Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
PDP Thesis Oleh : dr. Kun Marisa Farhana
Pembimbing I: Prof.Dr.dr.Samekto Wibowo, P.farK, Sp.FK(K), Sp.S(K) Pembimbing II : dr. Abdul Ghofir,Sp.S(K)
, Sp.S(K) Pembimbing II : dr. Abdul Ghofir,Sp.S(K)")
2
JUDUL Efektifitas Ekstrak Daun Pegagan (Centella Aisatica) untuk Terapi Gangguan Konitif Vaskuler
 untuk Terapi Gangguan Konitif Vaskuler")
3
Latar belakang masalah (1)
Gangguan kognitif yang berhubungan dengan stroke heterogen, sering tidak terdeteksi Penyakit cerebrovaskuler merupakan faktor risiko terjadinya gangguan kognitif 50%-75% pasien post stroke dengan gangguan kognitif berkembang menjadi demensia Haring,2002

4
Latar Belakang Masalah(2)
Penatalaksanaan penyakit serebrovaskuler harus meliputi preventif stroke dan terapi spesifik gangguan kognitif Belum cukup data mengenai pengaruh pengendalian faktor risiko terhadap perbaikan fungsi kognitif

5
Latar belakang(3) Obat-obatan neuroprotektif , antidepresant , hipnosedatif memiliki beberapa kerugaian dan mahal kecenderungan pengguanaan bahan alam Kandungan utama pegagan (Centella asiatica) berupa triterpen saponin memliki aktaifitas antioxidant, antiinflamasi dan antiapoptosis
 berupa triterpen saponin memliki aktaifitas antioxidant, antiinflamasi dan antiapoptosis.")
6
Perumusan masalah Gangguan kognitif vaskuler dapat berkembang menjadi demensia Demensia vaskuler merupakan kelainan yang dapat dicegah Penggunaan obat herbal ekstrak pegagan (Centella asiatica) untuk meningkatkan fungsi kognitif masih perlu penelitian lebih lanjut
 untuk meningkatkan fungsi kognitif masih perlu penelitian lebih lanjut.")
7
Pertanyaan penelitian
Apakah pemberian ekstrak daun pegagan efektif untuk memperbaiki gangguan kognitif vaskuler

8
Tujuan Penilitian Mengetahui perbaikan fungsi kognitif pada pasien gangguan kognitif vaskuler dengan menggunakan Montreal Cognitif Assesent- Indonesia setelah peberian ekstrak pegagan mg/hari selama 60 hari

9
Manfaat penelitian Diharapkan dapat menambah pengetahuan tenaga dan masyarakat tentang manfaaat ekstrak pegagan (Centella asiatica) terhadap perbaikan fungsi kognitif pada pasien dengan gangguan kognitif vaskuler
 terhadap perbaikan fungsi kognitif pada pasien dengan gangguan kognitif vaskuler.")
10
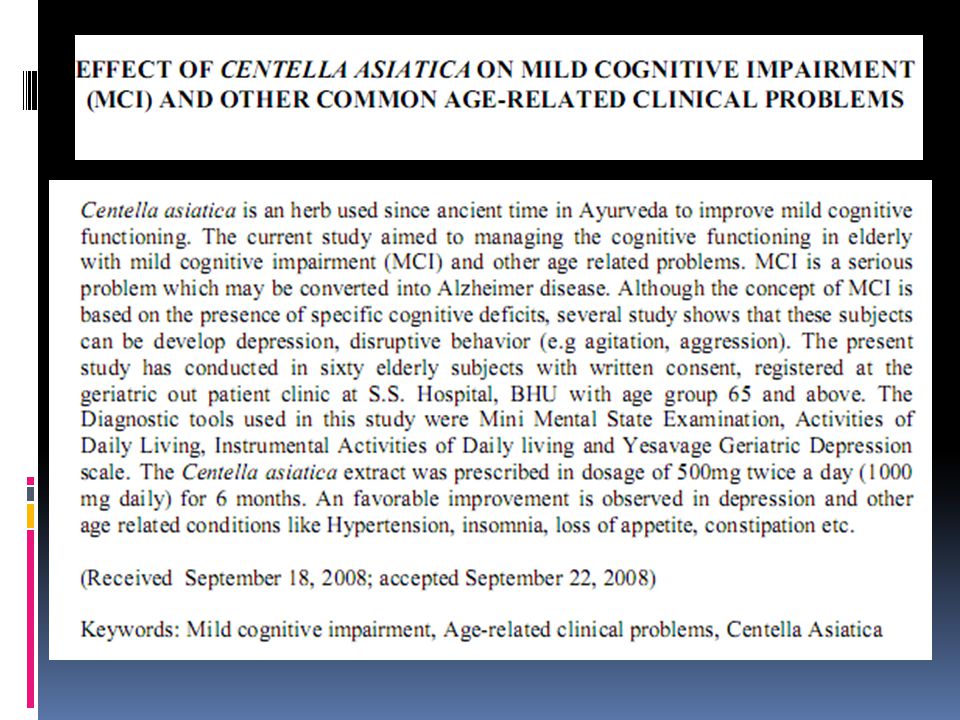
Keaslian penelitian No Peneliti Judul Metode Alat ukur Obat 1
Tiwari et al.,2008 Effect of Centella asiatica on MCI and other common age related clinical problems Eksperimental cohort 6 bulan MMSE 2 x 500 mg 2 Dev et al.,2009 Comparison on cognitive effect of CeA in healthy middle age female and male volunteer 60 hari Woodcock Johnson Cognitive Abilities test III 3g dan 4g 3 Watanathorn et al,2007 Positive modulation of cognition and mood in the healthy elderly volunteer following administration ofCeA Double blind RCT Computer batery test,lader visual analog scale 250,500, 750 mg once daily

11
Kerangka teori

12
+ Protein or lipid Small vesel disease Large vessel Disease Hipertensi
Diabetes Melitus Vasculer Endotelium Change Infark/isemia ROS+Sugar Glycolisis n TCA Cycle Neurotramsmiter ATP Inflamasi+Gliosis Centela asiatica Carbonyl Kegagalan pompa Depolarisasi Mitocondria disfunction Hipoperfusi, hipoxia + Protein or lipid Ca Influks Glicocylation or lipooxidation products Superoxide Transduksi signalabnormal ROS Nerve disfunction + Death Apoptosis Oxidative Stress Centela asiatica Centella Asiatica VCI

13
Kerangka konsep Faktor Risiko : Faktor Risisko lain: Stroke DM
Hipertensi Faktor Risisko lain: Lokasi infark Lama menderita Depresi Variabel tergantung: Gangguan Cognitif Demografi : Usia JenisKelamin Pendidikan Variabel bebas : Ekstrak Pegagan

14
Rancangan penelitian Desain penelitian menggunakan metode penelitian acak terkendali, buta ganda selama 60 hari Dua kelompok subyek dengan variabel yang mirip: Perlakuan : ekstrak pegagan 2x 500 mg & citicolin e 2x500mg Kontrol : Placebo&citicoline 2x500mg

15
Subyek penelitian Subyek penelitian adalah semua pasien pasca stroke dengan gangguan cognitif yang kontrol di poli saraf RSUP Dr. Sarjito

16
Kriteria inklusi Usia> 18 th Mild stroke (NIHSS <4)
Bukti infark pada ct scan Faktor risiko vaskuler MoCA-Ina < 26 Informed consent

17
Kriteria eksklusi ADL-IADL :dependen Short IQ-Code > 3,4
Parkinson disease Gangguan penglihatan dan pendengaran berat Penyakit psikiatri Tinggal sendiri Terapi cognitif sebelumnya

18
Hipotesis Pemberian ekstrak pegagan (centella asiatica) dapat memperbaiki fungsi kognitif pada pasien Gangguan kognitif vaskuler
 dapat memperbaiki fungsi kognitif pada pasien Gangguan kognitif vaskuler.")
19
Besar sampel n1= n2 = 2 (Zα + Zβ) x S 2 x1 – x2 Nilai x1- x2 adalah 3,30, sedangkan nilai S adalah 9,68(Tiwari et al.,2008). Pada penelitian ini, peneliti menetapkan nilai α adalah dan nilai β adalah 0.20 sehingga Zα adalah 1.96 dan Zβ adalah Jumlah sampel (n) yang dibutuhkan tiap kelompok berdasarkan rumus di atas adalah sebesar 22 orang. Drop out ditentukan sebesar 10% maka besar sampel minimal yang dibutuhkan tiap kelompok adalah sebesar 25 subyek
 yang dibutuhkan tiap kelompok berdasarkan rumus di atas adalah sebesar 22 orang. Drop out ditentukan sebesar 10% maka besar sampel minimal yang dibutuhkan tiap kelompok adalah sebesar 25 subyek.")
20
Variabel penelitian Variabel Bebas Variabel Tergantung
Jenis Terapi: Terapi perlakuan dan terapi kontrol (K/Nom) Variabel Tergantung Nilai MoCA-Ina(Nu/rasio) Efek samping terapi (K/Nom) Variabel Perancu Usia (Nu/rasio) Jenis kelamin (K/Nom) Pendidikan (K/Nom) Lokasi lesi
 Variabel Tergantung. Nilai MoCA-Ina(Nu/rasio) Efek samping terapi (K/Nom) Variabel Perancu. Usia (Nu/rasio) Jenis kelamin (K/Nom) Pendidikan (K/Nom) Lokasi lesi.")
21
Definisi Operasional Probable DVa Diagnosis klinis probable DVa meliputi semua item di bawah ini: Demensia. Bukti adanya penyakit serebrovaskular yang konsisten dengan stroke, dan kejadiannya mempunyai relevansi dengan pencitraan otak. Terdapat hubungan antara kedua gangguan di atas dengan satu atau lebih keadaan di bawah ini: Awitan demensia berada dalam kurun waktu 3 bulan pasca stroke Deteriorasi fungsi luhur yang mendadak atau berfluktuasi, defisit kognisi yang progresif dan bersifat stepwise

22
Atau tidak adanya hubungan waktu yang jelas antara demensia dan stroke
Possible DVa Demensia disertai defisit neurologis fokal, tetapi tanpa konfirmasi pencitraan otak Atau tidak adanya hubungan waktu yang jelas antara demensia dan stroke Atau awitan penyakit tidak jelas dengan perjalanan klinis yang bervariasi seperti plateau atau perbaikan defisit kognitif Definite DVa Kriteria klinik “probable DVa” Konfirmasi pemeriksaan histopatologi penyakit serebrovaskular Adanya neurofibrillary tangles dan neuritic plaque sesuai umur Tidak ditemukan adanya gangguan klinik dan patologi lainnya yang dapat menyebabkan demensia Gambaran klinis yang tidak menyokong diagnosa DVa meliputi: Defisit memori pada tahap dini, perburukan fungsi memori dan gangguan kognisi lain seperti bahasa (afasia transkortikal sensorik), ketrampilan motorik (apraksia), dan persepsi (agnosia) tanpa adanya lesi yang relevan pada pencitraan otak Tidak ditemukannya defisit neurologis fokal selain gangguan kognis
, ketrampilan motorik (apraksia), dan persepsi (agnosia) tanpa adanya lesi yang relevan pada pencitraan otak. Tidak ditemukannya defisit neurologis fokal selain gangguan kognis.")
23
Terapi ekstrak pegagan dan citicoline
Alur penelitian Consecutive sampling Pasien Stroke Subyek Penelitian Kriteria Inklusi Kriteria Inklusi Sampel Penelitian MoCA-Ina (1) Randomisasi Terapi citicoline Terapi ekstrak pegagan dan citicoline 8 minggu terapi MoCA-Ina(2) MoCA-Ina(2)
 Randomisasi. Terapi citicoline. Terapi ekstrak pegagan dan citicoline. 8 minggu terapi. MoCA-Ina(2) MoCA-Ina(2)")
24
Analisis Statistik Variabel Skala pengukuran Uji Statistik
Jenis terapi/perlakuan Nominal Paired t-test MoCa-Ina Interval Usia Rasio Independent t-test Jenis kelamin Chi-square test

25
Sebuah proses tiada henti

26
Thank You

29
ROC curves showing MoCA© superiority to MMSE in distinguishing Normal Controls from MCI. «The areas under ROC curves were compared with the method of Delong,Delong and Clarke-Pearson (1988) for correlated curves. The difference was statistically significant x2(1,N=182)=11,66, p<0.001.»
 for correlated curves. The difference was statistically significant x2(1,N=182)=11,66, p<0.001.».")
30
Test Result Variable(s) : MoCA Lower BoundUpper BoundLower Bound Area
Area Under the Curve Test Result Variable(s) : MoCA Lower BoundUpper BoundLower Bound Area Std. Error (a) Asymptotic Sig. (b) Asymptotic 95% Interval Upper Bound Lower Bound .921 .020 .000 .882 .960 The test result variable(s): MOCA new has at least one tie between the positive actual state group and the negative actual state group. Statistics may be biased. (a) Under the nonparametric assumption. (b) Null hypothesis: true area = 0.5 Test Result Variable(s) : MMSE Area Std. Error (a) Asymptotic Sig. (b) .814 .032 .751 .876 The test result variable(s): MMSE_num has at least one tie between the positive actual state group and the negative actual state group. Statistics may be biased.
 : MoCA. Lower BoundUpper BoundLower Bound. Area. Std. Error (a) Asymptotic Sig. (b) Asymptotic 95% Interval. Upper Bound. Lower Bound The test result variable(s): MOCA new has at least one tie between the positive actual state group and the negative actual state group. Statistics may be biased. (a) Under the nonparametric assumption. (b) Null hypothesis: true area = 0.5. Test Result Variable(s) : MMSE. Area. Std. Error (a) Asymptotic Sig. (b) The test result variable(s): MMSE_num has at least one tie between the positive actual state group and the negative actual state group. Statistics may be biased.")
31
The Mini-Mental State Examination and Montreal Cognitive Assessment in Persons With Mild Subacute Stroke: Relationship to Functional Outcome Results The MoCA classified more persons as cognitively impaired than the MMSE (89% vs 63%, respectively; using a cutoff score of 27 on the MMSE and 26 on the MoCA). The MoCA also showed less of a ceiling effect than the MMSE, higher internal reliability (Cronbach α=.78 compared with α=.60), and marginally stronger associations with discharge functional status (r=.40; P<.001) than the MMSE (r=0.30; P<.05). The MoCA visuoexecutive subscore was the strongest predictor of functional status (P=.01) and improvement (P=.02) in global and subscores for both tests. Conclusions The MoCA may be an important cognitive screening tool for persons with stroke and mild cognitive dysfunction on an acute rehabilitation unit. Lower visuoexecutive subscores may assist in identifying persons at risk for decreased functional gains in self-care and mobility (mFIM) during inpatient rehabilitation. The findings justify further validation studies of the MoCA in persons with subacute stroke. Toglia,et al.,2011
. The MoCA also showed less of a ceiling effect than the MMSE, higher internal reliability (Cronbach α=.78 compared with α=.60), and marginally stronger associations with discharge functional status (r=.40; P<.001) than the MMSE (r=0.30; P<.05). The MoCA visuoexecutive subscore was the strongest predictor of functional status (P=.01) and improvement (P=.02) in global and subscores for both tests. Conclusions. The MoCA may be an important cognitive screening tool for persons with stroke and mild cognitive dysfunction on an acute rehabilitation unit. Lower visuoexecutive subscores may assist in identifying persons at risk for decreased functional gains in self-care and mobility (mFIM) during inpatient rehabilitation. The findings justify further validation studies of the MoCA in persons with subacute stroke. Toglia,et al.,2011.")
32
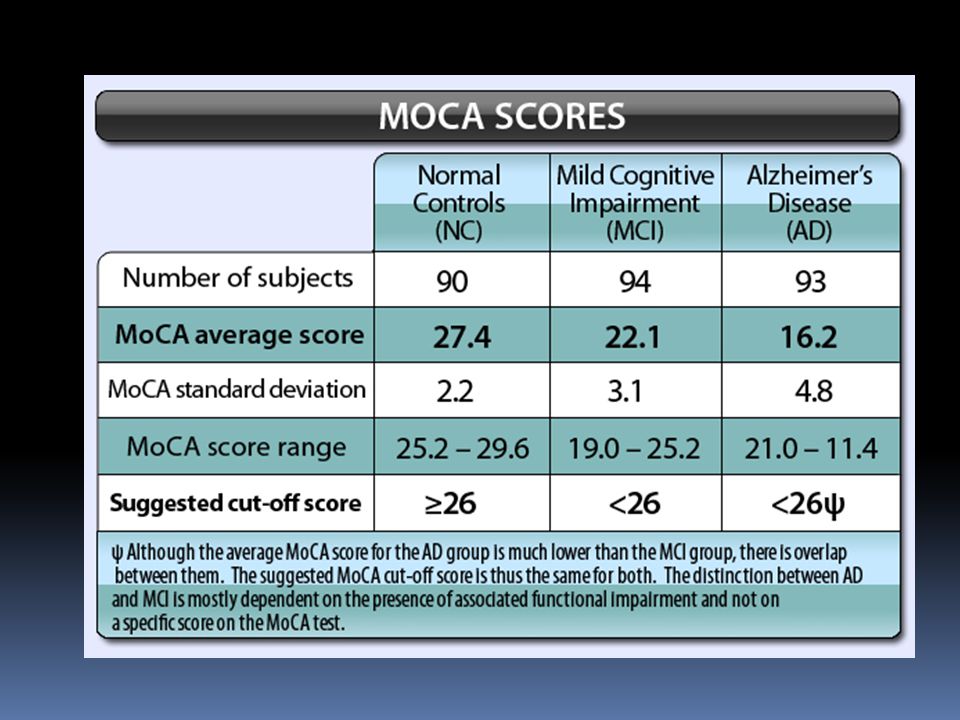
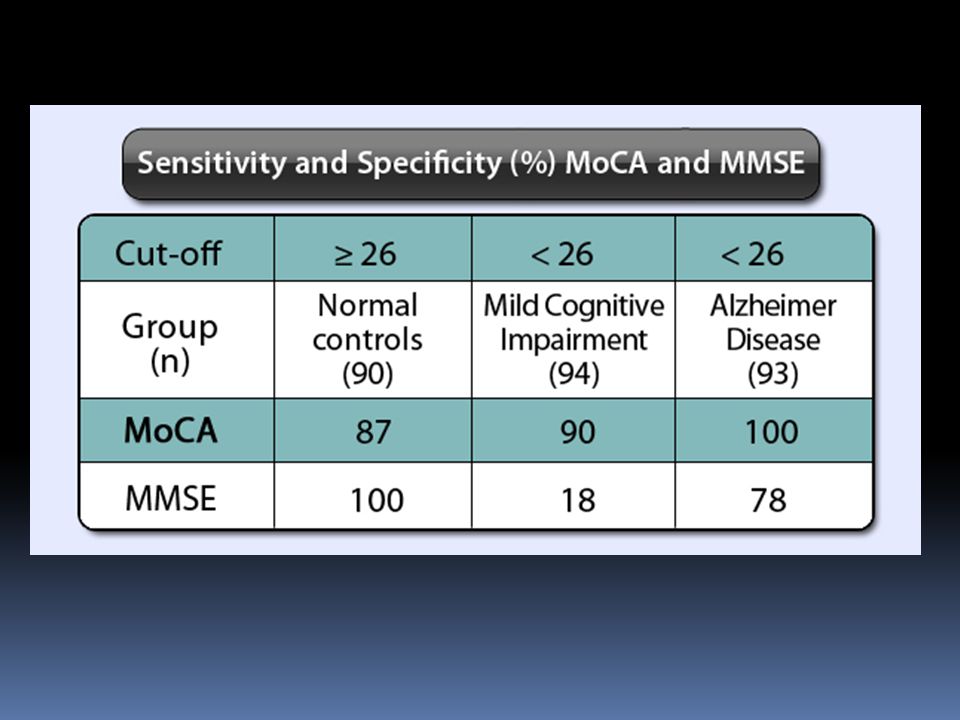
The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. Nasreddine ZS, Phillips NA, Bédirian V, Charbonneau S, Whitehead V, Collin I, Cummings JL, Chertkow H. OBJECTIVES: To develop a 10-minute cognitive screening tool (Montreal Cognitive Assessment, MoCA) to assist first-line physicians in detection of mild cognitive impairment (MCI), a clinical state that often progresses to dementia. PARTICIPANTS: Ninety-four patients meeting MCI clinical criteria supported by psychometric measures, 93 patients with mild Alzheimer's disease (AD) (Mini-Mental State Examination (MMSE) score > or =17), and 90 healthy elderly controls (NC). MEASUREMENTS: The MoCA and MMSE were administered to all participants, and sensitivity and specificity of both measures were assessed for detection of MCI and mild AD. RESULTS: Using a cutoff score 26, the MMSE had a sensitivity of 18% to detect MCI, whereas the MoCA detected 90% of MCI subjects. In the mild AD group, the MMSE had a sensitivity of 78%, whereas the MoCA detected 100%. Specificity was excellent for both MMSE and MoCA (100% and 87%, respectively). CONCLUSION: MCI as an entity is evolving and somewhat controversial. The MoCA is a brief cognitive screening tool with high sensitivity and specificity for detecting MCI as currently conceptualized in patients performing in the normal range on the MMSE.
 to assist first-line physicians in detection of mild cognitive impairment (MCI), a clinical state that often progresses to dementia. PARTICIPANTS: Ninety-four patients meeting MCI clinical criteria supported by psychometric measures, 93 patients with mild Alzheimer s disease (AD) (Mini-Mental State Examination (MMSE) score > or =17), and 90 healthy elderly controls (NC). MEASUREMENTS: The MoCA and MMSE were administered to all participants, and sensitivity and specificity of both measures were assessed for detection of MCI and mild AD. RESULTS: Using a cutoff score 26, the MMSE had a sensitivity of 18% to detect MCI, whereas the MoCA detected 90% of MCI subjects. In the mild AD group, the MMSE had a sensitivity of 78%, whereas the MoCA detected 100%. Specificity was excellent for both MMSE and MoCA (100% and 87%, respectively). CONCLUSION: MCI as an entity is evolving and somewhat controversial. The MoCA is a brief cognitive screening tool with high sensitivity and specificity for detecting MCI as currently conceptualized in patients performing in the normal range on the MMSE.")
33
E€ect of saikosaponin, a triterpene saponin, on apoptosis in lymphocytes: association with c-myc, p53, and bcl-2 mRNA The apoptotic e€ect of saikosaponin-d ( ±1074 M) was also demonstrated by TUNEL analysis and DNA laddering. The percentage of apoptotic cells induced by saikosaponin-d( ±1075 M) was una€ected by the presence of Z-VAD-FMK, indicating that saikosaponin-d-induced apoptosis may not be mediated by caspase activity. However, the percentage of apoptoticcells induced by dexamethasone was signi®cantly reduced by the presence of Z- VAD-FMK. 6 Levels of c-myc, p53, and bcl-2 mRNA were analysed by the reverse transcription-polymerasechain reaction. Levels of c-myc and p53 mRNA were signi®cantly increased, while the level of bcl-2mRNA was decreased, by saikosaponin-d (1075 M) treatment. Dexamethasone did not signi®cantlychange the expression of these genes. 7 It is suggested that the apoptotic e€ect of saikosaponin-d may be partly mediated by increases in c-myc and p53 mRNA levels accompanied by a decrease in bcl-2 mRNA level.
 was also demonstrated by TUNEL analysis and DNA laddering. The percentage of apoptotic cells induced by saikosaponin-d( ±1075 M) was una€ected by the presence of Z-VAD-FMK, indicating that saikosaponin-d-induced apoptosis may not be mediated by caspase activity. However, the percentage of apoptoticcells induced by dexamethasone was signi®cantly reduced by the presence of Z- VAD-FMK. 6 Levels of c-myc, p53, and bcl-2 mRNA were analysed by the reverse transcription-polymerasechain reaction. Levels of c-myc and p53 mRNA were signi®cantly increased, while the level of bcl-2mRNA was decreased, by saikosaponin-d (1075 M) treatment. Dexamethasone did not signi®cantlychange the expression of these genes. 7 It is suggested that the apoptotic e€ect of saikosaponin-d may be partly mediated by increases in c-myc and p53 mRNA levels accompanied by a decrease in bcl-2 mRNA level.")
35
Pharmacological review on Centella asiatica: A potential herbal cure-all
Abstract In recent times, focus on plant research has increased all over the world. Centella asiatica is an important medicinal herb that is widely used in the orient and is becoming popular in the West. Triterpenoid, saponins, the primary constituents of Centella asiatica are manly believed to be responsible for its wide therapeutic actions. Apart from wound healing, the herb is recommended for the treatment of various skin conditions such as leprosy, lupus, varicose ulcers, eczema, psoriasis, diarrhoea, fever, amenorrhea, diseases of the female genitourinary tract and also for relieving anxiety and improving cognition. The present review attempts to provide comprehensive information on pharmacology, mechanisms of action, various preclinical and clinical studies, safety precautions and current research prospects of the herb. At the same time, studies to evaluate the likelihood of interactions with drugs and herbs on simultaneous use, which is imperative for optimal and safe utilization of the herb, are discussed.

36
Active constituents: The primary active constituents of CA are saponins (also called triterpenoids), which include asiaticosides, in which a trisaccharide moiety is linked to the aglycone asiatic acid, madecassoside and madasiatic acid [13] . These triterpene saponins and their sapogenins are mainly responsible for the wound healing and vascular effects by inhibiting the production of collagen at the wound site. Other components isolated from CA, such as brahmoside and brahminoside, may be responsible for CNS and uterorelaxant actions, but are yet to be confirmed by clinical studies. Crude extract containing glycosides isothankuniside and thankuniside showed antifertility action in mice [14],[15] .
![Active constituents: The primary active constituents of CA are saponins (also called triterpenoids), which include asiaticosides, in which a trisaccharide moiety is linked to the aglycone asiatic acid, madecassoside and madasiatic acid [13] .](http://slideplayer.info/slide/1983011/7/images/36/Active+constituents%3A+The+primary+active+constituents+of+CA+are+saponins+%28also+called+triterpenoids%29%2C+which+include+asiaticosides%2C+in+which+a+trisaccharide+moiety+is+linked+to+the+aglycone+asiatic+acid%2C+madecassoside+and+madasiatic+acid+%5B13%5D+..jpg "These triterpene saponins and their sapogenins are mainly responsible for the wound healing and vascular effects by inhibiting the production of collagen at the wound site. Other components isolated from CA, such as brahmoside and brahminoside, may be responsible for CNS and uterorelaxant actions, but are yet to be confirmed by clinical studies. Crude extract containing glycosides isothankuniside and thankuniside showed antifertility action in mice [14],[15] ..")
37
Pathology and pathophysiology of vascular cognitive impairment
Pathology and pathophysiology of vascular cognitive impairment. A critical update. Abstract The prevalence, morphology, and pathogenesis of vascular dementia (VaD), recently termed vascular cognitive impairment (VCI), and of mixed dementia (Alzheimer disease associated with vascular encephalopathy) are a matter of discussion and clinical diagnostic criteria for these disorders slow low sensitivity and variable specificity. In Western memory clinic-based series, VaD/VCI is suggested in 8-10% of cognitively impaired elderly subjects. Its prevalence in autopsy series ranges from 0.03% to 58% with reasonable values of 4-10%. It has been related to focal, multifocal or diffuse cortical and/or subcortical microinfarcts and lacunes often affecting strategically important brain areas (thalamus, frontobasal and/or limbic systems), hemispheric white matter lesions and, less often, large brain infarcts.
, recently termed vascular cognitive impairment (VCI), and of mixed dementia (Alzheimer disease associated with vascular encephalopathy) are a matter of discussion and clinical diagnostic criteria for these disorders slow low sensitivity and variable specificity. In Western memory clinic-based series, VaD/VCI is suggested in 8-10% of cognitively impaired elderly subjects. Its prevalence in autopsy series ranges from 0.03% to 58% with reasonable values of 4-10%. It has been related to focal, multifocal or diffuse cortical and/or subcortical microinfarcts and lacunes often affecting strategically important brain areas (thalamus, frontobasal and/or limbic systems), hemispheric white matter lesions and, less often, large brain infarcts.")
39
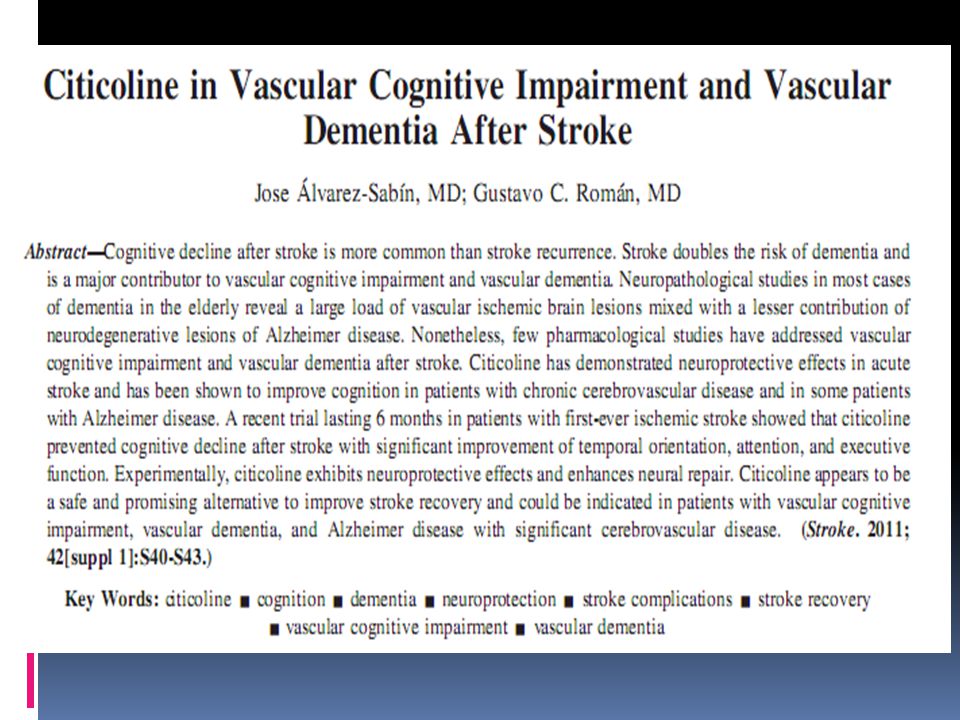
Ischemic Stroke Citicoline has been tested on stroke patients in controlled trials. A multicenter, double-blind, placebocontrolled trial evaluated the effect of citicoline on 272 stroke patients in the acute stage of moderate-to-severe cerebral infarction with mild-to-moderate disturbances in consciousness.21 The treatment group (n=133) received 1,000 mg intravenous (I.V.) citicoline daily for 14 days. Compared to 139 patients on placebo, the level of consciousness improved significantly in the citicoline group. By day 14, 54 percent of patients on citicoline showed improvement, compared to 29 percent of placebo patients.
 received. 1,000 mg intravenous (I.V.) citicoline daily for. 14 days. Compared to 139 patients on placebo, the level. of consciousness improved significantly in the citicoline. group. By day 14, 54 percent of patients on citicoline. showed improvement, compared to 29 percent of placebo. patients.")
40
citicoline A multicenter, double-blind controlled trial conducted by the Citicoline Stroke Study Group examined the effects of oral citicoline on 259 stroke patients. 23 Three doses of citicoline (500 mg, 1,000 mg, or 2,000 mg) were administered (n=65 in each of three groups) within 24 hours of stroke onset, while a fourth group received placebo. Treatment was continued for six weeks, with a six-week follow-up period. The primary clinical endpoint was a change in the Barthel Index of Neurological Function, while baseline NIH Stroke Scale (NIHSS) score was assessed as a secondary variable to decrease the effect of baseline differences in stroke severity.
 were administered (n=65 in each of three groups) within 24 hours of stroke onset, while a fourth group received placebo. Treatment was continued for six weeks, with a six-week follow-up period. The primary clinical endpoint was a change in the Barthel Index of Neurological Function, while baseline NIH Stroke Scale (NIHSS) score was assessed as a secondary variable to decrease the effect of baseline differences in stroke severity.")
43
Cognitive impairment after stroke: clinical determinants and its associations with long-term stroke outcomes. Patel MD, Coshall C, Rudd AG, Wolfe CD. Abstract OBJECTIVES: To identify factors that were associated with cognitive impairment 3 months after stroke, and to examine the associations of cognitive impairment with stroke outcomes up to 4 years after stroke. DESIGN: Observational study. CONCLUSION Cognitive impairment is common 3 months after stroke and is independently associated with older age, ethnicity, lower social class, left hemispheric stroke, visual field defect, and urinary incontinence. It is associated with poor long-term outcomes, including survival and disability, up to 4 years after stroke. Because physical and cognitive impairments after stroke have independent prognostic implications, measures that evaluate both functions should be used in future studies of stroke outcome and in care of stroke patients.

46
Abstract The prevalence, morphology, and pathogenesis of vascular dementia (VaD), recently termed vascular cognitive impairment (VCI), and of mixed dementia (Alzheimer disease associated with vascular encephalopathy) are a matter of discussion and clinical diagnostic criteria for these disorders slow low sensitivity and variable specificity. In Western memory clinic-based series, VaD/VCI is suggested in 8-10% of cognitively impaired elderly subjects. Its prevalence in autopsy series ranges from 0.03% to 58% with reasonable values of 4-10%. It has been related to focal, multifocal or diffuse cortical and/or subcortical microinfarcts and lacunes often affecting strategically important brain areas (thalamus, frontobasal and/or limbic systems), hemispheric white matter lesions and, less often, large brain infarcts.
, recently termed vascular cognitive impairment (VCI), and of mixed dementia (Alzheimer disease associated with vascular encephalopathy) are a matter of discussion and clinical diagnostic criteria for these disorders slow low sensitivity and variable specificity. In Western memory clinic-based series, VaD/VCI is suggested in 8-10% of cognitively impaired elderly subjects. Its prevalence in autopsy series ranges from 0.03% to 58% with reasonable values of 4-10%. It has been related to focal, multifocal or diffuse cortical and/or subcortical microinfarcts and lacunes often affecting strategically important brain areas (thalamus, frontobasal and/or limbic systems), hemispheric white matter lesions and, less often, large brain infarcts.")
Presentasi serupa










 Sindrom polimorfik Ada stresor.>")



>")

>")
>")



