Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
Fisiologi dan Patofisiologi Proses Berkemih
dr. Bobby Hery Yudhanto, SpU

2
Anatomi traktus urinarius laki-laki

3
Anatomy and relations of the bladder, urethra, uterus and ovary, vagina, and rectum

4
Sistem Persarafan Traktus Urinarius dan Traktus Digestivus

5
Physiology Main function of bladder : 1. Urine storage
2. Urine voiding Ada 2 faktor yang berpengaruh dalam proses miksi : 1. Buli – buli (kandung kemih) sebagai “pompa” 2. Saluran kemih bagian bawah, meliputi bladder neck, prostat, sphincter urethra externa dan urethra sebagai “ jalan keluar urine”
 sebagai pompa 2. Saluran kemih bagian bawah, meliputi bladder neck, prostat, sphincter urethra externa dan urethra sebagai jalan keluar urine")
6
Neuroanatomy and Neurophysiology of micturition :
A. Peripheral : 1. Sympathetic : Filling /storage 2. Parasympathetic : voiding / emptying 3. Somatic : external sphincter B. Central : four loops in Brain, Brainstem, Spinal cord

7
Peripheral innervation :
Afferents : from detrusor stretch receptors, sphincter, perineum, genitalia Efferents : a. Parasympathetic S2 – S4 Receptors : Cholinergic – muscarinic ( at body of the bladder ) b. Sympathetic : T11 – L2 Receptors : Alpha adrenergic ( at sphincter) Beta adrenergic ( at body of the bladder)
 b. Sympathetic : T11 – L2. Receptors : Alpha adrenergic ( at sphincter) Beta adrenergic ( at body of the bladder)")
8
Central Innervation : Loop I : Corticopontine-mesencephalic nuclei
From frontal lobe Exerts inhibitory influence on parasympathetic Sacral Micturition Center (SMS) bladder storage Lesions here detrusor hyperreflexia Loop II : Pontine-mesencephalic-sacral nuclei Pontine Micturition Center (PMC) To coordinate efficient detrusor and sphincter interaction Lesions here and down DSD
 bladder storage. Lesions here detrusor hyperreflexia. Loop II : Pontine-mesencephalic-sacral nuclei. Pontine Micturition Center (PMC) To coordinate efficient detrusor and sphincter interaction. Lesions here and down DSD.")
9
Central innervartion……..
3. Loop III : Pelvic-Pudendal nuclei : “Sacral Micturition Center (SMC) Lesions here areflexic / atonic bladder 4. Loop IV : Motor Cortex to pudendal nuclei Responsible for the voluntary control of the external sphincter
 Lesions here areflexic / atonic bladder. 4. Loop IV : Motor Cortex to pudendal nuclei. Responsible for the voluntary control of the external sphincter.")
10
Innervation of Lower Urinary Tract
Bladder- cholinergic parasympathetic- contraction; beta-adrenergic & NO– relaxation Bladder neck – alpha-adrenergic- contration Urethral muscles- cholinergic parasympathetic, NO, cholinergic somatic nerves

11
Innervation of the bladder
Sympathetic nerve supply Parasympathetic nerve supply S2 S3 S4 L1 L2 L3 Pelvic nerve Sympathetic chain Hypogastric ganglion nerve Somatic nerve supply S2 S3 S4 Urethra External sphincter Pudendal nerve

12
BLADDER FILLING

13
Physiology of Urine Storage
First sensation of filling Fullness sensation Urge sensation Premicturition urge sensation- phasic detrusor contraction Increased activity of urethral sphincter during filling

14
Fase Pengisian Buli Terjadi relaksasi dari buli-buli dan kontraksi dari bladder neck (dipengaruhi oleh saraf simpatis) Volume buli pada usia dewasa muda sekitar 500cc. Pada volume sekitar 150cc sudah ada rangsangan untuk berkemih Pada volume 300cc rangsangan untuk berkemih semakin kuat yang disertai pembukaan bladder neck secara spontan. Proses miksi masih bisa ditahan melalui sphincter urethra externa (bisa diatur secara sadar/voluntary)
")
15
BLADDER EMPTYING

16
Fase Pengosongan Buli (berkemih)
Dipengaruhi oleh sistem saraf parasimpatis Terjadi relaksasi dari otot sphincter urethra externa dan bladder neck. Kemudian diikuti oleh kontraksi otot-otot detrusor Buli. Terjadi pengosongan buli sehingga volume urine di dalam buli-buli tidak tersisa atau residu urine kurang dari 50cc

17
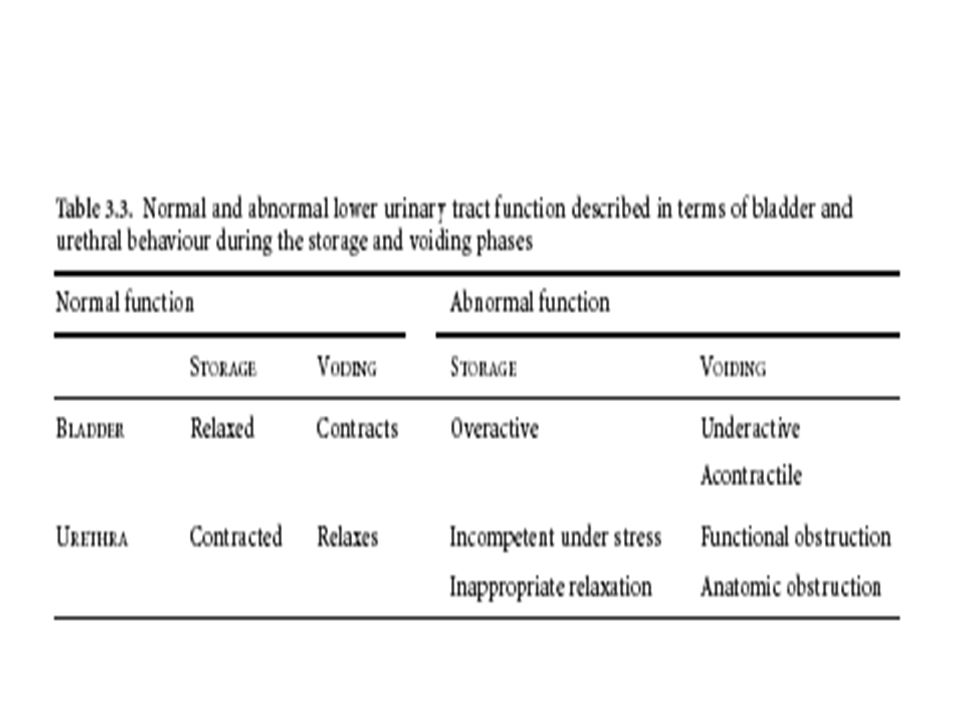
Bladder filling and urine storage require:
1. Accommodation of increasing volumes of urine at a low intravesical 2. A bladder outlet that is closed at rest and remains so during increases pressure and with appropriate sensation in intra-abdominal pressure 3. Absence of involuntary bladder contractions. Bladder emptying requires: 1. A coordinated contraction of the bladder smooth musculature of adequate magnitude 2. A concomitant lowering of resistance at the level of the smooth and striated sphincter. 3. Absence of anatomic (as opposed to functional) obstruction.
 obstruction.")
18
Micturition detrusor pressure- depends on urethral resistance
High voiding pressure indicates a greater urethral resistance Low voiding pressure indicates a lower urethral resistance or a low detrusor contractility Efficient bladder empty depends on a sustained detrusor contraction

19
Efficient Bladder Empty
Hypersensitive bladder- low detrusor contractility Inadequate contractility in elderly Bladder outlet obstruction- Bladder neck dysfunction, Prostatic enlargement, Urethral stricture, Cystocele, External sphincter dyssynergia

21
Abnormalities of micturition
Atonic bladder This is due to destruction of sensory nerve fibers from urinary from the bladder. When the dorsal sacral roots are interrupted by diseases of the dorsal roots such as tabes dorsalis or when there is crush injury to sacral segments of spinal cord, person looses bladder control (abolition of reflex contractions of the bladder). Bladder muscle looses the tone (hypotonic) and becomes flaccid). Bladder fills to the capacity and overflows few drops at a time through the urethra (overflow incontinence or overflow dribbling).
. Bladder muscle looses the tone (hypotonic) and becomes flaccid). Bladder fills to the capacity and overflows few drops at a time through the urethra (overflow incontinence or overflow dribbling).")
22
2. Automatic bladder (Spastic neurogenic bladder)
During spinal shock after complete transection of spinal cord above sacral centres of micturition, the urinary bladder looses its tone and becomes flaccid and unresponsive. So, the bladder is completely filled, and later urine overflows by dribbling. After the spinal shock has passed, the voiding reflex returns although there is no voluntary and higher centre control. Whenever, the bladder is filled with some amount of urine, there is automatic evacuation of the bladder.

23
Spinal Cord injury Abnormality in micturition cycle depend spinal cord injury’s level : Above brain stem detrusor hyperreflexia Above S2 segment detrusor hyperreflexia with detrusor external sphincter dyssynergia (DESD) Below S2 segment detrusor areflexia with fixed sphincter urethral external tone
 Below S2 segment detrusor areflexia with fixed sphincter urethral external tone.")
24
3. Uninhibited neurogenic bladder
Due to a lesion in some parts of brain stem (interrupting mst of the inhibitory signals), there is continuous excitation of spinal micturition centres by the higher centres. There is uncontrollable micturition. Even a small quantity of urine collected in bladder will elicit the micturition reflex increasing the frequency of micturition.
, there is continuous excitation of. spinal micturition centres by the higher centres. There is. uncontrollable micturition. Even a small quantity of urine. collected in bladder will elicit the micturition reflex increasing. the frequency of micturition.")
25
4. Nocturnal micturition (Bed wetting)
This is normal in infants and children below 3 years. It occurs due to incomplete myelination of motor nerve fibers of the bladder resulting loss of voluntary control of micturition .

26
Traktus Urinarius Bawah
Gejala Iritatif Frekuensi Frekuensi normal miksi orang dewasa sebanyak 5-6x/hari dengan setiap miksi sebanyak 300cc Penyebab : penurunan kapasitas buli-buli termasuk bladder outlet obstruction dengan penurunan daya regang buli, peningkatan residu urine, dan/atau penurunan kapasitas fungsional buli karena iritasi neurogenic bladder dengan peningkatan sensitivitas dan penurunan daya regang buli penekanan dari luar anxietas. Disuria : nyeri pada saat kencing yang disebabkan oleh proses inflamasi Nokturia : merupakan frekuensi yang terjadi malam hari Normal : orang dewasa tidak terbangun lebih dari 2x semalam untuk miksi Produksi urine pada penderita geriatri meningkat pada malam hari Merupakan efek sekunder dari bladder outlet obstruction dan panurunan daya regang buli

27
Penurunan pancaran kencing
Gejala Obstruksi Penurunan pancaran kencing Merupakan akibat dari bladder outlet obstruction (biasanya oleh BPH atau striktur urethra). Karena prosesnya berjalan perlahan-lahan maka seringkali tidak dikeluhkan oleh penderita. Hesitansi : memerlukan waktu yang lama untuk memulai miksi Intermittensi : proses miksi terputus-putus Post void dribbling : keluarnya urine setelah akhir proses miksi Straining : harus mengejan untuk memulai proses miksi
. Karena prosesnya berjalan perlahan-lahan maka seringkali tidak dikeluhkan oleh penderita. Hesitansi : memerlukan waktu yang lama untuk memulai miksi. Intermittensi : proses miksi terputus-putus. Post void dribbling : keluarnya urine setelah akhir proses miksi. Straining : harus mengejan untuk memulai proses miksi.")
28
Penyakit-penyakit lain yang dapat menimbulkan keluhan iritatif :
Penyakit neurologis (contoh : cerebrovascular accidents, diabetes mellitus dan Parkinson's) Karsinoma buli-buli in situ
 Karsinoma buli-buli in situ.")
29
Inkontinensia Urine Definisi : Keluarnya urine tanpa disadari (involunter) a. Continuous Incontinence Penyebab : fistula traktus urinarius, ektopik ureter b. Stress Incontinence Stress incontinence merujuk pada keluarnya urine secara tiba-tiba pada saat batuk, bersin olahraga atau aktivitas lain yang meningkatkan tekanan intra-abdominal. c. Urgency Incontinence Merupakan keluarnya urine yang disebab dorongan kuat yang mendadak untuk berkemih. Biasanya terjadi pada penderita sistitis, neurogenic bladder atau obstruksi bladder outlet berat dengan hilangnya daya regang buli.

30
d. Overflow Urinary Incontinence /Inkontinensia paradoksal
Merupakan efek sekunder dari retensio urine dan volume residual urine yang tinggi. (terjadi distensi buli secara kronis dan tidak dapat mengosongkan kandung kemih secara tuntas) e. Enuresis Merupakan inkontinensia urine yang terjadi pada waktu tidur. Secara normal terjadi pada anak-anak hingga usia 3 tahun, tetapi tetap ada pada 15% anak usia 5 tahun dan 1 % pada usia hingga 15 tahun ( Forsythe and Redmond, 1974 ). Setiap anak berusia diatas 6 tahun dengan enuresis harus dilakukan pemeriksaan urologis
 e. Enuresis. Merupakan inkontinensia urine yang terjadi pada waktu tidur. Secara normal terjadi pada anak-anak hingga usia 3 tahun, tetapi tetap ada pada 15% anak usia 5 tahun dan 1 % pada usia hingga 15 tahun ( Forsythe and Redmond, 1974 ). Setiap anak berusia diatas 6 tahun dengan enuresis harus dilakukan pemeriksaan urologis.")
31
Pharmacology of Micturition- Increase storage efficiency
Reduce detrusor overactivity Anticholinergic agents- oxybutynine, flavoxate, imipramine Ganglion blocker- bentyl Beta-adrenergic agents Botulinum toxin Vanilloid receptor blockers- capsaicin, resiniferatoxin

32
Pharmacology of Micturition- Increase empty efficiency
Parasympathomimetic agent- Urecholine Adrenergic blockers- inhibition of detrusor relaxation (?)
")
33
Pharmacology of Micturition- Increase outlet resistance
Increase smooth muscle tone Imipramine, methylephedrine Increase striated muscle tone Nitric oxide synthase inhibitor Pelvic floor muscle training

34
Pharmacology of Micturition- Decrease outlet resistance
Decrease bladder neck & urethral resistance Alpha-adrenergic blockers- dibenyline, terazosin, tamsulosin, doxazosin Nitric oxide donors Botulinum toxin Polysynaptic blocker – baclofen, diazepam

Presentasi serupa















>")



