Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
Askep hipoPARAtiroidisme hiperPARAtiroidisme
Nilai normal parathormon: picograms per milliliter (pg/mL) Nilai normal kalsium serum: 9-11 mg/dl Nilai normal fosfor serum: 2,5-4,5 mg/dl (1.7-2,6 mEq/L)
 Nilai normal kalsium serum: 9-11 mg/dl. Nilai normal fosfor serum: 2,5-4,5 mg/dl (1.7-2,6 mEq/L)")
6
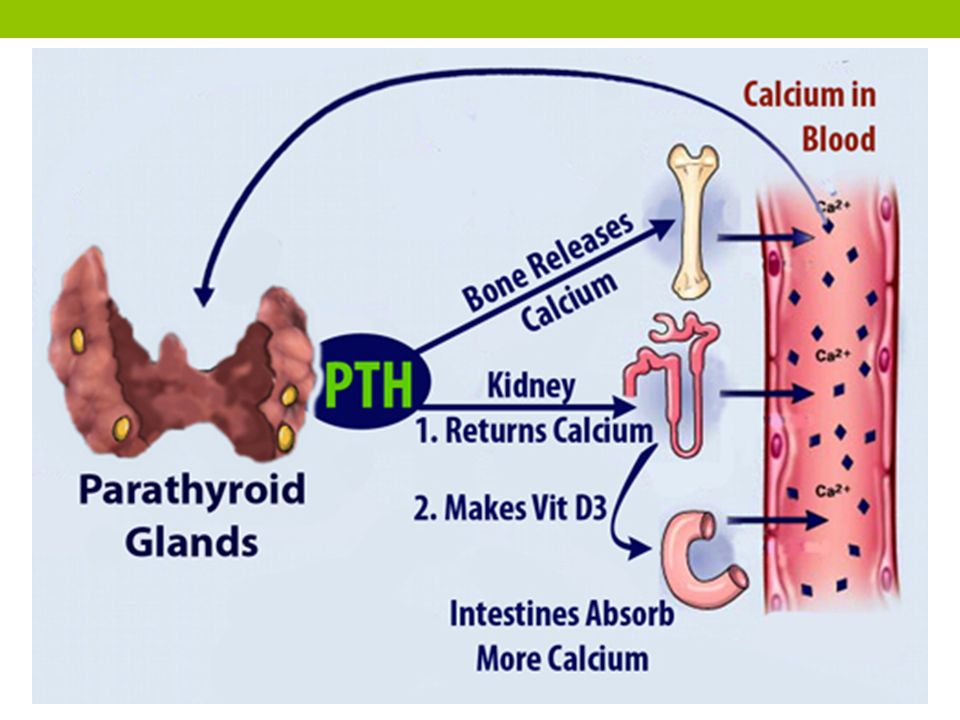
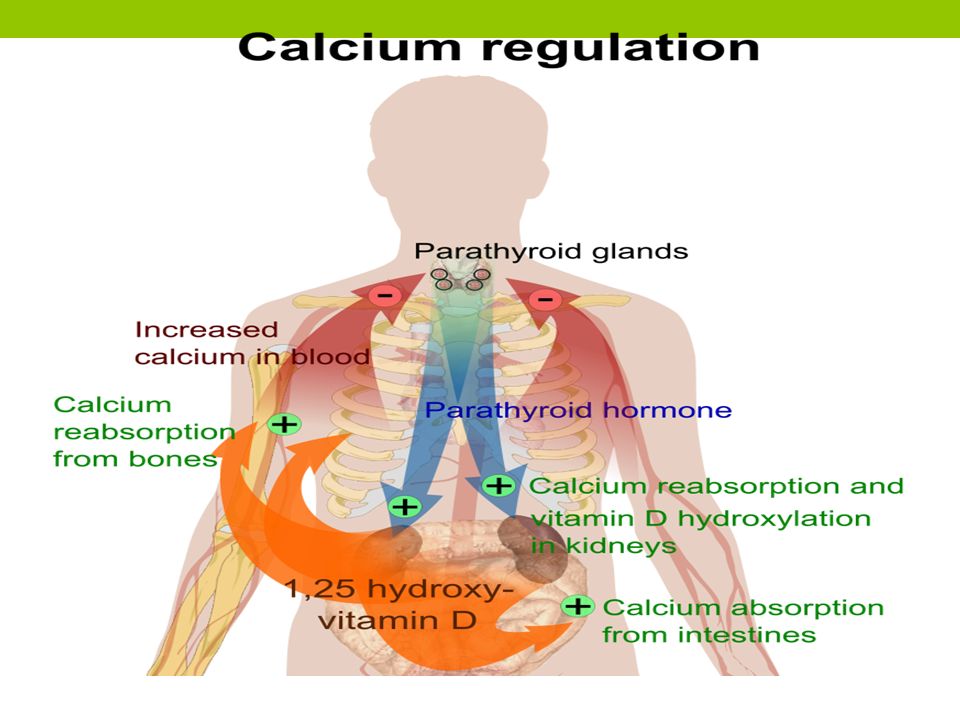
EFEK HORMON PARATIROID (PTH)
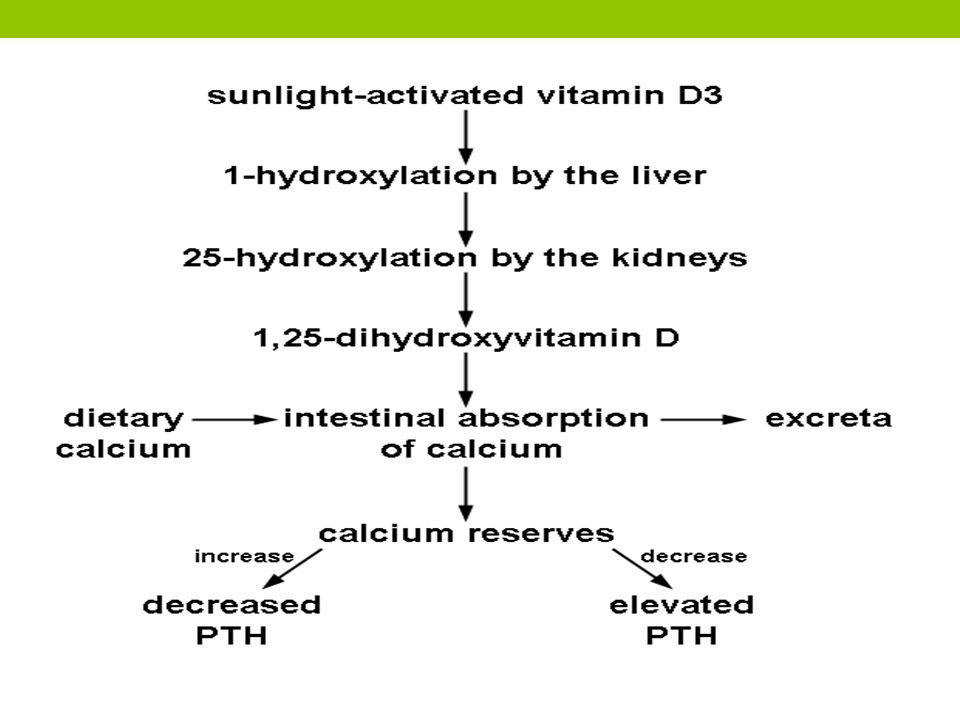
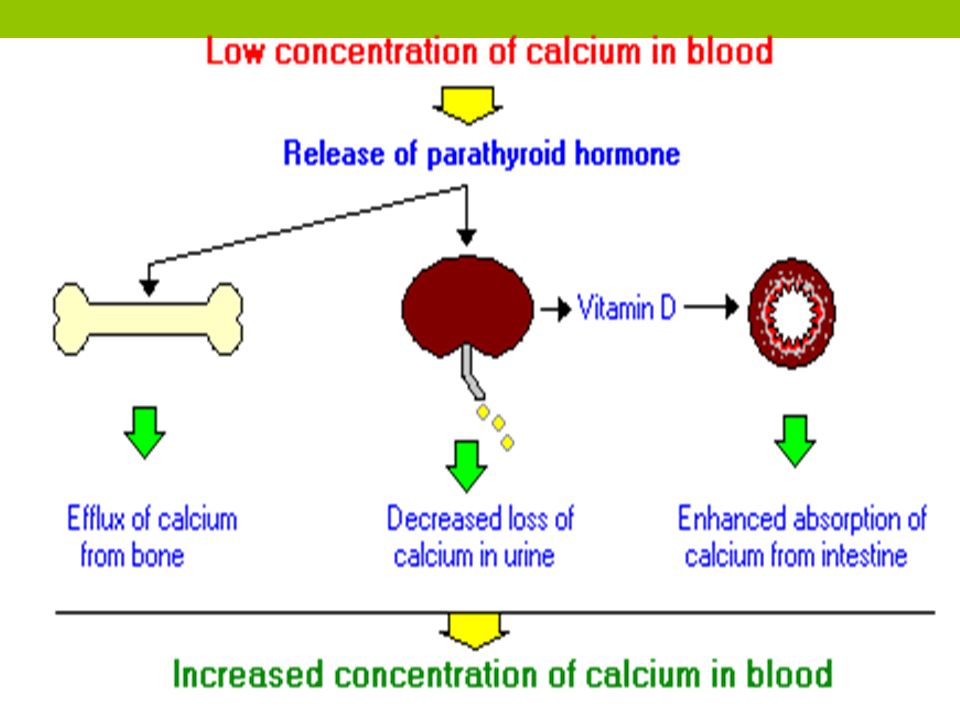
bekerja langsung pada tulang meningkatkan resorpsi tulang dan memobilisasi Ca2+ ke dalam darah meningkatkan kalsium plasma. penurunan reabsorbsi fosfat di tubulus proksimal (efek fosfaturik) meningkatkan ekskresi fosfat dalam urin menurunkan fosfat plasma. meningkatkan reabsorpsi Ca2+ di tubulus distal meningkatkan pembentukan 1,25 dihidroksikolekalsiferol (metabolit vitamin D yang secara fisiologis aktif meningkatkan absorpsi Ca2+ dari usus Role of calcium: strengthening bones and teeth, regulating muscle functioning (contraction and relaxation), the transmission of signals in nerve cells
 meningkatkan ekskresi fosfat dalam urin menurunkan fosfat plasma. meningkatkan reabsorpsi Ca2+ di tubulus distal. meningkatkan pembentukan 1,25 dihidroksikolekalsiferol (metabolit vitamin D yang secara fisiologis aktif meningkatkan absorpsi Ca2+ dari usus. Role of calcium: strengthening bones and teeth, regulating muscle functioning (contraction and relaxation), the transmission of signals in nerve cells.")
7
HIPOPARATIROIDISME Produksi hormon paratiroid yang tidak adekuat
PENYEBAB: Kekurangan sekresi hormon paratiroid (PTH), akibat: kerusakan atau pengangkatan kelenjar paratiroid pada saat operasi paratiroid atau tiroid Radiasi area leher Proses autoimun Tidak adanya kelenjar paratiroid (secara kongenital) Level magnesium yang rendah normal magnesium diperlukan untuk sekresi optimal dari paratiroid idiopatik
, akibat: kerusakan atau pengangkatan kelenjar paratiroid pada saat operasi paratiroid atau tiroid. Radiasi area leher. Proses autoimun. Tidak adanya kelenjar paratiroid (secara kongenital) Level magnesium yang rendah normal magnesium diperlukan untuk sekresi optimal dari paratiroid. idiopatik.")
8
Manifestasi klinik Gejala tetanus spasmodik: tremor, timbul gerakan tubuh tak terkoordinasi Gejala tetanus laten: kesemutan, kram pada kaki, kekakuan ekstremitas Gejala tetanus terbuka: bronkospasme, spasme laring, spasme karpopedal, disfagia, fotofobia, aritmia jantung, kejang Gejala lain: cemas, iritabilitas, depresi, delirium. Perubahan pada EKG dan hipotensi dapat terjadi

9
CARPOPEDAL SPASM: contraction of the muscles of the hands and feet or especially of the wrists and ankles

10
Signs and symptoms of neuromuscular irritability:
Paresthesia (involving fingertips, toes, perioral area) Hyperirritability Fatigue Anxiety Mood swings and/or personality disturbances Seizures (especially in patients with epilepsy) Hoarseness (due to laryngospasm) Wheezing and dyspnea (due to bronchospasm) Muscle cramps, diaphoresis, and biliary colic Hypomagnesemia, hypokalemia, and alkalosis (eg, hyperventilation), which worsen signs and symptoms of hypocalcemia
 Hyperirritability. Fatigue. Anxiety. Mood swings and/or personality disturbances. Seizures (especially in patients with epilepsy) Hoarseness (due to laryngospasm) Wheezing and dyspnea (due to bronchospasm) Muscle cramps, diaphoresis, and biliary colic. Hypomagnesemia, hypokalemia, and alkalosis (eg, hyperventilation), which worsen signs and symptoms of hypocalcemia.")
11
Pemeriksaan Diagnostik
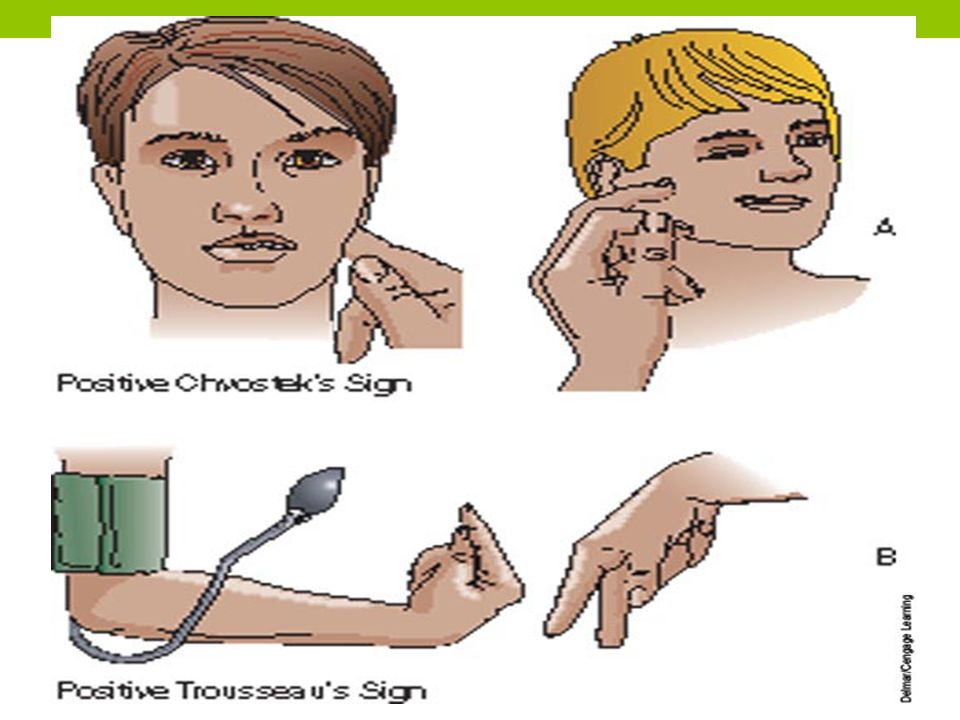
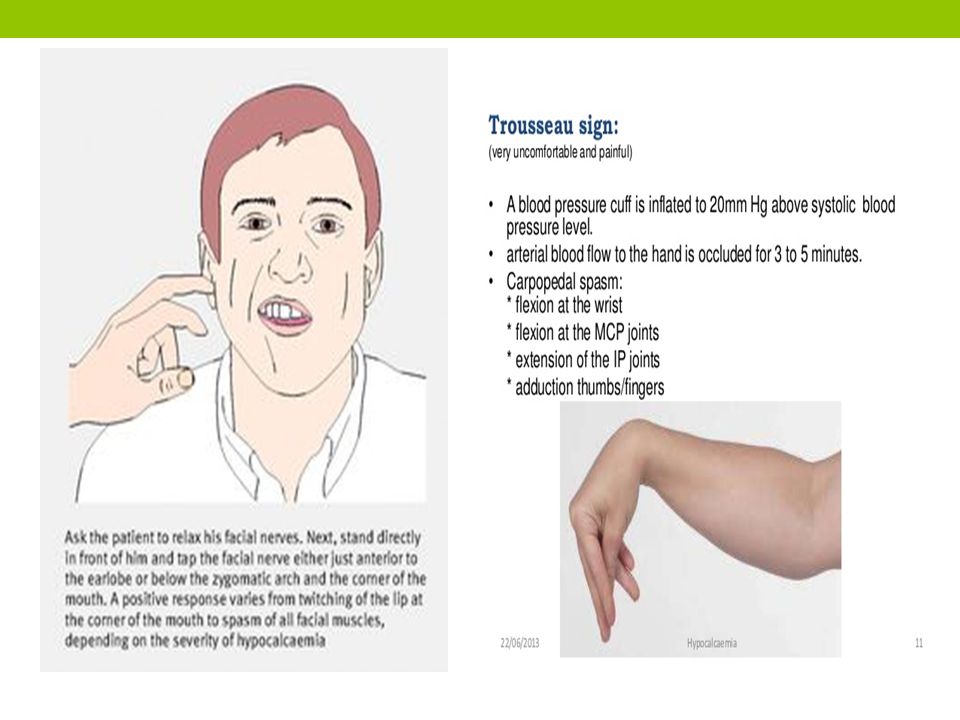
Erb’s sign Dengan stimulasi listrik kurang dari 5 milli-ampere sudah ada kontraksi dari otot (normal pada 6 milli-ampere) Chvostek’s sign Ketokan ringan pada nervus fasialis menyebabkan kontraksi dari otot-otot wajah. Trousseau’s sign Jika sirkulasi darah dilengan ditutup dengan manset (lebih dari tekanan sistolik) maka dalam tiga menit tangan mengambil posisi spasme carpopedal. Peroneal sign Dengan mengetok bagian lateral fibula akan terjadi dorsofleksi dan adduksi dari kaki.
 Chvostek’s sign. Ketokan ringan pada nervus fasialis menyebabkan kontraksi dari otot-otot wajah. Trousseau’s sign. Jika sirkulasi darah dilengan ditutup dengan manset (lebih dari tekanan sistolik) maka dalam tiga menit tangan mengambil posisi spasme carpopedal. Peroneal sign. Dengan mengetok bagian lateral fibula akan terjadi dorsofleksi dan adduksi dari kaki.")
14
Pemeriksaan penunjang
Didapatkan: A low blood-calcium level A low parathyroid hormone level A high blood-phosphorus level A low blood-magnesium level Kalsium serum rendah. Tetanus terjadi pada kadar kalsium yang berkisar mg/dl (1,2 - 1,5 mmol/L) atau lebih rendah lagi. Kadar fosfat dalam serum meningkat Rontgen: Densitas dari tulang bisa bertambah EKG: biasanya QT-interval lebih panjang.
 atau lebih rendah lagi. Kadar fosfat dalam serum meningkat. Rontgen: Densitas dari tulang bisa bertambah. EKG: biasanya QT-interval lebih panjang.")
15
Penatalaksanaan Meningkatkan tingkat kalsium serum
Pemberian kalsium glukonat intravena Obat penenang seperti pentobarbital mungkin diberikan Pengaturan lingkungan yang bebas dari kebisingan, cahaya terang, atau gerakan tiba-tiba. Pemberian parathormon parenteral Gejala kesulitan pernafasan trakeostomi atau ventilasi mekanis, bronchodilating obat Diet tinggi kalsium dan rendah fosfor Pemberian vitamin D untuk meningkatkan absorbsi Kalsium di usus

16
Treatments and drugs Dietary
Oral calcium carbonate tablets. Oral calcium supplements can increase calcium levels. However, at high doses, calcium supplements can cause gastrointestinal side effects, such as constipation, in some people. Vitamin D. High doses of vitamin D, generally in the form of calcitriol, can help body absorb calcium and eliminate phosphorus. Dietary Rich in calcium. This includes dairy products, green leafy vegetables, broccoli, kale, and fortified orange juice and breakfast cereals. Low in phosphorus-rich items avoiding carbonated soft drinks, which contain phosphorus in the form of phosphoric acid, and limiting eggs and meats.

17
Diagnosa keperawatan Ineffective airway clearance related to laryngospasm Activity intolerance related to fatigue/weakness, Decreased cardiac output related to cardiac dysrhythmias Risk for injury related to tetany, muscle weakness

18
Intervensi Evaluasi keadekuatan jalan nafas
Kaji adanya penurunan kalsium Perhatikan adanya tanda Chvostek's and trosseaus yang positif Perawatan kulit karena kulit biasanya kering Berikan bantalan pada side rail tempat tidur karena pasien bisa mengalami kejang Komunikasi dengan pasien karena pasien dapat mengalami gangguan memori Sediakan lingkungan yang tidak menstimulasi kejang

19
HIPERPARATIROIDISME Berlebihnya produksi hormon paratiroid
Etiologi: adenoma, hiperplasia

20
Primary hyperparathyroidism
Primary hyperparathyroidism occurs because of some problem with one or more of the four parathyroid glands: A noncancerous growth (adenoma) on a gland is the most common cause. Enlargement (hyperplasia) of two or more parathyroid glands accounts for most other cases. A cancerous (malignant) tumor is a rare cause of primary hyperparathyroidism. Primary hyperparathyroidism usually occurs randomly, but some people inherit a gene that causes the disorder.
 on a gland is the most common cause. Enlargement (hyperplasia) of two or more parathyroid glands accounts for most other cases. A cancerous (malignant) tumor is a rare cause of primary hyperparathyroidism. Primary hyperparathyroidism usually occurs randomly, but some people inherit a gene that causes the disorder.")
21
Hiperparatiroid primer
Etiologi: adenoma, hiperplasia Terjadi peningkatan kadar hormon paratiroid serum, peningkatan kalsium serum (hiperkalsemia) dan penurunan fosfat serum. Hiperkalsemia anoreksia, nausea, muntah, konstipasi, berat badan menurun, lekas lelah, otot-otot lemah, perubahan mental. Sebagai akibat kalsifikasi viseral, kalsifikasi pada ginjal berupa kalkuli (batu ginjal), nefrokalsinosis. Peningkatan resorbsi tulang nyeri tulang dan deformitas, fraktur patologis
 dan penurunan fosfat serum. Hiperkalsemia anoreksia, nausea, muntah, konstipasi, berat badan menurun, lekas lelah, otot-otot lemah, perubahan mental. Sebagai akibat kalsifikasi viseral, kalsifikasi pada ginjal berupa kalkuli (batu ginjal), nefrokalsinosis. Peningkatan resorbsi tulang nyeri tulang dan deformitas, fraktur patologis.")
22
Secondary hyperparathyroidism
Secondary hyperparathyroidism is the result of another condition that lowers calcium levels. Factors that may contribute to secondary hyperparathyroidism include: Severe calcium deficiency. not enough calcium from diet, digestive system doesn't absorb the calcium. Severe vitamin D deficiency. Vitamin D helps maintain appropriate levels of calcium in the blood, and it helps digestive system absorb calcium from food. Chronic kidney failure. kidneys convert vitamin D into a form that body can use. If kidneys function poorly, usable vitamin D may decline and calcium levels drop. Chronic kidney failure is the most common cause of secondary hyperparathyroidism.

23
Hiperparatiroidisme sekunder
Produksi hormon paratiroid yang berlebihan karena rangsangan produksi yang tidak normal Terjadi hiperplasia kompensatorik untuk mengoreksi penurunan kadar kalsium serum Terjadi penurunan kadar kalsium serum, kadar PTH tinggi, fosfat serum tinggi kemudian menurun. berkaitan dengan gagal ginjal akut, kekurangan vitamin D, gangguan penyerapan Kalsium Gagal ginjal menurun fungsi ginjal dalam ekskresi fosfat retensi fosfat menekan kadar kalsium memicu sekresi PTH Gagal ginjal gangguan perubahan vitamin D menjadi 1,25 dihidroksi gangguan penyerapan kalsium kalsium serum rendah memicu sekresi PTH PTH menarik kalsium dari tulang

24
Signs and symptoms of hyperparathyroidism
Fragile bones that easily fracture (osteoporosis) Kidney stones Excessive urination Abdominal pain Tiring easily or weakness Depression or forgetfulness Bone and joint pain Frequent complaints of illness with no apparent cause Nausea, vomiting or loss of appetite
 Kidney stones. Excessive urination. Abdominal pain. Tiring easily or weakness. Depression or forgetfulness. Bone and joint pain. Frequent complaints of illness with no apparent cause. Nausea, vomiting or loss of appetite.")
25
Tanda dan gejala Cepat lelah (Letargi);
Penurunaan tonus otot sehingga otot menjadi lemah; Konstipasi, yang disebabkan oleh gangguan reabsorsi kalsium di usus dan penurunan peristaltik usus; Reabsorbsi kalsium dari tulang meningkat sehingga terjadi hiperkalsemia dalam darah; Hiperkalsemia menyebabkan poliuri dan polidipsi, neprolithiasis ginjal, pankreatitis, ulkus peptikum Resorbsi kalsium tulang meningkat sehingga tulang mudah fraktur di berbagai tempat Nyeri pinggang karena batu ginjal; Henti jantung karena krisis hiperkalsemia

26
Pemeriksaan diagnostik
Hasil Laboratorium: Kalsium serum meninggi Fosfat serum rendah Fosfatase alkali meninggi Kalsium dalam urin bertambah Foto Rontgen: tulang menjadi tipis, ada dekalsifikasi

27
Penatalakasanaan Medis
Operasi pengangkatan paratiroid yang mengalami pembesaran (adenoma) Surgery is the most common treatment for primary hyperparathyroidism and provides a cure in about 95 percent of all cases. Medikamentosa, menghalangi destruksi kalsium dan fosfor tubuh, pemberian furosemid Medications: Calcimimetics. A calcimimetic is a drug that mimics calcium circulating in the blood. The drug may trick the parathyroid glands into releasing less parathyroid hormone. This drug is sold as cinacalcet (Sensipar). Hormone replacement therapy. For women who have gone through menopause and have signs of osteoporosis, hormone replacement therapy may help bones retain calcium. Bisphosphonates. Bisphosphonates also prevent the loss of calcium from bones and may lessen osteoporosis caused by hyperparathyroidism. Some side effects associated with bisphosphonates include low blood pressure, fever and vomiting.
 Surgery is the most common treatment for primary hyperparathyroidism and provides a cure in about 95 percent of all cases. Medikamentosa, menghalangi destruksi kalsium dan fosfor tubuh, pemberian furosemid. Medications: Calcimimetics. A calcimimetic is a drug that mimics calcium circulating in the blood. The drug may trick the parathyroid glands into releasing less parathyroid hormone. This drug is sold as cinacalcet (Sensipar). Hormone replacement therapy. For women who have gone through menopause and have signs of osteoporosis, hormone replacement therapy may help bones retain calcium. Bisphosphonates. Bisphosphonates also prevent the loss of calcium from bones and may lessen osteoporosis caused by hyperparathyroidism. Some side effects associated with bisphosphonates include low blood pressure, fever and vomiting.")
28
Diagnosa keperawatan Fatigue berhubungan dengan kelemahan otot
Ketidakseimbangan nutrisi kurang dari kebutuhan tubuh berhubungan dengan intake tidak adekuat Resiko cedera: fraktur patologis berhubungan dengan dekalsifikasi tulang

29
Nursing intervention Monitor level serum potassium, calcium, phosphate, and magnesium sebelum treatment. Lakukan tindakan pencegahan untuk meminimalkan resiko jatuh Jadwalkan aktivitas yang memungkinkan pasien dengan kelemahan otot dapat beristirahat sebaik mungkin Sediakan tindakan yang membuat nyaman untuk meredakan nyeri tulang Berikan antasid dengan tepat untuk mencegah ulkus peptikum Auskultasi suara paru untuk mengetahui adanya edema pulmo Cek peningkatan level kalsium serum jika pasien mendapatkan glikosida jantung Kaji tingkat nyeri dan monitor keefektifan analgesik dan tindakan yang membuat nyaman

30
QUESTIONS 1) A client diagnosed with primary hyperparathyroidism demonstrates that she understands the teaching plan when the client makes which of the following statements? (1) “I know I must have surgery to remove my parathyroid gland.” (2) “I must take diuretics the rest of my life.” (3) “I must eat a diet low in potassium.” (4) “I must limit my daily fluid intake.” Answer: 1 Rationale: The treatment for primary hyperparathyroidism is a parathyroidectomy (surgical removal of parathyroid glands). Options 2, 3, and 4 are incorrect treatments for primary hyperparathyroidism.
 A client diagnosed with primary hyperparathyroidism demonstrates that she understands the teaching plan when the client makes which of the following statements (1) I know I must have surgery to remove my parathyroid gland. (2) I must take diuretics the rest of my life. (3) I must eat a diet low in potassium. (4) I must limit my daily fluid intake. Answer: 1. Rationale: The treatment for primary hyperparathyroidism is a parathyroidectomy (surgical removal of parathyroid glands). Options 2, 3, and 4 are incorrect treatments for primary hyperparathyroidism.")
31
2) The priority nursing diagnosis for a client with hypoparathyroidism would be which of the following? (1) Risk for fluid volume excess (2) Risk for injury (3) Anxiety related to lack of knowledge (4) Knowledge deficit Answer: 2 Rationale: Risk for injury related to hypocalcemia is the priority diagnosis as injury may occur as a result of low calcium levels and tetany. The client is at risk for fluid volume deficit, and anxiety and knowledge deficit would not be a priority over injury.
 Risk for fluid volume excess. (2) Risk for injury. (3) Anxiety related to lack of knowledge. (4) Knowledge deficit. Answer: 2. Rationale: Risk for injury related to hypocalcemia is the priority diagnosis as injury may occur as a result of low calcium levels and tetany. The client is at risk for fluid volume deficit, and anxiety and knowledge deficit would not be a priority over injury.")
32
3) In providing care for a client being admitted for hyperparathyroidism, the nurse anticipates implementing which of the following aactions? (1) Administering intravenous calcium gluconate (2) Administering large amounts of intravenous saline (3) Maintaining strict fluid restriction (4) Monitoring for tetany Answer: 2 Rationale: Hypercalcemia is the primary complication of hyperparathyroidism, and the manifestations of the disorder are directly related to the effects of hypercalcemia. Administering large amounts of intravenous saline promotes renal excretion of calcium. Calcium gluconate would increase serum calcium levels, and tetany is a symptom of hypocalcemia
 Administering intravenous calcium gluconate. (2) Administering large amounts of intravenous saline. (3) Maintaining strict fluid restriction. (4) Monitoring for tetany. Answer: 2. Rationale: Hypercalcemia is the primary complication of hyperparathyroidism, and the manifestations of the disorder are directly related to the effects of hypercalcemia. Administering large amounts of intravenous saline promotes renal excretion of calcium. Calcium gluconate would increase serum calcium levels, and tetany is a symptom of hypocalcemia")
33
CASE STUDY Case 1 A female patient, 41 years old, was hospitalized in the Oncology Clinic in February 2003 with suspicion on multiple bone metastases, and a tumor in the pelvis (CT verified). A detailed anamnesis showed that the patient had four spontaneous fractures (foot, clavicle, upper arm, forearm) four years before. She had not been examined in the sense of determining the etiology of the fractures. She complained about gastric problems for many years accompanied by minor loss of weight. She also reported poor appetite, nausea and vomiting every day during the last several months, constipation (up to 10 days), regular urination. Menstrual cycles were irregular. Three years before she had a maxilofacial operation in a specialized institution when a resection of the jaw was performed because of cystic changes. A few months after coming to hospital, she felt pains in the lumbar part of the spine and in pelvis with pains spreading to both legs. Difficulties in walking, numbness, and dull pain were becoming more intense, and soon she was confined to bed. Then, she was transferred to the Neurology Clinic. Because of suspected bone metastases (CT of skeleton) she was transferred to the Oncology Clinic. Extremities were painful on palpation and movement, fractures were conservatively treated by plaster fixation. Based on the detailed anamnestic data, objective findings and analysis performed before the patient was hospitalized at the Oncology Clinic,a working diagnosis of primary hyperparathyroidism was made and further examination was conducted in that direction. ECHO of abdomen and kidneys: in both kidneys a few small stones, other findings were regular. The patient was transferred to the Institute of Endocrinology in where she was operated on April 17, OP: Parathyreoidectomia. In the postoperative period, the patient felt much better. She had good appetite, she was gaining weight, stools were regular. Menstrual cycle was normalized two months after operation. With the application of symptomatic therapy, laboratory analysis were within the limits of referred values. A year after the operation, the patient walks without help, she has gained 15kg, and does not complain of any discomfort.
. A detailed anamnesis showed that the patient had four spontaneous fractures (foot, clavicle, upper arm, forearm) four years before. She had not been examined in the sense of determining the etiology of the fractures. She complained about gastric problems for many years accompanied by minor loss of weight. She also reported poor appetite, nausea and vomiting every day during the last several months, constipation (up to 10 days), regular urination. Menstrual cycles were irregular. Three years before she had a maxilofacial operation in a specialized institution when a resection of the jaw was performed because of cystic changes. A few months after coming to hospital, she felt pains in the lumbar part of the spine and in pelvis with pains spreading to both legs. Difficulties in walking, numbness, and dull pain were becoming more intense, and soon she was confined to bed. Then, she was transferred to the Neurology Clinic. Because of suspected bone metastases (CT of skeleton) she was transferred to the Oncology Clinic. Extremities were painful on palpation and movement, fractures were conservatively treated by plaster fixation. Based on the detailed anamnestic data, objective findings and analysis performed before the patient was hospitalized at the Oncology Clinic,a working diagnosis of primary hyperparathyroidism was made and further examination was conducted in that direction. ECHO of abdomen and kidneys: in both kidneys a few small stones, other findings were regular. The patient was transferred to the Institute of Endocrinology in where she was operated on April 17, OP: Parathyreoidectomia. In the postoperative period, the patient felt much better. She had good appetite, she was gaining weight, stools were regular. Menstrual cycle was normalized two months after operation. With the application of symptomatic therapy, laboratory analysis were within the limits of referred values. A year after the operation, the patient walks without help, she has gained 15kg, and does not complain of any discomfort.")
34
Case 2 A 30 year old male, was presented to the emergency facility in an unconscious condition. He was intubated on the way to the hospital as he had suffered from two episodes of ventricular tachycardia. He had previous history of recurrent seizures for 6 years inspite of multiple anticonvulsants including phenytoin sodium, sodium valproate, and levetiracetam. The seizure frequency increased in the last year and he would have 5-6 episodes/ month. A MRI brain scan and EEG at the onset were both normal, as was the general examination but he had history of bilateral cataracts. There were no signs of tetany. Investigations revealed a normal hemoglobin and glucose level with normal electrolytes. He had a serum calcium level of 3.3 mg% with a serum parathyroid hormone level of 1pg/ml, serum 25(OH) vitamin D levels of 6.6ng/ml and hypomagnesemia. Head scan showed bilateral basal ganglia, and deep white matter calcification. Patient was diagnosed with primary hypoparathyroidism.
 vitamin D levels of 6.6ng/ml and hypomagnesemia. Head scan showed bilateral basal ganglia, and deep white matter calcification. Patient was diagnosed with primary hypoparathyroidism.")
Presentasi serupa










>")



>")


 Hidsal Jamil(135020100111028) Padel Aji Pamungkas(135020100111042)>")

