg keamanan obat dari perpustakaan lokal atau internet
 mengakses komputer. Komputer yg didisain spesifik unt farmakovigilans: 11 negara. Komputer tdk begitu mendukung kebutuhan farmakovigilans: 11 negara. 32 negara mengeklaim memiliki akses cukup thd referensi ttg keamanan obat dari perpustakaan lokal atau internet.")
40
Spontaneous Reporting Macam-macam Aktivitas
Hanya farmakovigilans: 6 negara (13%) + informasi obat: 63% + promosi keamanan obat: 52% + penggunaan obat rasional: 46% + informasi keracunan: 15%
 + informasi obat: 63% + promosi keamanan obat: 52% + penggunaan obat rasional: 46% + informasi keracunan: 15%")
41
Spontaneous Reporting Macam-macam Aktivitas

42
Spontaneous Reporting Who Reports
Di 33 negara (67%): menjadi persyaratan legal untuk pemegang izin edar obat 8 negara (17%): persyaratan legal untuk tenaga kesehatan All (n=48): dokter 98% (n=47): farmasis 90%: perawat 79%: produsen 58%: pasien 38%: traditional therapist
: menjadi persyaratan legal untuk pemegang izin edar obat. 8 negara (17%): persyaratan legal untuk tenaga kesehatan. All (n=48): dokter. 98% (n=47): farmasis. 90%: perawat. 79%: produsen. 58%: pasien. 38%: traditional therapist.")
43
Spontaneous Reporting What is Reported
Di 33 negara (67%): menjadi persyaratan legal untuk pemegang izin edar obat 8 negara (17%): persyaratan legal untuk tenaga kesehatan All (n=48): dokter 98% (n=47): farmasis 90%: perawat 79%: produsen 58%: pasien 38%: traditional therapist
: menjadi persyaratan legal untuk pemegang izin edar obat. 8 negara (17%): persyaratan legal untuk tenaga kesehatan. All (n=48): dokter. 98% (n=47): farmasis. 90%: perawat. 79%: produsen. 58%: pasien. 38%: traditional therapist.")
44
Farmakovigilans di Indonesia (MESO)
")
45
Kegunaan MESO BADAN PENGAWASAN OBAT PERUSAHAAN FARMASI SISI AKADEMIK
Menilai hubungan kausal obat dengan gejala yang dicurigai sebagai keluhan efek samping obat → berdampak pada peredaran dan penandaan obat PERUSAHAAN FARMASI Pengamanan investasi yang telah ditanamkan dalam pengembangan dan penelitian obat baru → berdampak pada keamanan obat SISI AKADEMIK Menguji suatu hipotesis → analisa struktur kimia obat atau golongan obat Misal: MESO Cimetidine dilakukan karena struktur kimianya mirip dengan Methiamide yang telah ditarik karena menyebabkan agranulositosis

46
Form dan Buletin MESO POM
Form MESO nasional Buletin MESO POM Terbit 1 tahun 2 kali Tersedia dalam bentuk elektronik Tips: Via Google.com buletin berita eso site:pom.go.id

47
Cara MESO LAPORAN INSIDENTAL LAPORAN SUKARELA
biasanya dikemukakan pada pertemuan-pertemuan di RS atau laporan kasus di majalah tidak dapat tersebar dengan cepat karena tidak ada organisasi nasional yang mengatur pengendalian ESO yang diduga, sangat tergantung pada motivasi masing-masing klinikus LAPORAN SUKARELA dikoordinir oleh pusat disebut “laporan spontan” diminta melaporkan ESO pada praktek sehari-hari

48
Cara MESO LAPORAN INTENSIF di RS
kelompok dokter, perawat terlatih, ahli farmasi mencari dan mengumpulkanESO populasi tertentu dan terbatas di RS data yang terkumpul dianalisa oleh tim ahli

49
Cara MESO LAPORAN LEWAT CATATAN MEDIK LAPORAN WAJIB
pengumpulan data melalui riwayat penyakit serta pengobatan yang diterima dari bermacam sumber mungkin dikerjakan di tempat di mana pelayanan medik yang lengkap, terorganisir baik dan fasilitas komputer yang canggih LAPORAN WAJIB ada peraturan yang mewajibkan setiap petugas kesehatan melaporkan ESO di tempat tugas atau praktek sehari-hari

50
References Aronson JK, Ferner RE, 2003, Joining the DoTS: new approach to classifying adverse drug reactions, BMJ, 327, p Edwards, IR, Aronson, JK, 2000, Adverse drug reactions: definitions, diagnosis, and management, The Lancet, 356, p Olsson S, Pal SN, Stergachis A, Couper M. Pharmacovigilance activities in 55 low- and middle-income countries: a questionnaire-based analysis, Drug Saf, 2010 Aug 1;33(8):689–703. Waller, P., 2010, An Introduction to Pharmacovigilance, John Wiley and Sons: West Sussex
:689–703. Waller, P., 2010, An Introduction to Pharmacovigilance, John Wiley and Sons: West Sussex.")
Presentasi serupa


 pada Radiology Information System (RIS)>")














>")

