Upload presentasi
Presentasi sedang didownload. Silahkan tunggu

1
Teleconference 12 Program Pra Doktor Résumé, Summary, Rangkuman 6 April 2015 Jam 11:00 -13:00

2
Proses penelitian dimulai dengan suatu topik. Topik dapat mengenai suatu intervensi (e.g., Statin), suatu hasil intervensi (e.g., Pencegahan sekunder penyakit kardiovaskuler), atau keduanya (e.g., Farmakoterapi utk pencegahan sekunder penyakit kardiovaskuler). Berdasarkan topik ini peneliti mengidentifikasi kata-kata kunci dalam Bahasa Inggeris. Contoh: Pharmacotherapy, Cardiovascular Disease, Secondary Prevention.
, suatu hasil intervensi (e.g., Pencegahan sekunder penyakit kardiovaskuler), atau keduanya (e.g., Farmakoterapi utk pencegahan sekunder penyakit kardiovaskuler). Berdasarkan topik ini peneliti mengidentifikasi kata-kata kunci dalam Bahasa Inggeris. Contoh: Pharmacotherapy, Cardiovascular Disease, Secondary Prevention..")
3
Dengan kata2 kunci peneliti mencari makalah Systematic Review (SR) di mesin2 pencari. Cari makalah SR yg seterkini mungkin. Jika makalah SR yg diinginkan belum ditemukan coba terus mencari dengan menggunakan sinonim, thesaurus (Shift F7), pengejaan yg lain, akhiran/awalan, kata2 kunci yg terdapat di bawah abstract makalah2 Penelitian Empirik (PE), judul makalah2 di daftar rujukan.
, pengejaan yg lain, akhiran/awalan, kata2 kunci yg terdapat di bawah abstract makalah2 Penelitian Empirik (PE), judul makalah2 di daftar rujukan..")
4
Hirarki Bukti Sumber: http://www.mededirect.org/faculty.cfmhttp://www.mededirect.org/faculty.cfm

5
Makalah SR memuat hasil critical appraisal (CA) makalah2 PE yg dilacak dan disaring secara sistematis. Biasanya yg diCA adalah makalah2 PE yg menggunakan rancangan experimen murni (RCT), karena validitas dalam dan luar yg tinggi tentang efikasi intervensi.
, karena validitas dalam dan luar yg tinggi tentang efikasi intervensi..")
6
Penafsiran Data Pop Sasaran Pop yg Disampel Sampel Validitas Dalam Inferensi statistik Validitas Luar

7
Untuk menghasilkan kesimpulan yg valid ttg efikasi intervensi, PE juga harus didasarkan atas kerangka konsep yg valid, menggunakan metoda pengumpulan dan pengolahan data yg valid dan dilaksanakan dgn seksama sesuai rencana.

8
Kemungkinan kesimpulan makalah SR: a)Tidak ada makalah PE dgn kesimpulan yg valid PE lebih lanjut dengan rancangan yg lebih baik. b)Ada makalah PE dgn kesimpulan yg valid dan efikasi intervensi bermakna secara praktis/klinis (effect size besar) EBP. c)Jika effect size besar, tetapi tidak bermakna secara statistik replikasi dgn sample size yg lebih besar atau meta-analysis. d)Ada makalah PE dgn kesimpulan yg valid tetapi efikasi intervensi tidak bermakna secara praktis/klinis perbaiki kerangka konsep.
Ada makalah PE dgn kesimpulan yg valid dan efikasi intervensi bermakna secara praktis/klinis (effect size besar) EBP. c)Jika effect size besar, tetapi tidak bermakna secara statistik replikasi dgn sample size yg lebih besar atau meta-analysis. d)Ada makalah PE dgn kesimpulan yg valid tetapi efikasi intervensi tidak bermakna secara praktis/klinis perbaiki kerangka konsep..")
9
Makalah SR seterkini mungkin supaya tidak perlu melacak terlalu jauh ke belakang makalah2 PE yg terbit kemudian. Makalah2 PE yg terbit kemudian mungkin ada yg berhasil memecahkan seluruh/sebagian masalah penelitian Masalah Penelitian & Tujuan Penelitian diperbaharui. Perhatikan metoda SR yg digunakan (utk ditiru saat menulis Bab II) dan nilai mutunya, atau cari makalah SR yg telah direview organisasi yg dapat diandalkan (e.g., The Cochrane Library, HealthEvidence).
 dan nilai mutunya, atau cari makalah SR yg telah direview organisasi yg dapat diandalkan (e.g., The Cochrane Library, HealthEvidence)..")
10
Bab II. Telaah Pustaka Penelitian2 Empirik terkini (sebut metoda telaah pustaka – narrative, scoping, + CA, SR) Konstruk Intervensi/Prediktor Konstruk Hasil Intervensi/Kriterion Landasan Teori, Konstruk Mediator & Konstruk Moderator Kerangka Konsep Hipotesis2 Penelitian.
 Konstruk Intervensi/Prediktor Konstruk Hasil Intervensi/Kriterion Landasan Teori, Konstruk Mediator & Konstruk Moderator Kerangka Konsep Hipotesis2 Penelitian..")
11
Contoh hasil pelacakan makalah SR di Google Scholar (sejak 2015) dgn kata2 kunci: Statin* Systematic Review Gudzune, K. A., Monroe, A. K., Sharma, R., Ranasinghe, P. D., Chelladurai, Y., & Robinson, K. A. (2014). Effectiveness of combination therapy with statin and another lipid- modifying agent compared with intensified statin monotherapy: a systematic review. Annals of internal medicine, 160(7), 468-476. *) Mengatasi hyperlipidemia merupakan pencegahan sekunder penyakit CV.
. Effectiveness of combination therapy with statin and another lipid- modifying agent compared with intensified statin monotherapy: a systematic review. Annals of internal medicine, 160(7), *) Mengatasi hyperlipidemia merupakan pencegahan sekunder penyakit CV..")
12
Purpose: To compare the clinical benefits, adherence, and harms of lower-intensity statin combination therapy with those of higher-intensity statin monotherapy among adults at high risk for atherosclerotic cardiovascular disease (ASCVD). Data Sources: MEDLINE, EMBASE, and the Cochrane Central Register of Controlled Trials from inception to July 2013, with an updated MEDLINE search through November 2013. Study Selection: Randomized, controlled trials published in English. Data Extraction: Two reviewers extracted information on study design, population characteristics, interventions, and outcomes (deaths, ASCVD events, low-density lipoprotein [LDL] cholesterol level, adherence, and adverse events). Two independent reviewers assessed risk of bias.
. Two independent reviewers assessed risk of bias..")
13
Date of download: 4/5/2015 From: Effectiveness of Combination Therapy With Statin and Another Lipid-Modifying Agent Compared With Intensified Statin Monotherapy: A Systematic ReviewEffectiveness of Combination Therapy With Statin Ann Intern Med. 2014;160(7):468-476. doi:10.7326/M13-2526 Summary of evidence search and selection. ASCVD = atherosclerotic cardiovascular disease; CENTRAL = Cochrane Central Register of Controlled Trials; FDA = U.S. Food and Drug Administration; RCT = randomized, controlled trial; SIP = scientific information packet. * Citations could be excluded for >1 reason; therefore, the sum of excluded studies listed from each category may exceed the actual number of citations excluded. Figure Legend: Copyright © American College of Physicians. All rights reserved.American College of Physicians
: doi: /M Summary of evidence search and selection. ASCVD = atherosclerotic cardiovascular disease; CENTRAL = Cochrane Central Register of Controlled Trials; FDA = U.S. Food and Drug Administration; RCT = randomized, controlled trial; SIP = scientific information packet. * Citations could be excluded for >1 reason; therefore, the sum of excluded studies listed from each category may exceed the actual number of citations excluded. Figure Legend: Copyright © American College of Physicians. All rights reserved.American College of Physicians.")
14
Data Synthesis: A total of 36 trials were included. Low-intensity statin plus bile acid sequestrant decreased LDL cholesterol level 0% to 14% more than mid-intensity monotherapy among high-risk hyperlipidemic patients. Mid-intensity statin plus ezetimibe decreased LDL cholesterol level 5% to 15% and 3% to 21% more than high-intensity monotherapy among patients with ASCVD and diabetes mellitus, respectively. Evidence was insufficient to evaluate LDL cholesterol for fibrates, niacin, and ω-3 fatty acids. Evidence was insufficient for long-term clinical outcomes, adherence, and harms for all regimens.

15
Limitation: Many trials had short durations and high attrition rates, lacked blinding, and did not assess long-term clinical benefits or harms. Conclusion: Clinicians could consider using lower-intensity statin combined with bile acid sequestrant or ezetimibe among high-risk patients intolerant of or unresponsive to statins; however, this strategy should be used with caution given the lack of evidence on long-term clinical benefits and harms.

16
Bang, C. N., & Okin, P. M. (2014). Statin treatment, new-onset diabetes, and other adverse effects: a systematic review. Current cardiology reports, 16(3), 1-5. Effek samping Statin: DM, myopathy, rhabdo- myolysis, transaminase meningkat, cataract, mood disorders, dementia, peripheral neuro- pathy, hemorhagic stroke.
, 1-5. Effek samping Statin: DM, myopathy, rhabdo- myolysis, transaminase meningkat, cataract, mood disorders, dementia, peripheral neuro- pathy, hemorhagic stroke..")
17
Finegold, J. A., Manisty, C. H., Goldacre, B., Barron, A. J., & Francis, D. P. (2014). What proportion of symptomatic side effects in patients taking statins are genuinely caused by the drug? Systematic review of randomized placebo-controlled trials to aid individual patient choice. European journal of preventive cardiology, 21(4), 464-474.
. What proportion of symptomatic side effects in patients taking statins are genuinely caused by the drug. Systematic review of randomized placebo-controlled trials to aid individual patient choice. European journal of preventive cardiology, 21(4),")
18
Results Among 14 primary prevention trials (46,262 participants), statin therapy increased diabetes by absolute risk of 0.5% (95% CI 0.1–1%, p = 0.012), meanwhile reducing death by a similar extent: −0.5% (−0.9 to −0.2%, p = 0.003). In the 15 secondary prevention RCTs (37,618 participants), statins decreased death by 1.4% (−2.1 to −0.7%, p < 0.001). There were no other statin- attributable symptoms, although asymptomatic liver transaminase elevation was 0.4% more frequent with statins across all trials. Serious adverse events and withdrawals were similar in both arms.
, statins decreased death by 1.4% (−2.1 to −0.7%, p < 0.001). There were no other statin- attributable symptoms, although asymptomatic liver transaminase elevation was 0.4% more frequent with statins across all trials. Serious adverse events and withdrawals were similar in both arms..")
19
Practical Meta-Analysis -- D. B. Wilson19 Manafsirkan ES Cohen’s “Rules-of-Thumb” – standardized mean difference effect size small = 0.20 medium = 0.50 large = 0.80 – correlation coefficient small = 0.10 medium = 0.25 large = 0.40 – odds-ratio small = 1.50 medium = 2.50 large = 4.30 Sumber: http://mason.gmu.edu/~dwilsonb/downloads/interpretation.ppthttp://mason.gmu.edu/~dwilsonb/downloads/interpretation.ppt

20
Brault, M., Ray, J., Gomez, Y. H., Mantzoros, C. S., & Daskalopoulou, S. S. (2014). Statin treatment and new- onset diabetes: a review of proposed mechanisms. Metabolism, 63(6), 735-745. Mediator2 yg dapat diuji: Certain statins affect insulin secretion through direct, indirect or combined effects on calcium channels in pancreatic β-cells. Reduced translocation of glucose transporter 4 in response to treatment results in hyperglycemia and hyperinsulinemia. Statin therapy decreases other important downstream products, such as coenzyme Q10, farnesyl pyrophosphate, geranylgeranyl pyrophosphate, and dolichol; their depletion leads to reduced intracellular signaling.
. Statin treatment and new- onset diabetes: a review of proposed mechanisms. Metabolism, 63(6), Mediator2 yg dapat diuji: Certain statins affect insulin secretion through direct, indirect or combined effects on calcium channels in pancreatic β-cells. Reduced translocation of glucose transporter 4 in response to treatment results in hyperglycemia and hyperinsulinemia. Statin therapy decreases other important downstream products, such as coenzyme Q10, farnesyl pyrophosphate, geranylgeranyl pyrophosphate, and dolichol; their depletion leads to reduced intracellular signaling..")
21
Proposal = Disertasi – (Hasil, Kesimpulan & Saran) Halaman-Halaman Muka (Halaman judul & Pengesahan, Daftar Isi, Daftar Tabel & Daftar Gambar, Intisari) Bagian Utama: Pendahuluan Telaah Pustaka Metoda Penelitian Rencana Pelaksanaan Hasil, Kesimpulan & Saran Daftar Rujukan Lampiran-Lampiran
 Halaman-Halaman Muka (Halaman judul & Pengesahan, Daftar Isi, Daftar Tabel & Daftar Gambar, Intisari) Bagian Utama: Pendahuluan Telaah Pustaka Metoda Penelitian Rencana Pelaksanaan Hasil, Kesimpulan & Saran Daftar Rujukan Lampiran-Lampiran")
22
Pendahuluan Latar Belakang: Masalah Praktis, Rekam Jejak Masalah Penelitian. Masalah Penelitian. Tujuan Penelitian. Manfaat Penelitian, Keaslian Penelitian.

23
Telaah Pustaka Review Makalah2 PE terkini. Konstruk Intervensi (Prediktor). Konstruk Hasil Intervensi (Kriterion). Kerangka Konsep, Konstruk Mediator, dan Konstruk Moderator Hipotesis Penelitian
. Kerangka Konsep, Konstruk Mediator, dan Konstruk Moderator Hipotesis Penelitian.")
24
24 Moderator Intervensi (Prediktor) Hasil (Kriterion) Mediator V2V2V1 Explanatory Theory F1F3F2 F = Faktor = Dimensi V = variabel atau item Confounding = moderator non-spesifik Action (Predictive) Theory
 Hasil (Kriterion) Mediator V2V2V1 Explanatory Theory F1F3F2 F = Faktor = Dimensi V = variabel atau item Confounding = moderator non-spesifik Action (Predictive) Theory")
25
Metoda Penelitian A.Rancangan Penelitian: 1. Rancangan pengumpulan data. 2. Rancangan pengolahan data. 3. Rancangan penafsiran data. B.Metoda Pengumpulan Data. C.Metoda Pengolahan Data. D.Metoda Penafsiran Data. Operasiona- lisasi dari A

26
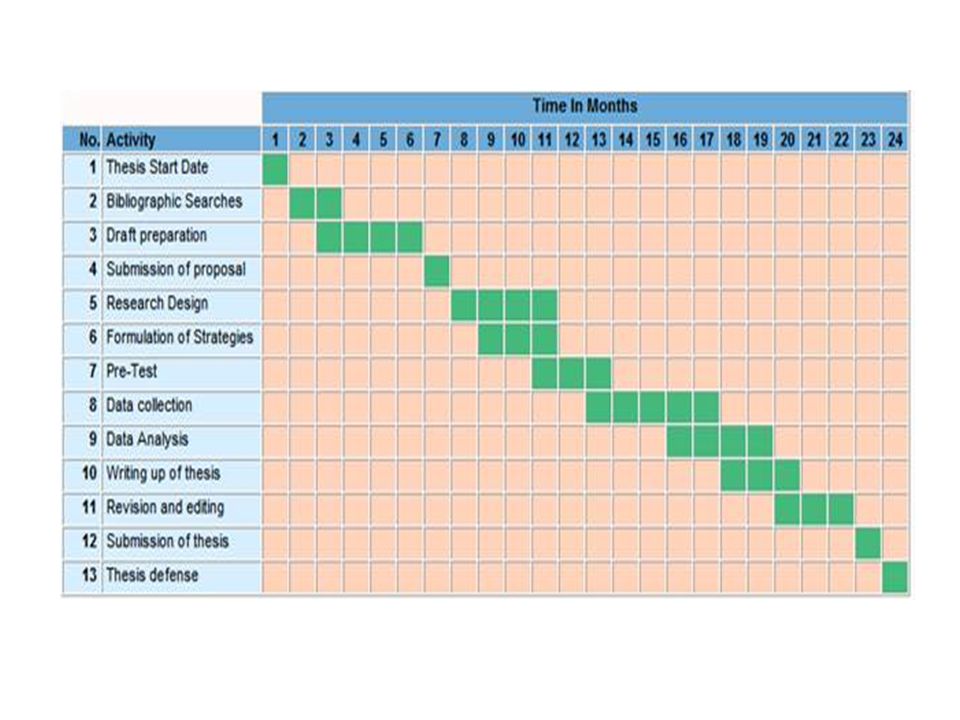
Rencana Pelaksanaan Penelitian Gannt Chart (Waktu, Kegiatan) Anggaran.
 Anggaran.")
Presentasi serupa
 untuk menemukan masalah penelitian. Memperkenalkan telaah pustaka yg melengkapi.>")





>")












